Brain Fog
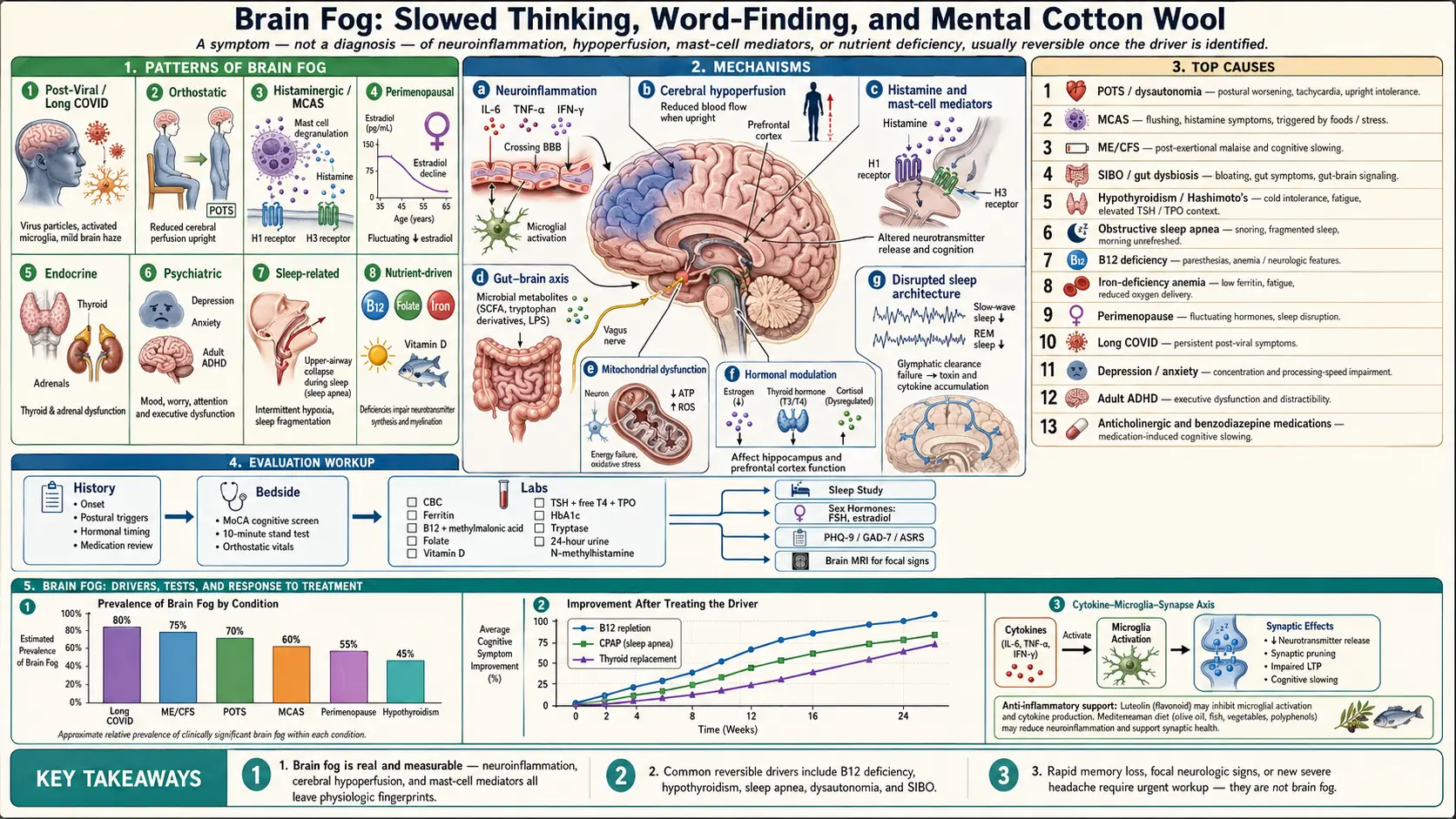


Table of Contents
- Overview
- Patterns of Brain Fog
- Common Causes
- Mechanisms
- Evaluation
- Management
- When to Seek Medical Care
- Connections
- References & Research
- Featured Videos
Overview
Brain fog is the subjective sense of slowed thinking, poor concentration, word-finding difficulty, and short-term-memory lapses without measurable dementia or focal neurologic deficit. It is a symptom, not a diagnosis — the same complaint can reflect post-viral inflammation, autonomic dysfunction, perimenopausal hormonal shifts, mast-cell activation, untreated sleep apnea, B12 deficiency, depression, or any combination. The hallmark is a mismatch: people feel they are thinking through cotton wool while routine cognitive tests look normal. Most brain fog is reversible once the underlying driver is identified and addressed.
Patterns of Brain Fog
- Post-viral / post-infectious — cognitive haze persisting weeks to months after a viral illness, often with fatigue and post-exertional malaise. Overlaps with ME/CFS and dysautonomia.
- Orthostatic — worse on standing, in heat, or after meals; classic in POTS and orthostatic hypotension because of cerebral hypoperfusion.
- Histaminergic / mast-cell — flares with food triggers, alcohol, stress, or hormonal changes; often accompanies flushing, urticaria, GI symptoms.
- Perimenopausal / menopausal — verbal recall and processing speed dip during the menopausal transition and partially recover afterward.
- Endocrine — hypothyroidism, Hashimoto's, adrenal insufficiency, and uncontrolled diabetes all blunt cognition.
- Psychiatric — depression and anxiety produce real, measurable cognitive slowing; ADHD often presents as adult-onset brain fog.
- Sleep-related — obstructive sleep apnea, insomnia, and shift-work disorder degrade attention and consolidation of memory.
- Nutrient-driven — B12, folate, iron, vitamin D, and omega-3 deficiencies all impair cognition.
Common Causes
- POTS and other dysautonomias — standing produces cerebral hypoperfusion and adrenergic surges; brain fog is one of the most disabling symptoms patients report.
- Mast cell activation syndrome (MCAS) — histamine and other mediators cross the blood-brain barrier and disrupt neurotransmission.
- ME/CFS — cognitive impairment is part of the diagnostic criteria; worsens with exertion (post-exertional malaise).
- SIBO and gut dysbiosis — bacterial fermentation produces short-chain fatty acids and gases that influence the gut-brain axis; clearance of overgrowth often resolves brain fog.
- Hypothyroidism and Hashimoto's — even subclinical thyroid disease can produce cognitive complaints.
- Obstructive sleep apnea — intermittent hypoxia degrades attention, memory, and executive function.
- B12 deficiency and folate deficiency — classic causes of cognitive slowing, sometimes with subacute combined degeneration.
- Iron-deficiency anemia — reduced oxygen delivery to the brain.
- Perimenopause and menopause — estrogen withdrawal affects hippocampal function and verbal memory.
- Long COVID and post-viral syndromes — persistent neuroinflammation drives one of the most-reported cognitive complaints in post-acute illness.
- Depression and anxiety — "pseudodementia" of depression and anxiety-driven cognitive narrowing are common and reversible.
- Adult ADHD — under-diagnosed in women; presents with attention and working-memory complaints often labeled "brain fog."
- Medications — anticholinergics, benzodiazepines, opioids, sedating antihistamines, statins, and some chemotherapies cause cognitive impairment.
Mechanisms
- Neuroinflammation — circulating cytokines (IL-6, TNF-alpha, IFN-gamma) cross the blood-brain barrier and activate microglia, blunting synaptic function.
- Cerebral hypoperfusion — in dysautonomia, the brain receives less blood when upright, particularly in the prefrontal cortex.
- Histamine and mast-cell mediators — histamine acts on H1 and H3 receptors in the CNS, modulating arousal and cognition; tryptase and prostaglandins amplify the effect in MCAS.
- Gut-brain axis — vagal signaling, microbial metabolites, and inflammatory tone from the gut all influence cognition; this is why SIBO, IBS, and dysbiosis can present with brain fog.
- Mitochondrial dysfunction — energy supply to neurons drops, particularly in ME/CFS and post-viral states.
- Hormonal modulation — estrogen, thyroid hormone, and cortisol all directly affect hippocampal and prefrontal function.
- Sleep architecture — loss of slow-wave and REM sleep impairs memory consolidation and clearance of waste proteins via the glymphatic system.
Evaluation
- History — onset, triggers (food, posture, hormones), associated fatigue, sleep, mood, medication review.
- Brief cognitive screening — MoCA or similar to rule out true cognitive impairment vs subjective brain fog.
- Bloodwork — CBC, ferritin, B12 with methylmalonic acid, folate, vitamin D, TSH with free T4 and thyroid antibodies, comprehensive metabolic panel, HbA1c.
- Sleep study — if any history of snoring, witnessed apneas, or non-restorative sleep.
- Orthostatic vitals or 10-minute stand test — if symptoms worsen with standing or in heat.
- Tryptase, plasma histamine, 24-hour urine N-methylhistamine — if MCAS features (flushing, urticaria, GI, anaphylaxis history) are present.
- Sex hormones — FSH, estradiol if perimenopausal age and timing fits.
- Mental health screening — PHQ-9, GAD-7, adult ADHD screens (ASRS).
- Brain MRI — if focal deficits, headache pattern change, or rapid progression.
Management
- Treat the driver — thyroid replacement, B12 injections or sublingual cyanocobalamin, iron repletion, CPAP for sleep apnea, SSRI for depression, hormone therapy in menopause when appropriate.
- Reduce inflammation — Mediterranean or anti-inflammatory diet; treat root causes of chronic inflammation (autoimmune, infection, gut dysbiosis).
- Mast-cell stabilization — H1 + H2 antihistamines, cromolyn, low-histamine diet trial in MCAS or histamine intolerance.
- Address dysautonomia — salt and fluid loading, compression garments, recumbent-to-upright exercise progression, beta-blockers or ivabradine if indicated.
- Sleep optimization — consistent schedule, reducing alcohol, screening for and treating sleep-disordered breathing.
- Aerobic exercise — in deconditioning and depression, gentle progressive exercise improves cognition; in ME/CFS, exertion must be carefully paced to avoid post-exertional malaise.
- Cognitive rehabilitation — structured pacing, environmental modifications, written checklists, and rest schedules.
- Stress reduction — mindfulness, gut-directed hypnotherapy, and cognitive-behavioral therapy reduce visceral hypersensitivity and improve attention.
When to Seek Medical Care
- Rapidly progressive memory loss, disorientation to time and place, or personality change.
- New focal neurologic signs (weakness, numbness, vision change, speech difficulty).
- Severe headache that is changing in pattern or accompanied by nausea, vomiting, or vision change.
- Cognitive symptoms with fever, neck stiffness, or confusion (rule out CNS infection).
- Loss of consciousness, seizure, or sudden severe headache.
- Brain fog with depressive symptoms severe enough to cause suicidal thoughts.
Connections
- Depression
- MCAS
- POTS
- Chronic Fatigue Syndrome
- Obstructive Sleep Apnea
- Anxiety
- SIBO
- Vitamin B12
- Thyroid Disorders
- Fatigue
- Iron
- Anemia
- Hashimoto's Thyroiditis
- POTS Subtypes
- POTS/MCAS/EDS Triad
- Headache
- Iodine
- Tryptophan
References & Research
Historical Background
Brain fog was long dismissed as a vague subjective complaint until cytokine research, autonomic testing, and brain imaging in chronic fatigue syndrome, post-viral illness, and mast-cell disease established measurable physiologic correlates. The post-2020 surge in long-COVID cognitive complaints accelerated formal study and produced the first imaging and metabolic signatures of brain fog as a discrete entity rather than a euphemism.
Key Research Papers
- Theoharides TC, Cholevas C, Polyzoidis K, Politis A. Long-COVID syndrome-associated brain fog and chemofog: luteolin to the rescue. BioFactors. 2021;47(2):232-241.
- Komaroff AL, Bateman L. Will COVID-19 lead to myalgic encephalomyelitis/chronic fatigue syndrome? Frontiers in Medicine. 2020;7:606824.
- Ross AJ, Medow MS, Rowe PC, Stewart JM. What is brain fog? An evaluation of the symptom in postural tachycardia syndrome. Clinical Autonomic Research. 2013;23(6):305-311.
- Dantzer R, Heijnen CJ, Kavelaars A, Laye S, Capuron L. The neuroimmune basis of fatigue. Trends in Neurosciences. 2014;37(1):39-46.
- Greene C, Connolly R, Brennan D, et al. Blood-brain barrier disruption and sustained systemic inflammation in individuals with long COVID-associated cognitive impairment. Nature Neuroscience. 2024;27(3):421-432.
- Maki PM, Henderson VW. Cognition and the menopause transition. Menopause. 2016;23(7):803-805.
- Theoharides TC, Stewart JM, Hatziagelaki E, Kolaitis G. Brain fog, inflammation and obesity: key aspects of neuropsychiatric disorders improved by luteolin. Frontiers in Neuroscience. 2015;9:225.
- Stamatelopoulos K, Mengr A, Zoumpoulakis P, et al. Cognitive function in subclinical and overt hypothyroidism. Thyroid Research. 2018;11:14.
- Kaminska M, Mery VP, Lafontaine AL, et al. Cognition in obstructive sleep apnea: meta-analysis of cognitive function in patients with sleep-disordered breathing. Sleep Medicine Reviews. 2017;36:1-13.
- Smith AD, Refsum H. Homocysteine, B vitamins, and cognitive impairment. Annual Review of Nutrition. 2016;36:211-239.
PubMed Topic Searches
- Brain fog pathophysiology
- POTS and cognitive impairment
- MCAS and neuroinflammation
- Long COVID cognitive impairment
- Menopause, cognition, and estrogen
- B12 deficiency and cognition