Orthostatic Intolerance in ME/CFS
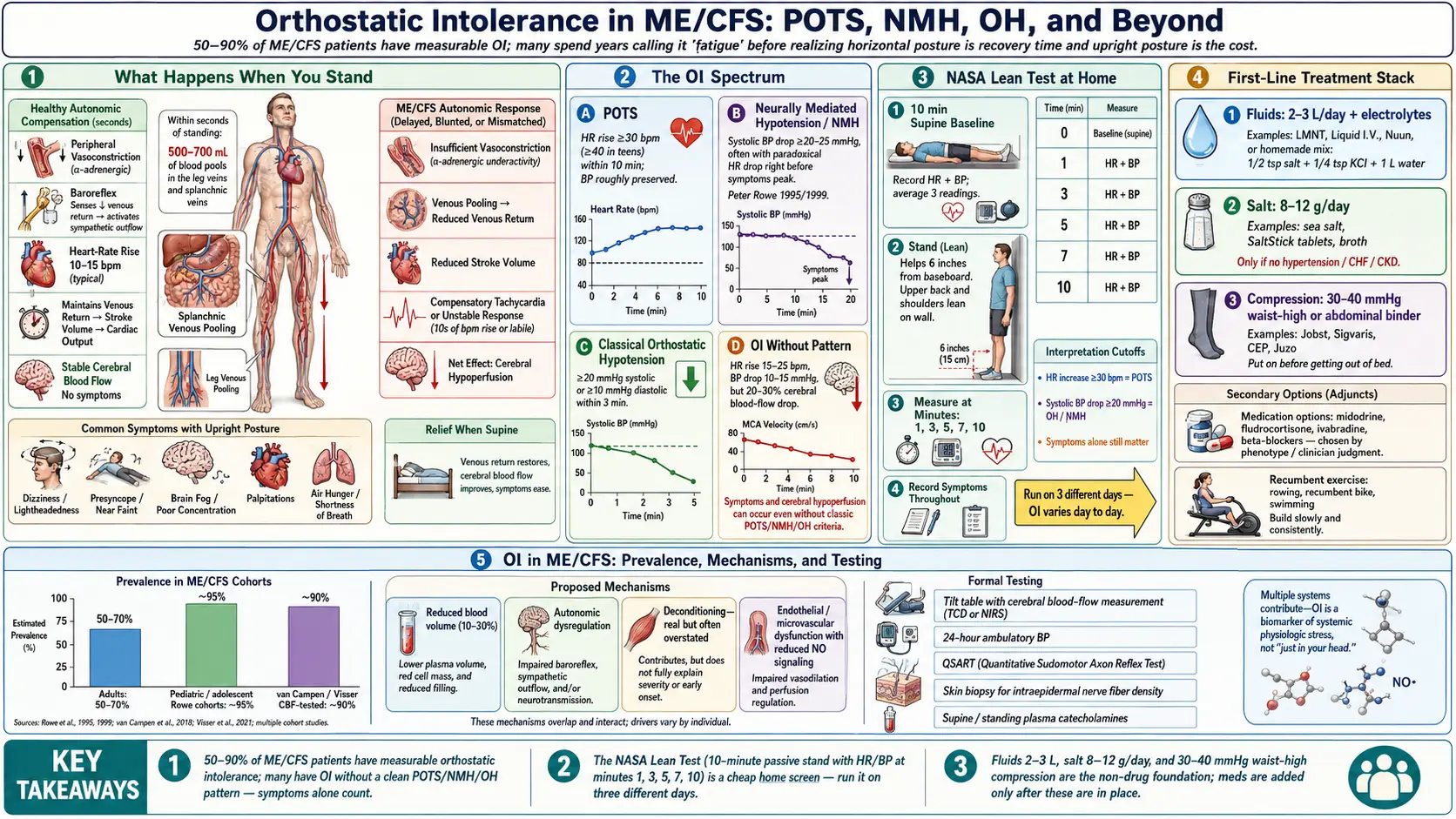
Table of Contents
- What Orthostatic Intolerance Is
- How Common It Is in ME/CFS
- The Spectrum: POTS, NMH, OH, and OI-Without-Pattern
- Why Upright Posture Worsens ME/CFS
- Mechanisms — What Is Actually Going Wrong
- The NASA Lean Test at Home
- Tilt Table, 24-Hour BP, and Other Formal Testing
- First-Line Treatment: Fluids, Salt, Compression
- Medications — What, When, and How Much
- Recumbent Exercise and Why Upright GET Fails
- Practical Tips for Daily Life
- Key Research Papers
- Connections
- Featured Videos
What Orthostatic Intolerance Is
Orthostatic intolerance (OI) is the umbrella term for symptoms that appear or worsen when you stand up and improve when you lie back down. In healthy physiology, standing shifts about 500–700 mL of blood into the legs and splanchnic veins within the first few seconds. The autonomic nervous system answers by tightening blood vessels and nudging heart rate up by 10–15 beats per minute, keeping brain perfusion steady. In orthostatic intolerance, that response is broken, overshoots, or simply never comes — and the brain ends up underperfused.
The symptoms are what you would expect from a brain that is not getting enough blood: lightheadedness, brain fog, blurred vision, fatigue that gets dramatically worse the longer you stand, racing or pounding heart, nausea, shakiness, and sometimes fainting. In ME/CFS the picture is even messier, because the fatigue, cognitive fog, and post-exertional malaise of the underlying illness blur the edges of the OI syndrome. Many patients spend years describing “fatigue” without realizing that a huge fraction of it is driven by the act of staying upright.
How Common It Is in ME/CFS
Depending on the criteria used and whether testing is passive (lean test, tilt table) or symptom-based, 50–90% of ME/CFS patients have measurable orthostatic intolerance. Pediatric and adolescent cohorts skew toward the higher end — studies from Peter Rowe at Johns Hopkins have consistently found that nearly all teenagers with ME/CFS develop OI on tilt testing. Adult cohorts trend lower, but in the large cohort studied by van Campen and Visser in the Netherlands, 90% of ME/CFS patients developed abnormal cerebral blood flow on tilt testing even without meeting heart-rate or blood-pressure criteria for POTS or orthostatic hypotension.
The practical takeaway: if you have ME/CFS and have never been evaluated for OI, the odds are very high that you have it. And if you have it and do not know, you are almost certainly trying to manage the illness with a broken leg you have never bothered to set.
The Spectrum: POTS, NMH, OH, and OI-Without-Pattern
Orthostatic intolerance is not one thing. It is a family of patterns on the same axis, and ME/CFS patients can sit anywhere on it — or can show more than one pattern across different days. The four main categories:
Postural Orthostatic Tachycardia Syndrome (POTS). Heart rate rises by at least 30 beats per minute (40 bpm in adolescents) within 10 minutes of standing, without a meaningful drop in blood pressure. Standing HR typically hits 120 bpm or higher. Patients feel racing heart, lightheadedness, air hunger, shaking, and overwhelming fatigue. See the dedicated POTS page for the deeper clinical picture.
Neurally Mediated Hypotension (NMH). Also called neurocardiogenic syncope or vasovagal syndrome in its faintier form. Blood pressure drops by at least 20–25 mmHg systolic (or below 90 mmHg absolute) during prolonged upright posture, often with a paradoxical drop in heart rate right before symptoms peak. NMH tends to produce delayed symptoms — you feel fine for 10, 20, 30 minutes, then suddenly sweaty, nauseous, foggy, and about to fall over. Peter Rowe’s landmark 1995 and 1999 studies established NMH as a major OI pattern in ME/CFS, sometimes more common than POTS in adults.
Classical Orthostatic Hypotension (OH). Sustained drop of 20 mmHg systolic or 10 mmHg diastolic within 3 minutes of standing. Less common in ME/CFS than POTS or NMH. When present, it tends to point toward autonomic neuropathy, medication effects, or severe dehydration rather than primary ME/CFS physiology.
Orthostatic intolerance without a defined pattern. The most common and most underdiagnosed category. Heart rate rises only 15–25 bpm. Blood pressure drops 10–15 mmHg. Neither number hits the diagnostic cutoff. But the patient’s symptoms — cognitive fog, leg heaviness, fatigue, breathlessness — appear only upright and vanish supine. Cerebral blood flow measurements during tilt show 20–30% reductions in these patients even when HR and BP look normal. If you have been told your tilt test was “negative” but you still can’t tolerate standing, this is very likely what you have.
Why Upright Posture Worsens ME/CFS
Every ME/CFS patient eventually notices the same thing: the day gets worse as it goes on, and horizontal time is recovery time. This is not an accident of mood or effort. It is biology.
When you stand, blood pools in dependent veins. In a healthy person the nervous system compensates in seconds. In ME/CFS the compensation is sluggish, incomplete, or wrong, and cerebral blood flow drops. Reduced cerebral blood flow is not a theory — it has been measured directly with transcranial Doppler and extracranial Doppler ultrasound by the van Campen/Visser group and by Medow and Stewart’s lab at New York Medical College. The brain starves, and the symptoms we call “brain fog,” “cognitive fatigue,” and even “post-exertional malaise” in part reflect that ongoing hypoperfusion.
There is also a feedback loop. Upright posture in an OI patient provokes sympathetic overactivation — adrenaline surges to try to compensate — which itself feels awful (racing heart, tremor, sweating, anxiety) and consumes ATP at a cellular level. In ME/CFS, where cellular energy production is already impaired, every hour upright is an energy debt you cannot easily repay. That is why many moderately affected patients can function for two or three hours upright and then collapse for the rest of the day.
Mechanisms — What Is Actually Going Wrong
There is no single cause of OI in ME/CFS. Four mechanisms overlap in most patients.
1. Low blood volume (hypovolemia). Multiple studies have found ME/CFS patients carry 10–30% less circulating blood volume than healthy controls, with red cell mass and plasma volume both reduced. Less blood in the tank means less to spare when gravity pulls it south. This is one reason fluid and salt loading is a first-line treatment — you are literally refilling the tank.
2. Autonomic dysfunction. The autonomic nervous system — the part that runs blood vessels, heart rate, digestion, and sweat without your conscious input — is dysregulated in ME/CFS. Some vessels fail to constrict on demand. Others constrict inappropriately. Sympathetic tone is often high at rest and paradoxically low when needed. Small-fiber neuropathy is found in a meaningful subset and may contribute.
3. Deconditioning (real, but overstated). Yes, months or years of being horizontal weakens the muscle pump in the legs and reduces cardiac stroke volume. But deconditioning alone does not explain why an acute viral illness can flip a previously athletic person into severe OI overnight. Deconditioning is a contributor, not the driver. Treating it as the driver — the error at the heart of graded exercise therapy — is what makes patients worse, not better.
4. Endothelial and microvascular dysfunction. Newer work suggests that the small blood vessels themselves behave abnormally in ME/CFS, with reduced endothelial nitric oxide signaling and impaired flow-mediated dilation. This may overlap with the post-viral endothelial injury seen after other acute infections.
The NASA Lean Test at Home
You do not need a tilt table to get the first useful answer. The NASA Lean Test (also called the 10-minute stand test) is a protocol you can run at home with a basic blood-pressure cuff and a watch. It was originally developed to assess orthostatic tolerance in astronauts returning from spaceflight and is now the workhorse screening tool for OI in ME/CFS and POTS clinics.
Protocol.
- Lie flat on your back for 10 minutes. Do nothing. At the end, record HR and BP three times, one minute apart, and average them. This is your supine baseline.
- Stand up. Lean your upper back against a wall with your heels about 6 inches (15 cm) from the baseboard. Do not move your legs. Do not shift weight. The lean minimizes the muscle-pump effect that masks OI during active standing.
- At minutes 1, 3, 5, 7, and 10, record HR and BP. Note any symptoms — lightheadedness, visual changes, cognitive slowing, chest tightness, nausea.
- Stop early and lie down at any point if you feel faint, have tunnel vision, or start to lose awareness. Symptoms count even if numbers do not.
Interpretation. Calculate maximum HR rise over baseline and maximum BP drop over baseline. A HR rise of 30+ bpm (40+ in teens) suggests POTS. A systolic BP drop of 20+ mmHg (or 25+ for NMH criteria) or a diastolic drop of 10+ mmHg suggests orthostatic hypotension or NMH. Symptoms alone, with smaller numeric changes, still count as orthostatic intolerance. Bring the sheet to your doctor.
Run the test on three different days if you can. OI is notoriously day-to-day variable — salt intake, sleep, menstrual cycle phase, and hydration all move the numbers. A single negative test with clear symptoms should not reassure anyone.
Tilt Table, 24-Hour BP, and Other Formal Testing
Tilt table testing is the formal version. You lie strapped to a motorized table that tilts to 60–70 degrees upright for 30–45 minutes while HR and BP are recorded continuously. Some centers add cerebral blood flow measurement via transcranial Doppler or extracranial Doppler — this is the single biggest diagnostic advance in OI in the last decade and the only way to catch the OI-without-pattern group. Ask the center directly whether they measure cerebral blood flow; most community cardiology practices do not.
Pursue tilt testing if the home lean test is equivocal, if you are considering medications, or if an insurance carrier or disability application demands an objective result. The test is uncomfortable — some ME/CFS patients are knocked out for weeks by the provocation — so weigh the cost against what the answer will change.
24-hour ambulatory blood pressure monitoring catches patterns the clinic misses: non-dipping at night, morning surges, paradoxical hypertension, and “white coat” normal readings that hide everyday OI. Useful when symptoms do not match the in-office numbers.
Other adjuncts: QSART (quantitative sudomotor axon reflex testing) for small-fiber neuropathy, skin biopsy for intraepidermal nerve fiber density, and plasma catecholamines (supine and standing) when hyperadrenergic POTS is suspected.
First-Line Treatment: Fluids, Salt, Compression
Before any prescription, these three non-drug interventions are the foundation. They are cheap, broadly safe, and meaningfully effective for most patients. Skipping them and jumping to medications is a common mistake.
Fluids: 2–3 liters per day. Plain water is not enough — without sodium to hold it in the vasculature, extra water is simply urinated out. Target 2–3 L of fluid, with most of it paired with salt. Electrolyte mixes (LMNT, Liquid I.V., Nuun, or a homemade recipe of ½ tsp salt + ¼ tsp potassium chloride + 1 L water) work well. Spread intake through the day; chugging 2 L at once triggers a diuresis and wastes the effort.
Salt: 8–12 grams per day. That is 3–5 times the average Western intake and can feel absurd the first week. Use sea salt in cooking, salt all meals aggressively, add salt tablets (SaltStick, Thermotabs, 1 g each) if taste tolerance is limited, and broth or bouillon between meals. This is only appropriate if you do not have hypertension, heart failure, or kidney disease, and ideally under medical supervision. Blood pressure should be monitored during ramp-up. Most OI patients run chronically low-normal BP and handle the salt load without trouble.
Compression: 30–40 mmHg, waist-high. Knee-high compression is not enough. The blood that pools during standing pools mostly in the splanchnic veins of the abdomen and the large veins of the thighs, not the calves. Effective compression therefore needs to reach at least thigh-high, and ideally includes abdominal binders or waist-high pantyhose at 30–40 mmHg. Brands patients consistently recommend: Jobst, Sigvaris, CEP, and the medical-grade Juzo. Put them on before getting out of bed — once you are upright and pooling, pulling them on is a wrestling match and half the benefit is lost.
Medications — What, When, and How Much
Non-drug foundations first. If symptoms remain disabling after 4–8 weeks of consistent salt, fluid, and compression, medications are the next step. No single drug works for everyone; the choice depends on which physiological pattern is dominant. A specialist — a dysautonomia cardiologist, autonomic neurologist, or ME/CFS-experienced internist — is the right prescriber.
Fludrocortisone (Florinef). A mineralocorticoid that tells the kidneys to retain sodium and water, expanding blood volume. Typical dose 0.05–0.2 mg once daily in the morning. Useful for NMH, POTS with low blood volume, and classical OH. Common side effects: headache, leg swelling, low potassium (supplement with a banana or prescription KCl), and a small increase in BP that can be beneficial. Weeks are required for full effect.
Midodrine (ProAmatine). An alpha-1 agonist that directly constricts blood vessels. Typical dose 2.5–10 mg three times daily, timed to active hours — first dose on rising, then every 3–4 hours, with the last dose at least 4 hours before bed to avoid supine hypertension. The effect is fast (30–60 minutes) and short (3–4 hours). Side effects: scalp tingling (a signature), piloerection, and urinary retention. Good for POTS and NMH where vasoconstriction is the missing piece.
Low-dose propranolol. A non-selective beta blocker. Typical dose 10–20 mg two to four times daily. Counterintuitive — you would think slowing the heart in a patient whose HR already runs high would worsen the situation — but in POTS and hyperadrenergic patterns, low-dose propranolol reduces the sympathetic surge that drives symptoms and often improves both HR and subjective tolerance. Start very low (2.5–5 mg) in ME/CFS; some patients are exquisitely sensitive.
Ivabradine (Corlanor). Selectively slows the sinus node without affecting BP or contractility. Typical dose 2.5–7.5 mg twice daily. Increasingly the preferred choice for pure POTS — it lowers HR without the fatigue that beta blockers cause in some patients. Expensive and often requires prior authorization; generic availability is expanding.
Pyridostigmine (Mestinon). An acetylcholinesterase inhibitor originally used in myasthenia gravis. Typical dose 30–60 mg two to three times daily. Boosts parasympathetic tone, modestly lowers standing HR, and for many ME/CFS patients also improves fatigue and muscle endurance — a useful dual action. Side effects: cramping, loose stools, excess saliva; often dose-limiting.
Droxidopa (Northera). A synthetic norepinephrine precursor used mainly for neurogenic orthostatic hypotension. Typical dose 100–600 mg three times daily. Expensive and usually insurance-restricted; best reserved for patients who fail midodrine and have documented OH on testing.
Desmopressin (DDAVP). For selected patients with pronounced diuresis-driven symptoms. Used intermittently — not daily — because of hyponatremia risk. A specialist’s call.
A note on timing. Most OI medications have narrow therapeutic windows and interact. It is entirely normal to need a combination — e.g., fludrocortisone daily to expand volume, midodrine three times a day to constrict vessels, and low-dose propranolol to rein in sympathetic surges. Work with one prescriber to keep the regimen coherent.
Recumbent Exercise and Why Upright GET Fails
Patients with ME/CFS have been harmed for decades by well-meaning physical therapists prescribing graded exercise therapy (GET) — the steady upward push of upright aerobic exercise, on the theory that deconditioning is the driver. In ME/CFS with OI, upright GET attacks exactly the posture the patient cannot tolerate. It provokes post-exertional malaise, worsens cerebral hypoperfusion, and pushes many patients from moderate into severe disease. The 2021 NICE guidelines formally removed GET as a recommended treatment for this reason, and the CDC has done the same.
What can help is recumbent reconditioning done within a tight energy envelope (see pacing and the energy envelope). The protocol most commonly cited is CHOP’s (Children’s Hospital of Philadelphia) modified Dallas Protocol: start with a recumbent bike or rowing machine, or floor-based exercises like leg lifts and bridges, for 2–5 minutes at a time, two or three times a week. Keep heart rate well below the anaerobic threshold identified on 2-day CPET (typically HR < 110 bpm in deconditioned adults). Only progress when the current level is tolerated without post-exertional malaise for two full weeks. Many patients never progress past recumbent work, and that is fine — recumbent fitness is still fitness.
The key reframe: exercise in ME/CFS is not about deconditioning reversal. It is about protecting what autonomic function remains without triggering a crash.
Practical Tips for Daily Life
A short list of moves that cost nothing and help most OI patients immediately.
- Elevate the head of your bed 4–6 inches. Wooden blocks under the head-end bedposts, not just extra pillows. Sleeping head-up trains the kidneys to retain more sodium overnight and reduces the morning BP drop. This one trick alone buys many patients an extra hour of functional morning time.
- Cross-leg standing. In line at the store or on a platform, cross one leg tightly in front of the other and squeeze. The muscle contraction pushes venous blood upward. Widely used by trained vocalists and flight attendants for the same reason.
- Squatting. When presyncope hits, drop into a full squat rather than sitting. Squatting mobilizes far more venous blood back into circulation than sitting and aborts many near-faint episodes in seconds.
- Counter-maneuvers. Clench buttocks and thigh muscles for 30 seconds, hand-grip an object tightly, or tense abdominal muscles. These isometric contractions raise BP acutely — useful when you feel symptoms coming and cannot sit down yet.
- Eat small and often. Large meals divert blood to the gut and worsen postprandial OI. Six small meals beat three large ones for most patients.
- Avoid hot environments. Hot showers, saunas, hot yoga, and midday summer heat all dilate peripheral vessels and drop BP. Warm showers not hot, mornings not afternoons.
- Alcohol and cannabis both worsen OI. Both vasodilate. The “one glass of wine” that used to be harmless may now knock you horizontal for the evening.
- Track, don’t guess. A cheap home BP cuff plus a wrist heart-rate strap used a few times a week will tell you whether your regimen is working better than any symptom diary alone.
Key Research Papers
- Rowe PC, Calkins H, et al. Fludrocortisone acetate to treat neurally mediated hypotension in chronic fatigue syndrome: a randomized controlled trial. JAMA. 1999;282(18):1781–1788.
- Stewart JM. Orthostatic intolerance in pediatrics. Pediatrics. 2004.
- van Campen CLMC, Verheugt FWA, Rowe PC, Visser FC. Cerebral blood flow is reduced in ME/CFS during head-up tilt testing even in the absence of hypotension or tachycardia: a quantitative, controlled study using Doppler echography. Healthcare. 2020;8(3):210.
- Rowe PC. General information brochure on orthostatic intolerance and its treatment. Front Pediatr. 2014;2:64.
Live PubMed Searches
The following PubMed topic searches return current peer-reviewed work on orthostatic intolerance in ME/CFS, POTS, and autonomic dysfunction:
- Orthostatic intolerance and chronic fatigue syndrome
- POTS and ME/CFS overlap
- Neurally mediated hypotension in ME/CFS
- Cerebral blood flow during tilt testing in ME/CFS
- Blood volume and hypovolemia in ME/CFS
- Fludrocortisone for orthostatic intolerance
- Midodrine for POTS and orthostatic intolerance
- Ivabradine in postural tachycardia syndrome
- Pyridostigmine for autonomic orthostatic symptoms
- NASA lean test for orthostatic intolerance
- Compression garments in orthostatic intolerance
Connections
- ME/CFS Overview
- POTS
- POTS Subtypes
- Tilt-Table and NASA Lean Test
- Salt and Hydration Protocol
- POTS Medications Guide
- 2-Day CPET and Objective Testing
- Pacing and the Energy Envelope
- Post-Exertional Malaise
- Severe and Very Severe ME
- Post-Viral Triggers: EBV and Others
- ME/CFS Diagnostic Criteria
- LDN, Abilify and Experimental Therapies
- Mitochondrial Dysfunction and Energy Metabolism
- MCAS
- Fibromyalgia
- Lightheadedness
- Fatigue
- Mast Cell Activation Syndrome (MCAS)
- Fibromyalgia
- Post-Exertional Malaise Explained
- 2-Day CPET and Objective Testing
- Pacing and the Energy Envelope
- Severe and Very Severe ME