Severe and Very Severe ME
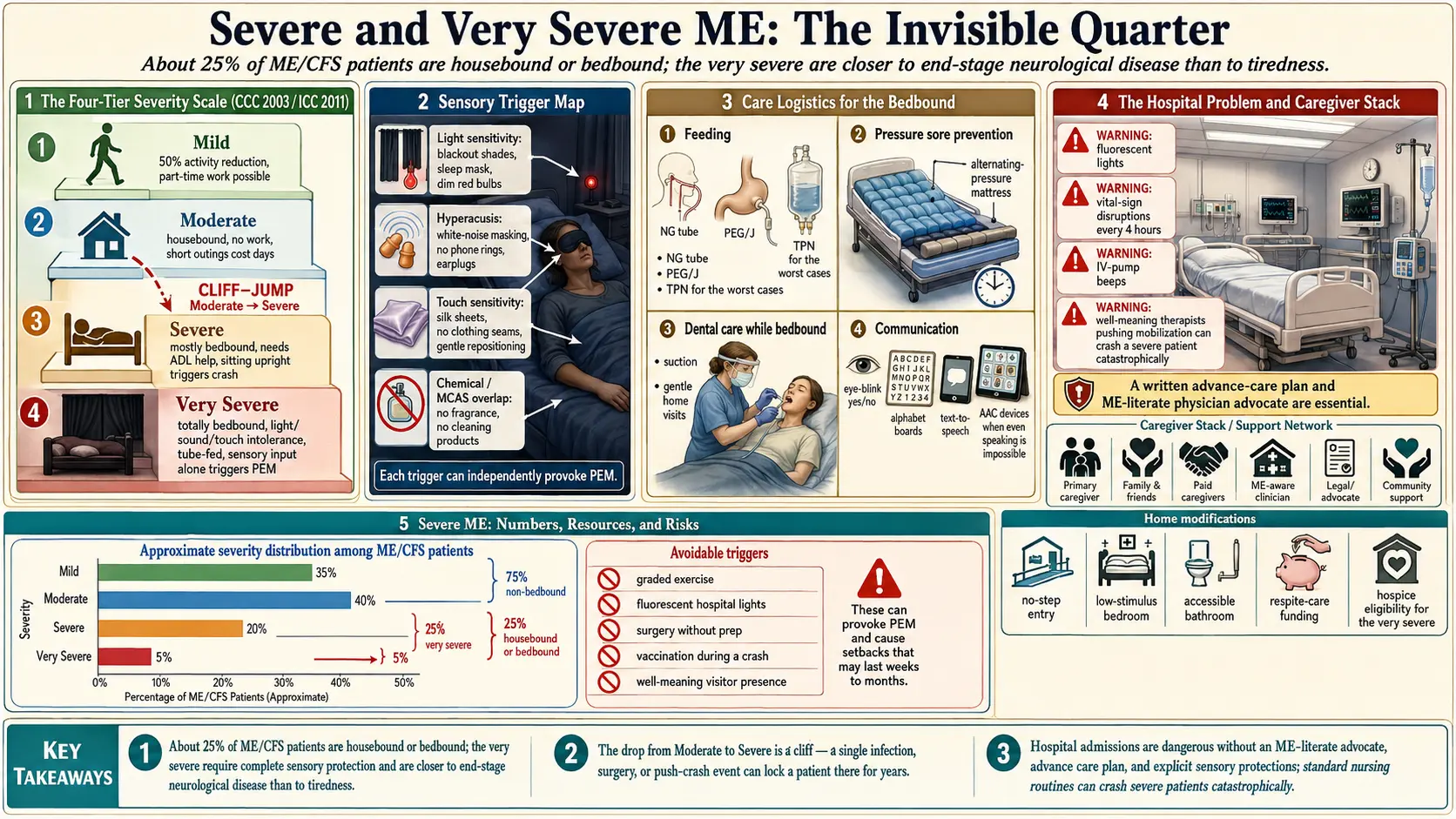
Table of Contents
- Why This Page Exists
- The ME Severity Scale
- How Many People Are This Sick
- Light Sensitivity — Living in the Dark
- Sound Sensitivity and Hyperacusis
- Touch and Chemical Sensitivity
- Cognitive Collapse
- Orthostatic Intolerance So Severe Sitting Crashes You
- Communication When Speaking Is Impossible
- Feeding Challenges — NG, PEG/J, TPN
- Dental Care While Bedbound
- Pressure Sore Prevention
- The Hospital Problem
- Caregivers and Respite
- Whitney Dafoe and Jen Brea: Two Public Faces
- Home Modifications
- When to Move Back With Family
- Disability Applications With Severe ME
- The 25% ME Group and Forward-ME
- Trigger Management — A Daily Protocol
- Key Research Papers
- Connections
- Featured Videos
Why This Page Exists
Most information written about ME/CFS is written for people who can still read it. That leaves the sickest quarter of patients — the severe and very severe — almost invisible. They cannot tolerate a computer screen, a conversation, or sometimes even the light that seeps around a closed door. Their illness is not a more intense version of chronic fatigue. It is a separate crisis, closer to end-stage neurological disease than to tiredness.
This page is written for caregivers, family members, and the rare patient who can have it read aloud a sentence at a time. It is blunt on purpose. Severe ME is not going to be managed out of existence with a better attitude or a graded exercise plan — those approaches harm these patients. What follows is what actually helps, what actually hurts, and what families need to prepare for.
The ME Severity Scale
The 2003 Canadian Consensus Criteria (CCC) drafted by Carruthers and colleagues, and the 2011 International Consensus Criteria (ICC), both use a four-tier severity scale. It is descriptive rather than numeric, and it is the scale the CCC/ICC criteria page walks through in more detail.
- Mild. Approximately 50% reduction in pre-illness activity. Patient can usually work part-time or manage school with heavy compromise, but at the cost of almost all social and leisure activity.
- Moderate. Mostly housebound. Work is no longer possible. Self-care is still feasible with rest. Short outings require days of recovery.
- Severe. Mostly bedbound. Unable to leave the house except in rare circumstances (often medical). Needs help with basic activities of daily living — bathing, dressing, sometimes feeding. Brief time sitting upright produces a crash.
- Very Severe. Totally bedbound. Requires help for all personal care. Often cannot tolerate light, sound, touch, or the presence of another person in the room. May be unable to eat, speak, or turn in bed without assistance. Sensory input alone — a door opening, a phone ringing — can trigger post-exertional malaise.
The jump from moderate to severe is not proportional. It is a cliff. A moderate patient who pushes too hard, catches an infection, or encounters a surgical trigger can drop into severe or very severe in days and stay there for years.
How Many People Are This Sick
Reviews of population cohorts and ME clinic registries consistently estimate that about 25% of ME/CFS patients fall into the severe or very severe categories. That figure appears in the UK Forward-ME coalition's advocacy materials, in Strassheim's 2021 severe-ME review, and in Kingdon's 2020 cohort. Across an estimated 836,000 to 2.5 million Americans with ME/CFS (IOM 2015 estimate), that translates to roughly 200,000 to 600,000 people in the U.S. alone who are bedbound or housebound.
They are absent from the literature for structural reasons. Research studies require patients who can travel to a clinic, sit for an interview, or fill out forms. The severe are, by definition, excluded by that design. When researchers do go to them — home visits, proxy-completed questionnaires — the picture that emerges is consistently worse than the published averages suggest.
Light Sensitivity — Living in the Dark
Severe ME patients commonly develop photophobia that goes far beyond ordinary migraine-level light sensitivity. A thin strip of daylight under a door can trigger a crash. A caregiver checking in with a phone flashlight can leave the patient worse for days.
Practical accommodations that families adopt:
- Blackout blinds plus blackout curtains on every window. The blinds block the bulk of the light; the curtains seal the edges where blinds always leak.
- Tape around door frames with weatherstripping foam, and a rolled towel along the bottom. Corridors outside the room should be kept dim.
- Red-filter night lights (the kind astronomers use) at floor level for caregivers navigating the room. Red light is the least provocative wavelength for most severe ME patients.
- Sunglasses worn indoors, even in a darkened room, during any care interaction. Some patients layer wraparound blackout glasses used for migraine (TheraSpecs, Axon Optics) over ordinary sunglasses.
- Sleep masks for the deepest crashes. A contoured mask that does not press on the eyes is preferable to a flat one.
- Phone and monitor screens kept out of the room. Even a screen flipped face-down leaks light in a dark room.
Sound Sensitivity and Hyperacusis
Hyperacusis in severe ME is not the familiar irritation of a loud restaurant. Normal conversational speech across a room can feel like physical pain. A dishwasher cycling, a dog barking, a toilet flushing two rooms away — any of these can trigger post-exertional malaise.
What helps:
- Silent household rules. No TV, no music, no raised voices anywhere in the home when the patient is in a crash. Phones on silent, notifications off.
- Foam earplugs (Mack's silicone, Hearos, or similar) worn continuously. Some patients layer foam plugs under noise-cancelling over-ear muffs (3M Peltor X5A or Howard Leight) for the quietest combination available without custom hearing protection.
- White-noise machines set to the lowest setting to mask irregular household sounds. Some patients tolerate pink or brown noise better than white. Others cannot tolerate any ambient sound.
- Warn before entering. A soft knock is often louder to the patient than caregivers realize. A simple written protocol — wait, open slowly, speak only if spoken to first — reduces the startle load.
- No visitors without explicit advance coordination. Even well-meaning relatives who "just want to say hello" can crash a very severe patient for weeks.
Touch and Chemical Sensitivity
Many severe patients develop allodynia — normal touch registers as pain — and an overlap with mast cell activation syndrome (MCAS) that turns perfumes, scented laundry detergent, cleaning products, and off-gassing new furniture into medical emergencies.
- Soft, seamless clothing (bamboo, high-thread-count cotton) with tags removed. Compression of any kind is often intolerable.
- Fragrance-free everything. Laundry detergent (All Free Clear, Seventh Generation free), soap, shampoo, lotion, dish soap used by anyone entering the room. Caregivers should not wear perfume, scented deodorant, or scented hair products.
- HEPA air purifier running continuously. A unit rated for a larger room than the patient's actually produces less turbulence on the lowest setting.
- No new furniture, no paint, no new carpets in or near the patient's room. Off-gassing volatile organic compounds from a new mattress alone has put patients into months-long crashes.
- Gentle, pre-announced touch. Caregivers should say "I am going to move your arm now" before every contact. Sudden touch, even loving, can trigger a crash.
Cognitive Collapse
Severe ME often includes cognitive symptoms well beyond ordinary brain fog. Patients describe being unable to follow a single sentence, unable to form words, unable to recognize faces of loved ones during a crash. Reading a text message can produce the same PEM that a flight of stairs produces in a moderate patient.
This is not dementia and it is not psychiatric. It fluctuates with the underlying disease. In better windows some cognition returns. During a deep crash, a patient may know who you are but be unable to produce the word for it. Do not quiz them. Do not ask them to "try harder." Do not interpret silence as indifference.
Orthostatic Intolerance So Severe Sitting Crashes You
The orthostatic intolerance article covers the mechanism. In severe ME, the threshold collapses. A patient who sits up in bed for thirty seconds to sip water can crash for two days. Many cannot tolerate a head-of-bed angle greater than 10 to 20 degrees. Some lie completely flat for years.
Practical adaptations:
- Electric adjustable hospital bed so positioning can be changed in tiny increments without the patient doing the work.
- Straws or hydration pouches (the kind used for hiking bladders) so drinking does not require lifting the head.
- Bed-pan or urinal at the bedside rather than a commode, for the most severe patients. Walking to a bathroom is not an option.
- Overlap with POTS is common. A cardiologist familiar with POTS can sometimes help with fluid loading, electrolytes, or medications (midodrine, fludrocortisone, ivabradine) — but every new medication is a risk in a severely reactive patient and should be started at a fraction of the usual dose.
Communication When Speaking Is Impossible
Many very severe patients lose the ability to speak during crashes. Some lose it permanently. Communication strategies families develop:
- Text only. Even inside the house, requests and answers are exchanged by phone text so the patient can respond without speaking.
- Letter or picture boards for patients who cannot hold a phone. A laminated sheet with common requests (water, bathroom, medication, dark, quiet) that the patient points to.
- Blink codes. One blink for yes, two for no, for the deepest crashes.
- Pre-written medical scripts. Many patients prepare a one-page document describing their condition, their sensory limits, and what they do and do not consent to in an emergency. A caregiver or advocate hands this to any new provider.
Feeding Challenges — NG, PEG/J, TPN
Severe orthostatic intolerance, severe gastroparesis, and sometimes severe oropharyngeal weakness make eating impossible for a subset of patients. The medical interventions escalate in steps.
- Nasogastric (NG) tube. A soft tube through the nose into the stomach. Placed at bedside, usable for weeks. A reasonable first step for an acute inability to eat.
- Percutaneous endoscopic gastrostomy (PEG). A feeding tube surgically placed through the abdominal wall into the stomach. Suitable when the problem is oropharyngeal but the stomach still works.
- PEG-J or jejunostomy (J-tube). Extends past the stomach into the jejunum, bypassing a stomach that cannot empty. Needed when gastroparesis is severe.
- Total parenteral nutrition (TPN). IV nutrition delivered through a central line. A last resort when no part of the GI tract tolerates feeding. Carries significant infection and liver risk and requires specialized home nursing.
These interventions keep patients alive. They are not a failure of will or a sign of giving up. Jen Brea, Whitney Dafoe, and many less-public patients have needed feeding tubes at various points. A gastroenterologist experienced in complex dysmotility is essential; many ME patients have had to educate their own GI teams about the differences between severe ME and standard gastroparesis.
Dental Care While Bedbound
Oral care for bedbound patients is repeatedly overlooked and repeatedly ends in abscesses that require emergency intervention in hospitals the patient cannot tolerate. A realistic protocol:
- Suction toothbrush (the type used for stroke and ICU patients; brands include Sage, Toothette, DenTrust). Allows teeth cleaning without the patient needing to sit up, rinse, or spit.
- Chlorhexidine or xylitol rinses applied with a swab when brushing is not tolerated.
- Dentist home visits. Mobile dental services exist in most U.S. metro areas and are standard in the UK National Health Service for housebound patients. Coverage for examinations and simple extractions can be arranged; more complex work may still require a brief ambulance trip.
- Caregiver training. A hygienist can teach a family member how to do a proper bedside clean in five minutes. Twice a week is better than nothing.
Pressure Sore Prevention
A patient who cannot turn in bed is at serious risk of pressure ulcers within days. Pressure sores in severe ME can become life-threatening because the patient cannot tolerate the sitting-up, wound-clinic, or hospital care that would normally treat them.
- Alternating-pressure air mattress (a Class II medical mattress that inflates cells in rotation) is the single most effective intervention. Many insurers cover these with a physician prescription.
- Repositioning every two hours is the standard of care. For a patient who cannot tolerate handling, an air mattress combined with micro-repositioning (a pillow under one hip for a few hours, then the other) is sometimes all that is possible.
- Heel protectors (soft foam or gel boots) to keep heels off the sheet.
- Daily skin check by a caregiver under dim light, with photographs if needed. A redness that does not blanch is a stage 1 ulcer.
The Hospital Problem
Hospitals are close to the worst environment on earth for a very severe ME patient. Bright fluorescent lights, overhead announcements, beeping monitors, frequent vitals checks, shared rooms, constant staff turnover, and a culture that interprets PEM as deconditioning all combine to crash patients into profoundly worse baselines that can take years to recover — if they recover at all.
If hospitalization becomes unavoidable, families should have prepared in advance:
- An advocacy letter from the patient's ME-literate physician explaining the diagnosis, the severity, the sensory limits, and specific requests: single room, dimmed lights, clustered care (one check every four hours instead of separate visits), no graded mobilization, no "encouragement to get up."
- A one-page summary for the bedside listing every medication, every allergy, every sensory limit, and a clear statement that PEM is real, delayed, and cumulative.
- Advance directives and a healthcare power of attorney. These should specify that severe ME is not a psychiatric illness, that the patient does not consent to forced mobilization or graded exercise therapy, and who speaks for the patient when they cannot.
- Eye masks, earplugs, sunglasses, and the patient's own clothing packed in a go-bag kept near the front door.
- A written request to avoid observation wards and shared rooms, including a willingness to pay out-of-pocket for a private room if insurance will not cover it.
Even with all of this, hospitalization often makes severe ME worse. Families and physicians should weigh every admission carefully and exhaust home-based alternatives first — home IV hydration, home nursing, telehealth consultation.
Caregivers and Respite
Caregivers for very severe ME patients routinely clock 80 to 120 hours of care per week, often for years, often unpaid, often alongside their own job loss, isolation, and health decline. Published surveys (Pendergrast 2016; UK carer surveys) describe rates of caregiver depression, anxiety, and chronic illness that exceed those for caregivers of late-stage cancer or dementia.
Respite planning is not a luxury. It is part of the treatment plan.
- A rotation of at least two trained caregivers. Relying on a single family member eventually breaks both of them.
- Home health aides trained in ME specifics. Most agencies will work with a family-written protocol. A two-hour training visit for a new aide should cover sensory limits, PEM, and the no-visitors rule.
- Mental health care for caregivers by telehealth, with a therapist who understands chronic illness. This is not optional.
- Financial planning early. Severe ME often lasts decades. Long-term-care insurance purchased before diagnosis, disability filings, and family financial structuring need to happen before the caregiver is too exhausted to do them.
Whitney Dafoe and Jen Brea: Two Public Faces
Whitney Dafoe is the son of Stanford geneticist Ron Davis. He has lived with very severe ME for more than a decade, has required feeding tubes, and for years could not tolerate speech, touch, or the presence of another person in his room. His father founded the Open Medicine Foundation and has directed much of his laboratory toward ME research in his son's name. Photographs and essays published with Whitney's consent are among the few public records of what the very severe end of the illness looks like.
Jen Brea is a documentary filmmaker whose 2017 film Unrest was shot largely from her bed. She has described the progression from moderate to severe to bedbound, her use of feeding support, her eventual partial recovery after diagnosis and treatment of craniocervical instability and tethered cord — conditions now recognized as overlapping in a subset of ME patients. Her case is not a template (surgery helped her; it is not appropriate for most patients), but her visibility changed how the illness is discussed.
What both case histories demonstrate: severe ME is not rare, is not new, and is not psychiatric. And public case histories matter because they give isolated patients and families evidence that they are not alone or imagining things.
Home Modifications
A sickroom that works for severe ME is closer to a hospice room than a bedroom.
- Electric adjustable hospital bed with head and foot articulation, side rails, and a remote the patient can reach.
- Alternating-pressure mattress as described above.
- Bedside commode for patients who can manage it, or bedpan and urinal for those who cannot.
- Overhead lift (ceiling track or portable Hoyer) for transfers when the patient cannot tolerate manual lifting. Ceiling-track systems are quieter and more controllable than floor-based lifts, which is a meaningful advantage in a room where any sudden motion matters.
- Hand-held shower with a bench, or bed baths only, depending on tolerance. Many severe patients cannot tolerate sitting upright long enough for a shower and are bed-bathed exclusively.
- Blackout-sealed room as described in the light and sound sections.
- Intercom or baby monitor so a silent patient can summon help without speaking.
- Air purifier, humidifier, thermostat that a caregiver controls from outside the room to avoid extra entries.
When to Move Back With Family
Many severe patients who started the illness as independent adults eventually move back in with parents, siblings, or spouses. This is not defeat. It is the correct medical decision when 24-hour care is required and paid nursing is unaffordable or unavailable.
The honest conversations a family needs to have before the move:
- Who is the primary caregiver, and who relieves them. Without a second person, the system fails within months.
- Which room. A ground-floor room that can be blackout-sealed, near a bathroom, away from kitchen noise, ideally with its own entrance for medical visits.
- Household rules that apply to everyone. Quiet hours (often 24/7), fragrance-free products, no unannounced visitors, children briefed on the patient's limits.
- Financial structure. Disability income, caregiver pay if any, shared costs. Clear agreements prevent resentment.
- The long horizon. Severe ME can last decades. A move that works for six months may not work for six years. Build in review points.
Disability Applications With Severe ME
Severe and very severe ME patients generally qualify for Social Security Disability Insurance (SSDI) in the United States and the equivalent programs in other countries, but the application process is brutal for a patient who cannot tolerate paperwork. Practical guidance:
- File early. Do not wait until the patient can "handle" the paperwork. They may never be able to.
- A third party — a disability attorney or a family member with power of attorney — completes the forms. SSDI explicitly allows this. Most disability attorneys work on contingency (capped at a percentage of backpay), so there is no upfront cost.
- Use CCC or ICC criteria, not the older Fukuda or Oxford criteria. CCC and ICC include post-exertional malaise as required; Fukuda and Oxford do not. Adjudicators increasingly recognize the distinction.
- Include objective evidence where possible. A 2-day CPET is the single most persuasive objective test for PEM, but most severe patients cannot tolerate it. Tilt-table testing, orthostatic vital signs, and documentation of hours-per-day in bed from the treating physician all help.
- Expect denials. Most ME claims are denied at the first level and approved on appeal. Plan for an 18-to-24-month process. A disability attorney familiar with ME is worth their fee.
The 25% ME Group and Forward-ME
The 25% ME Group is a UK-based charity founded specifically for the 25% of patients who are severe or very severe. Their name comes from the severity-distribution estimate. They publish home-visit protocols, hospital-admission letters, caregiver guidance, and written advocacy material aimed at physicians who have never met a severe patient. Their resources are freely downloadable from 25megroup.org and are among the most practical documents in the ME literature.
Forward-ME is a coalition of UK ME charities that convenes around parliamentary engagement and NHS guideline work. Its submissions to the 2021 NICE guideline revision on ME/CFS were instrumental in removing graded exercise therapy from the UK standard of care. For U.S. readers, similar materials are produced by the Open Medicine Foundation, Solve ME/CFS Initiative, and #MEAction.
Trigger Management — A Daily Protocol
A workable daily protocol for a very severe patient, adapted from 25% ME Group materials and common caregiver practice:
- Minimize sensory input by default. Dark, silent, empty room. Exceptions are negotiated in advance, not improvised.
- Cluster care. One entry every four hours for medication, hydration, repositioning, and a skin check. Not four separate entries.
- No visitors without explicit advance coordination including the patient's own written consent. "Just dropping by" is not a neutral act for a very severe patient; it is a medical event.
- Pre-scripted medical communications. A written summary kept at the bedside and another copy kept by the caregiver for phone consultations. The patient should not have to explain their illness to a new provider in a crisis.
- A crash protocol. A written document that specifies what to do when the patient is deeper than baseline: fewer entries, no decisions, no new medications, no visitors, no phone calls, extend the dark/silent period.
- A recovery window protocol. What can be carefully added back (a short text conversation, five minutes of audiobook at low volume, a brief family video call) when the patient signals they are tolerating more. Add one thing at a time, and roll back at the first sign of worsening.
None of this is optional theater. Every item on this list has been the difference, for some family, between stable severe ME and a months-long crash that did not fully resolve.
Key Research Papers
- Pendergrast T, et al. Housebound versus nonhousebound patients with myalgic encephalomyelitis and chronic fatigue syndrome. Chronic Illn. 2016.
- Strassheim V, Newton JL, Collins T. Experiences of living with severe chronic fatigue syndrome/myalgic encephalomyelitis. Medicina (Kaunas). 2021.
- Kingdon C, et al. Health care responsibility and compassion — visiting the housebound patient with severe ME/CFS. Healthcare (Basel). 2020.
- Baxter H, Speight N, Weir W. Reviews of deaths associated with very severe ME — cited cautiously; see primary sources for methodology.
- Carruthers BM, et al. Myalgic encephalomyelitis: International Consensus Criteria. J Intern Med. 2011.
Live PubMed Searches
PubMed searches for further reading on severe and very severe ME:
- Severe myalgic encephalomyelitis
- Very severe ME/CFS and bedbound patients
- ME/CFS hyperacusis and photophobia
- ME/CFS, feeding tubes, and gastroparesis
- ME/CFS caregiver burden and respite
- Hospital admission in severe ME/CFS
- ME/CFS and disability determination
- Canadian Consensus Criteria severity classification
Connections
- ME/CFS Overview
- Post-Exertional Malaise
- ME/CFS Diagnostic Criteria
- 2-Day CPET and Objective Testing
- Orthostatic Intolerance in ME/CFS
- Pacing and the Energy Envelope
- Post-Viral Triggers: EBV and Others
- LDN, Abilify and Experimental Therapies
- Mitochondrial Dysfunction and Energy Metabolism
- POTS
- MCAS
- Fibromyalgia
- Chronic Pain
- Fatigue
- Brain Fog
- Full Body MRI