IOM/SEID vs CCC vs ICC: ME/CFS Diagnostic Criteria Compared
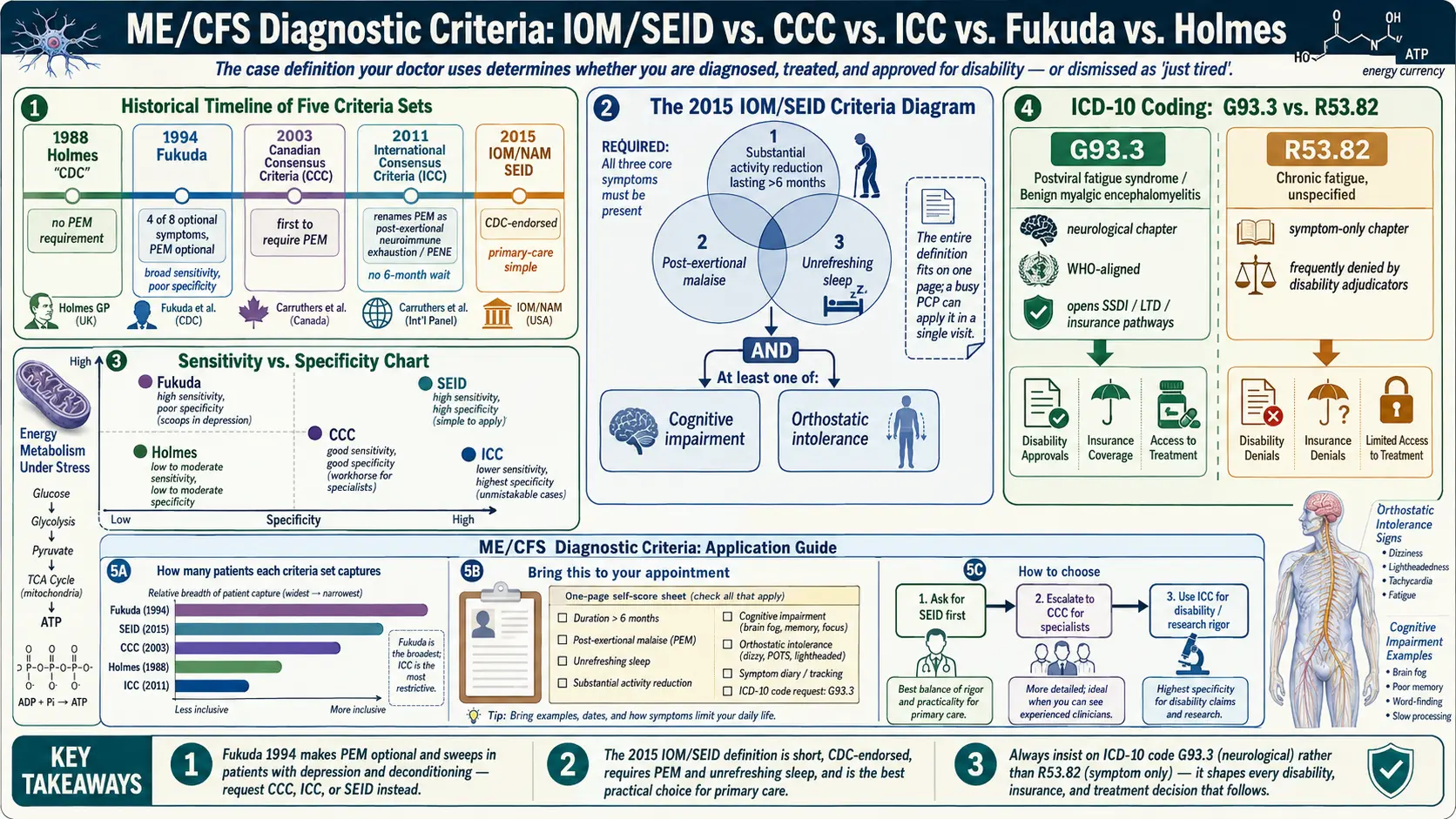
Table of Contents
- Why the Criteria You Are Diagnosed Under Matters
- Holmes 1988 — The First Case Definition
- Fukuda 1994 — The Most Widely Used (and Most Criticized)
- Canadian Consensus Criteria (CCC) 2003
- International Consensus Criteria (ICC) 2011
- IOM/NAM 2015 — SEID and the Push Into Primary Care
- Side-by-Side: Sensitivity, Specificity, and What Each One Misses
- How to Use a Self-Score Sheet Before Your Appointment
- Talking to a Skeptical Primary Care Physician
- ICD-10 Coding: G93.3 vs R53.82 and Why It Matters
- Which Criteria Should You Ask to Be Evaluated Under?
- Key Research Papers
- Connections
- Featured Videos
Why the Criteria You Are Diagnosed Under Matters
If you have been sick for months or years with crushing fatigue, brain fog, and a body that punishes you for every step you take, you may have noticed something odd: two doctors can look at the same patient and disagree about whether that patient has ME/CFS. One will say yes. The other will shrug and call it "chronic fatigue" or "deconditioning" or "depression with somatic features." They are not necessarily incompetent. They are often using different case definitions.
Over the last forty years, at least five major sets of criteria have been published for what we now usually call myalgic encephalomyelitis / chronic fatigue syndrome (ME/CFS). Each set defines the illness differently, captures a different slice of patients, and produces different estimates of how common the disease is. Under one definition your illness counts. Under another it does not. That single fact determines whether you get treated, whether you qualify for disability, whether your insurance covers workup, and whether your family believes you are really sick.
This article walks through the five big criteria sets in the order they were written, explains the trade-offs of each, and gives you a practical way to prepare for an appointment so the doctor across from you can apply them correctly. No criteria set is perfect. But some are far better than others at catching what you actually have.
Holmes 1988 — The First Case Definition
The first formal U.S. case definition came out of the Centers for Disease Control in 1988, led by Gary Holmes. The context matters: in the mid-1980s, clusters of mysteriously exhausted patients were being reported around Lake Tahoe, Nevada, and Lyndonville, New York. Journalists dubbed it "yuppie flu." The CDC needed a research definition so epidemiologists could count cases. Holmes and colleagues called the illness chronic fatigue syndrome — a name many patients now consider demeaning, but one that stuck.
The Holmes definition required at least six months of debilitating fatigue that reduced daily activity by at least 50%, plus a long checklist of minor symptoms (sore throat, tender lymph nodes, low-grade fever, muscle pain, joint pain, sleep disturbance, neuropsychological complaints, headaches) and strict exclusions for other medical and psychiatric disease.
It was a research definition, not a clinical one. It missed patients whose fatigue was severe but who did not hit the minor-symptom count, and it completely failed to require the single most defining feature of the illness: post-exertional malaise (PEM). Nobody in 1988 fully understood PEM yet. Holmes was the starting line, not the finish.
Fukuda 1994 — The Most Widely Used (and Most Criticized)
In 1994 the CDC released a revised definition authored by Keiji Fukuda, Stephen Straus, and colleagues. Fukuda 1994 became the dominant criteria set for research studies worldwide for the next two decades, and it is still the one many older primary care physicians learned in training.
Fukuda requires:
- Clinically evaluated, unexplained, persistent or relapsing chronic fatigue of new or definite onset (not lifelong), lasting at least six months, not the result of ongoing exertion, not substantially relieved by rest, and causing substantial reduction in previous levels of activity.
- Four or more of eight symptoms, present for at least six months: impaired memory or concentration, sore throat, tender cervical or axillary lymph nodes, muscle pain, multi-joint pain without swelling, new headaches, unrefreshing sleep, and post-exertional malaise lasting more than 24 hours.
Here is the central problem: in Fukuda, PEM is one of eight optional symptoms. A patient can meet Fukuda criteria without having PEM at all, as long as they have enough of the other symptoms. That matters enormously, because PEM — the worsening of all symptoms after minor physical, cognitive, or emotional exertion, often delayed 24–72 hours — is the single feature that distinguishes ME/CFS from depression, deconditioning, burnout, and almost every other fatiguing illness.
Leonard Jason and colleagues at DePaul University showed in multiple studies that Fukuda is so broad it scoops up patients with major depressive disorder who do not have ME/CFS at all. Treatment trials recruited under Fukuda often include a mixed population, which is one reason graded-exercise-therapy studies produced results that harmed real ME/CFS patients: many of the "responders" in those trials may not have had ME/CFS in the first place.
Fukuda is too sensitive and not specific enough. If your doctor is still diagnosing by Fukuda, you are being evaluated with a 1994 ruler that measures the wrong thing.
Canadian Consensus Criteria (CCC) 2003
In 2003, an international panel led by Canadian physicians Bruce Carruthers and Anil van de Sande published what became known as the Canadian Consensus Criteria. Unlike Holmes and Fukuda, CCC was built as a clinical (not just research) definition, and it was the first major criteria set to put PEM as a required symptom, not an optional one.
To meet CCC, a patient must have:
- Fatigue — significant, new, persistent, and substantially reducing activity.
- Post-exertional malaise and/or fatigue — required, with a pathologically slow recovery period (usually more than 24 hours).
- Sleep dysfunction — unrefreshing sleep, reversed or disrupted sleep rhythms.
- Pain — myalgias, arthralgias, headaches of a new type.
- Two or more neurological/cognitive manifestations — confusion, impaired concentration, short-term memory problems, disorientation, difficulty processing information, word-finding problems, sensory overload.
- At least one symptom from two of three categories: autonomic (orthostatic intolerance, palpitations, lightheadedness), neuroendocrine (temperature dysregulation, loss of thermostatic stability, anorexia or abnormal appetite, weight change), and immune (recurrent flu-like symptoms, sore throat, tender lymph nodes, new sensitivities to foods or chemicals).
- Illness persists at least six months.
CCC is sharper. Studies by Jason's group showed it identifies a more homogeneous, more impaired patient group with clearer biological abnormalities than Fukuda. The trade-off is that it is longer to apply in clinic and requires the physician actually to know what PEM is and how to ask about it.
International Consensus Criteria (ICC) 2011
In 2011, a larger international panel — again led by Carruthers — published the International Consensus Criteria. The ICC was deliberately stricter than CCC and, in an act of clinical politics, dropped the name "chronic fatigue syndrome" entirely. The authors argued the illness should be called what the World Health Organization had already classified it as since 1969: myalgic encephalomyelitis.
ICC requires:
- Post-exertional neuroimmune exhaustion (PENE) — a renamed, more rigorous PEM requirement, treated as the cardinal symptom. Rapid physical and/or cognitive fatigability in response to exertion, symptom exacerbation, post-exertional exhaustion, prolonged recovery period (usually 24 hours or more), and low threshold of physical and mental fatigability.
- At least one symptom from three of four neurological categories: neurocognitive impairment, pain, sleep disturbance, and neurosensory/perceptual/motor disturbances.
- At least one symptom from three of five immune/gastrointestinal/genitourinary categories: flu-like symptoms, susceptibility to viral infections with prolonged recovery, GI tract issues, genitourinary issues, sensitivities to food/medications/odors/chemicals.
- At least one symptom from the energy production/ion transport category (cardiovascular, respiratory, loss of thermostatic stability, intolerance of temperature extremes).
Importantly, ICC does not require a six-month waiting period. The authors argued that forcing a sick patient to wait half a year before being evaluated is cruel and clinically counterproductive — early recognition may improve outcomes.
ICC is the most specific of all the major criteria sets. Patients who meet ICC almost certainly have the illness. The downside is that it is long, symptom-heavy, and almost never taught in U.S. medical schools. A family-medicine doctor with a 15-minute appointment slot will not apply ICC. A specialist at a referral ME/CFS clinic might.
IOM/NAM 2015 — SEID and the Push Into Primary Care
In 2015, the U.S. Institute of Medicine (now the National Academy of Medicine) published a landmark report, Beyond Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Redefining an Illness. The committee reviewed more than 9,000 scientific articles and interviewed patients, clinicians, and researchers. Their goal was blunt: create a definition simple enough that primary care physicians would actually use it.
They proposed a new name, Systemic Exertion Intolerance Disease (SEID), and a dramatically streamlined criteria set. The name never caught on — patients and advocacy groups largely rejected it, and most clinicians still say "ME/CFS" — but the criteria themselves have become the de facto U.S. clinical standard and are endorsed by the CDC.
SEID requires all three of the following:
- A substantial reduction or impairment in the ability to engage in pre-illness levels of occupational, educational, social, or personal activities, persisting more than six months, accompanied by fatigue (often profound) that is of new or definite onset, not the result of ongoing excessive exertion, and not substantially alleviated by rest.
- Post-exertional malaise.
- Unrefreshing sleep.
Plus at least one of:
- Cognitive impairment (brain fog), OR
- Orthostatic intolerance (symptoms worsening when upright).
That is the entire definition. Three core symptoms plus one of two. A busy primary care physician can apply it in a single visit.
SEID kept what CCC and ICC made non-negotiable — PEM is required — while stripping away the long category lists that made the earlier definitions too complicated for general practice. Validation studies (Jason et al., 2015) found that SEID captures a larger share of ME patients than Fukuda while remaining far more specific, because PEM is now mandatory.
Side-by-Side: Sensitivity, Specificity, and What Each One Misses
No criteria set is perfect, and each one makes trade-offs between catching every real case (sensitivity) and excluding people who have something else (specificity).
- Holmes 1988 — historically important, now obsolete. Did not require PEM. Low sensitivity, moderate specificity. Do not let a physician use this.
- Fukuda 1994 — high sensitivity, poor specificity. PEM optional. Sweeps in patients with depression, burnout, and deconditioning. Still common in research papers, still taught to older U.S. physicians. Produces a heterogeneous patient group, which is why research trials with Fukuda-selected cohorts often contradict each other.
- CCC 2003 — good sensitivity, good specificity. PEM required. Adds autonomic and immune features. Identifies a more biologically consistent patient group than Fukuda. The workhorse criteria set for ME/CFS specialists.
- ICC 2011 — lower sensitivity, highest specificity. Demands the most symptoms. Patients who meet ICC are unmistakably ill; patients who almost meet it may still have ME/CFS. Rarely used in primary care.
- SEID 2015 — high sensitivity, high specificity, easy to apply. PEM and unrefreshing sleep both required. Does not explicitly capture immune or neuroendocrine features, so it can miss the full clinical picture — but it catches the core illness reliably and is the best practical choice for primary care.
The most common real-world mistake: a patient has classic ME/CFS, the PCP applies Fukuda (or no criteria at all), notes "fatigue and poor sleep," and writes "chronic fatigue" on the chart. That vague label unlocks no treatment, no specialist referral, and no disability support. The same patient evaluated under CCC or SEID with careful questioning about PEM would get a real diagnosis and real help.
How to Use a Self-Score Sheet Before Your Appointment
A short written summary handed to your doctor at the start of a visit is the single most effective way to get an accurate diagnosis. Most physicians have seen fewer than a handful of ME/CFS patients in their career and cannot remember the criteria off the top of their head. Make it easy for them.
Write a one-page sheet that covers:
- Onset. Month and year symptoms began. Any trigger you can identify (a viral illness, surgery, pregnancy, major stressor, vaccination, concussion).
- Baseline vs. now. One sentence describing your pre-illness activity level (e.g., "ran 20 miles a week, worked full-time as a nurse"). One sentence for current level ("housebound 4 days a week, cannot work").
- Post-exertional malaise. Describe a specific example. "After attending my nephew's birthday party for two hours, I was bedridden for four days with flu-like body aches, worsened brain fog, and had to cancel appointments for a week." Note the delay (did the crash start hours later or the next day?) and the duration. This single paragraph is the most important thing you will give your doctor.
- Unrefreshing sleep. "I sleep 9–10 hours and wake feeling as tired as when I went to bed, every day."
- Cognitive impairment. Give concrete examples: losing words mid-sentence, getting lost driving to familiar places, unable to read a page of a novel.
- Orthostatic intolerance. "Within 5 minutes of standing I become lightheaded, my heart races, vision darkens at the edges." If you have measured heart rate on standing, include the numbers.
- Duration. "Symptoms have continued without resolution for [X] months."
- What you have already ruled out. List any labs and imaging that came back normal (TSH, CBC, CMP, iron, B12, vitamin D, cortisol, sleep study, etc.)
At the end, write a single line: "Please evaluate me against the 2015 IOM/NAM criteria for ME/CFS (SEID) and/or the Canadian Consensus Criteria." That one line tells the doctor which ruler to use.
Talking to a Skeptical Primary Care Physician
If your physician pushes back — "this is just depression," "you need to exercise more," "everyone is tired" — you are not stuck. Try these moves, in order, without getting into an argument.
- Cite the source, not the symptom. "The 2015 Institute of Medicine report, commissioned by the NIH and HHS, concluded ME/CFS is a serious, chronic, complex, multisystem disease." The IOM is a mainstream, conservative institution. Citing it is harder to dismiss than citing a patient advocacy group.
- Name the CDC. The CDC now recommends the IOM/SEID criteria and explicitly states that graded exercise therapy is not recommended because it can worsen PEM. If your doctor suggests pushing through exercise, show them the CDC ME/CFS clinician guidance page.
- Distinguish PEM from fatigue. "This is not being tired. Exertion triggers a measurable physiological crash that lasts days. The objective test for this is a 2-day cardiopulmonary exercise test, which shows a drop in anaerobic threshold on day two that is not seen in healthy controls or in deconditioned patients."
- Ask for a referral, not a diagnosis. If the PCP is unwilling to diagnose, ask for a referral to a rheumatologist, neurologist, or ME/CFS-literate clinic. Getting out of the room with a referral in hand is a win.
- Switch clinicians if you can. Not every PCP is a good fit for a complex multisystem illness. If you are being dismissed repeatedly, you are allowed to find a new doctor. Patient forums (Health Rising, Phoenix Rising, #MEAction) maintain crowdsourced lists of ME/CFS-literate physicians by region.
ICD-10 Coding: G93.3 vs R53.82 and Why It Matters
The diagnosis code on your chart determines how the medical system treats you — literally and administratively. There are two codes you may see, and they are not equivalent.
- G93.3 — Postviral fatigue syndrome; Benign myalgic encephalomyelitis. This is a neurological code, in the "Diseases of the Nervous System" chapter. It aligns with the WHO's classification of ME as a neurological disease since 1969. A G93.3 code communicates that you have a recognized organic illness.
- R53.82 — Chronic fatigue, unspecified. This is a symptom code, in the "Symptoms, Signs, and Abnormal Clinical Findings" chapter. It sits next to codes like "malaise" and "weakness." It communicates that the doctor observed fatigue but did not diagnose a disease.
Why the distinction matters in practice:
- Disability claims. Social Security Disability (SSDI) and private long-term disability insurers routinely deny R53.82 claims on the grounds that "chronic fatigue" is a symptom, not a disease. G93.3 gets treated as a recognized medical condition with a neurological basis. SSA's own guidance (SSR 14-1p) recognizes ME/CFS as a medically determinable impairment.
- Insurance coverage. Some commercial insurers cover workup and specialist referrals more readily under G93.3 than R53.82. Home health, physical therapy, and durable medical equipment (shower chairs, wheelchairs) authorizations often turn on the code.
- Research and statistics. Epidemiological counts of ME/CFS prevalence depend on which codes are pulled. Undercoding with R53.82 makes the disease look rarer than it is, which starves it of research funding.
If your chart shows R53.82, you can politely ask your physician to update the diagnosis to G93.3 if you meet CCC, ICC, or SEID criteria. Bring your self-score sheet. This is a small administrative change that can meaningfully improve what the rest of the system will do for you.
Which Criteria Should You Ask to Be Evaluated Under?
For most patients in U.S. primary care today, the practical answer is:
- Ask first for IOM/SEID 2015. It is short, endorsed by the CDC, and your PCP can actually apply it in one visit.
- If SEID is met and you want a tighter clinical picture, ask a specialist for CCC 2003. The broader CCC symptom list often surfaces autonomic and immune features worth treating separately (see orthostatic intolerance in ME/CFS).
- ICC 2011 is valuable when you need maximum diagnostic rigor — for example, for disability appeals, private insurance disputes, or enrollment in research studies.
- Do not settle for Fukuda alone. If a physician tells you "you meet the Fukuda criteria for CFS," ask them to also apply SEID or CCC so PEM is explicitly documented in the chart.
- Do not accept a chart entry of "chronic fatigue, R53.82" if you actually meet a disease-level definition. Push politely for G93.3.
Your diagnosis is a paperwork decision with medical consequences. The criteria and the ICD-10 code your doctor writes down will shape every conversation with every clinician, insurer, and disability examiner who comes after. A little preparation before the appointment pays back for years.
Key Research Papers
- Institute of Medicine. Beyond Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Redefining an Illness. National Academies Press, 2015. (IOM/SEID criteria)
- Carruthers BM, et al. Myalgic encephalomyelitis: International Consensus Criteria. J Intern Med. 2011;270(4):327–338.
- Carruthers BM, et al. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Clinical Working Case Definition, Diagnostic and Treatment Protocols (Canadian Consensus Criteria). J Chronic Fatigue Syndr. 2003;11(1):7–115.
- Fukuda K, et al. The chronic fatigue syndrome: a comprehensive approach to its definition and study. Ann Intern Med. 1994;121(12):953–959.
Live PubMed Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on ME/CFS case definitions, diagnostic accuracy, and coding:
- IOM/SEID criteria for ME/CFS
- Canadian Consensus Criteria for ME
- International Consensus Criteria for ME
- Fukuda criteria — comparisons and critiques
- Post-exertional malaise in diagnostic criteria
- Sensitivity and specificity of ME/CFS case definitions
- ICD-10 coding (G93.3) in ME/CFS
- Jason and colleagues — criteria comparison studies
Connections
- ME/CFS Overview
- Orthostatic Intolerance in ME/CFS
- 2-Day CPET and Objective Testing
- Post-Viral Triggers: EBV and Others
- Post-Exertional Malaise
- Pacing and the Energy Envelope
- Severe and Very Severe ME
- LDN, Abilify and Experimental Therapies
- Mitochondrial Dysfunction and Energy Metabolism
- POTS
- MCAS
- Fibromyalgia
- Fibromyalgia: ACR 2016 Diagnostic Criteria
- Chronic Pain
- Fatigue
- Brain Fog
- Depression