Creatinine: Reference Ranges, Interpretation, and Pitfalls
Serum creatinine is the single most widely used kidney marker on the planet. It is cheap, automated, available at every clinical laboratory, and reasonably reproducible. It is also, on its own, a flawed proxy for kidney function — sensitive to muscle mass, age, sex, ethnicity, dietary creatine, and several common medications that look like kidney injury but aren't. The job of this page is to teach you how to read creatinine in context: what's actually being measured, what the number means, and the half-dozen ways it can mislead.
Interactive Visualization Kidney Nephron — watch blood become urine Follow blood into the glomerulus and see filtration and reabsorption turn 180 litres of filtrate into urine — then toggle dehydration or diabetes. Launch →Table of Contents
- What Creatinine Is
- Reference Ranges
- The "Creatinine Blind Range"
- Causes of Elevated Creatinine
- Causes of Low Creatinine
- Non-Kidney Things That Move Creatinine
- Acute Kidney Injury vs CKD
- Preparation and Specimen
- Creatinine vs Creatine Supplement
- Research Papers and References
- Connections
- Featured Videos
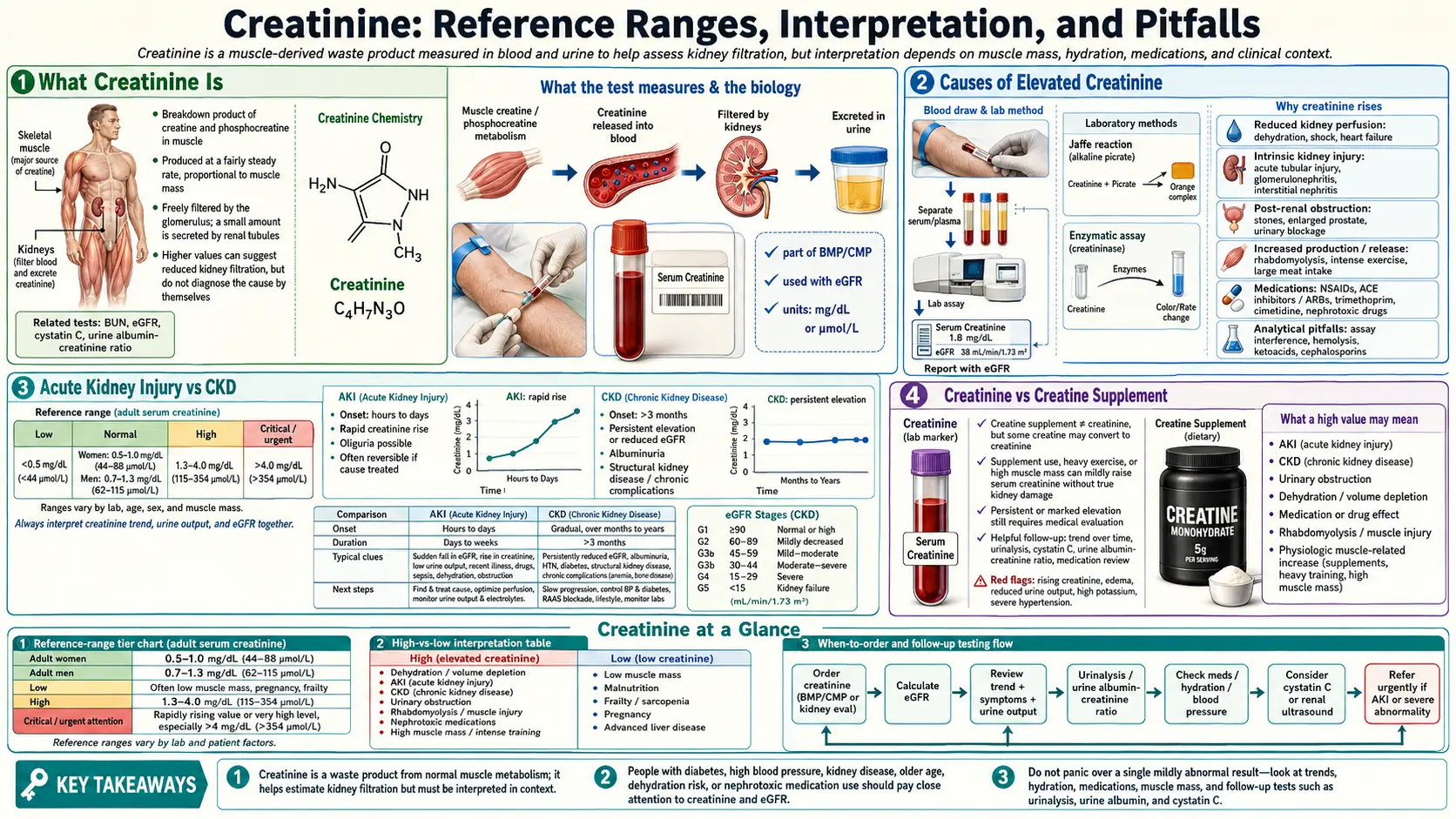
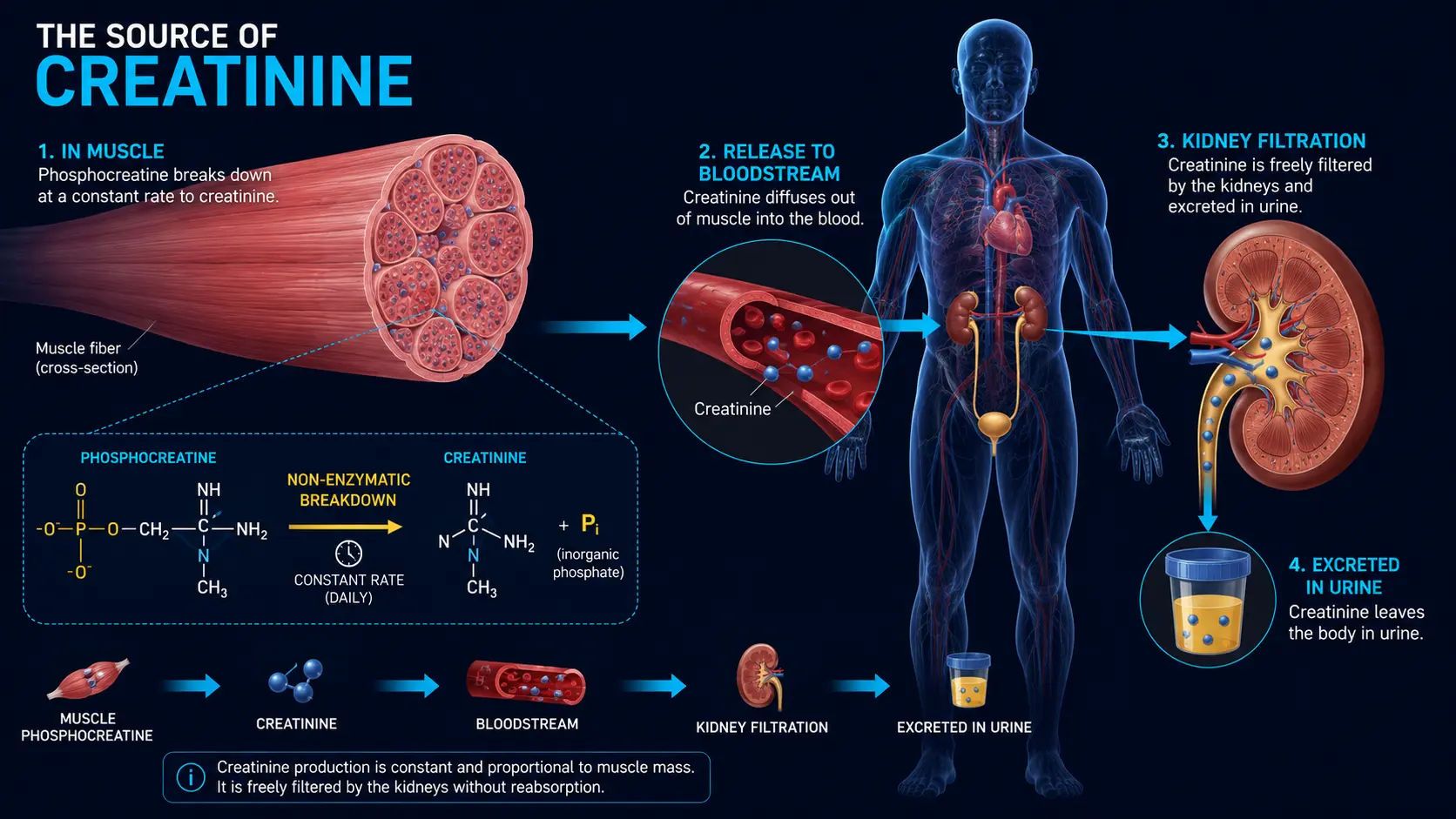
What Creatinine Is
Creatine is stored in muscle tissue as phosphocreatine, the high-energy phosphate buffer that lets a sprinter accelerate before glycolysis ramps up. About 1–2% of the body's creatine pool degrades non-enzymatically every day to creatinine, a small (113 Da) waste molecule. Creatinine is released into plasma at a roughly constant rate that is proportional to total muscle mass.
The kidneys handle creatinine in a near-ideal way for a filtration marker: it is freely filtered at the glomerulus, almost not reabsorbed, and only about 10–20% is added by tubular secretion. Because production is steady (when muscle mass and diet are stable) and filtration is the dominant mechanism of clearance, serum creatinine is a useful index of how well the glomerulus is doing its job.
The corollary — and the source of most clinical confusion — is that anything affecting muscle mass, dietary protein, or tubular secretion will move creatinine independently of actual kidney function.
Reference Ranges
Serum Creatinine — Adult Male (mg/dL)
Serum Creatinine — Adult Female (mg/dL)
Reference ranges differ between labs and methods (Jaffe vs. enzymatic), and the difference between sexes reflects average lean body mass — not a difference in kidney physiology. To convert mg/dL to µmol/L, multiply by 88.4 (1.0 mg/dL ≈ 88 µmol/L).
Children, pregnant patients, and bodybuilders all have their own normal patterns. A creatinine of 1.4 in a heavily muscled male athlete may be entirely benign; the same value in a frail 80-year-old woman represents significant kidney impairment.
The "Creatinine Blind Range"
Because production is constant and filtration has enormous reserve, serum creatinine does not rise linearly as kidneys decline. A patient can lose roughly 50% of their nephrons before serum creatinine creeps above the reference range. Once nephron loss exceeds 50%, creatinine begins to rise sharply — the classic hyperbolic relationship between serum creatinine and GFR.
This is the "creatinine blind range": early CKD that creatinine alone cannot detect. Two strategies bridge the gap:
- eGFR formulas (CKD-EPI 2021) translate serum creatinine plus age and sex into an estimated filtration rate, providing more clinically meaningful numbers in the early-CKD range
- Cystatin C — an alternative filtration marker that is more sensitive in the early ranges of nephron loss; a normal creatinine with elevated cystatin C is an early warning
Causes of Elevated Creatinine
Reduced filtration (the kidneys are not clearing it)
- Acute kidney injury — any cause; defined as creatinine rise of ≥ 0.3 mg/dL in 48 hours or 50% in 7 days
- Chronic kidney disease — diabetic, hypertensive, glomerulonephritis, polycystic, obstructive, drug-induced
- Dehydration — transient, reverses with rehydration
- Heart failure, shock, sepsis — reduced renal perfusion
- Bilateral renal artery stenosis
- Postrenal obstruction — bladder outlet obstruction, ureteral stones, retroperitoneal disease
Increased production (more muscle than the formulas assume)
- Bodybuilders, athletes with very high lean mass
- Recent strenuous exercise (transient)
- Rhabdomyolysis — massive muscle injury releases creatinine and creatine kinase together; usually with brown urine, elevated CK, and elevated potassium
Drug-induced creatinine elevations without true kidney injury
These are important because they look exactly like kidney injury on the printout but require no intervention:
- Cimetidine, trimethoprim (in Bactrim/Septra) — competitively inhibit tubular secretion of creatinine, raising serum levels by 0.2–0.4 mg/dL without changing GFR
- Cobicistat, dolutegravir (HIV antiretrovirals) — same mechanism
- Fenofibrate — mechanism less clear but well-documented; can raise creatinine 0.1–0.3 mg/dL
If creatinine rises modestly and stably right after starting one of these drugs, with no other clinical change, the likely diagnosis is the drug effect — not AKI.
Causes of Low Creatinine
- Reduced muscle mass — frailty, sarcopenia, advanced age, prolonged hospitalization, cachexia, neuromuscular disease, amputation
- Pregnancy — physiologic; increased plasma volume and GFR
- Vegetarian or vegan diet — lower dietary creatine load
- Severe liver disease — impaired creatine synthesis
- Glucocorticoid use, chronic illness, malnutrition — muscle wasting
Critically, "normal" creatinine in a frail patient with low muscle mass can hide significant kidney impairment. This is one of the strongest indications to use cystatin C-based eGFR.
Non-Kidney Things That Move Creatinine
Patients are often alarmed by lab printouts. These are the most common benign reasons creatinine moves:
- Heavy workout in the previous 24 hours — transient rise of 0.1–0.3 mg/dL
- Large meal of red meat — transient rise of 0.1–0.3 mg/dL within hours
- Creatine supplementation — raises baseline by 0.1–0.4 mg/dL via increased muscle creatine pool
- Starting cimetidine, trimethoprim, fenofibrate, cobicistat, dolutegravir — described above
- Recent contrast study — iodinated contrast can cause a real, usually self-limited AKI; recheck at 48–72 hours
- Lab method change — switching between Jaffe and enzymatic assays can shift values by 5–10%
Acute Kidney Injury vs CKD
The same creatinine value can mean very different things depending on the trajectory:
- Acute kidney injury (AKI) — KDIGO criteria: creatinine rise ≥ 0.3 mg/dL in 48 hours, OR creatinine rise ≥ 1.5× baseline within 7 days, OR urine output < 0.5 mL/kg/hr for 6 hours. AKI is staged 1–3 by the magnitude of rise. Most AKI is reversible if the trigger is identified and corrected quickly (volume, drugs, obstruction, sepsis).
- Chronic kidney disease (CKD) — reduced eGFR or albuminuria persisting for at least three months. The slope matters more than any single value: a stable creatinine of 1.6 in a known CKD patient is reassuring; a creatinine that has climbed from 0.9 to 1.6 over a year is an alarm bell.
The single most useful diagnostic question when an elevated creatinine appears is: "What was it last year, and the year before?" A baseline value transforms a confusing lab result into a clear trajectory.
Preparation and Specimen
- Fasting: not strictly required, though typically drawn fasting as part of a metabolic panel
- Avoid heavy exercise, very-high-protein meal, and cimetidine/trimethoprim immediately before the draw if a tight comparison is needed
- Tube: serum separator (gold-top SST) or lithium heparin (green-top)
- Stability: stable at room temperature for 24 hours, refrigerated for 7 days, frozen indefinitely
- Methods: Jaffe (older, less specific, affected by bilirubin and ketones) and enzymatic (newer, more specific). Most modern labs use enzymatic.
Creatinine vs Creatine Supplement
A common patient question: does creatine supplementation harm the kidneys? The short answer is no — creatine raises serum creatinine slightly (0.1–0.4 mg/dL) by expanding the muscle creatine pool, but it does not damage healthy kidneys. Multiple randomized trials and a 2024 systematic review found no adverse renal effects of standard creatine supplementation in healthy adults at doses up to 5 g/day for years. The relevant practical point is to tell your physician you are supplementing creatine before a routine lab draw, and to expect a slightly elevated baseline creatinine that is not a red flag.
Patients with pre-existing CKD should discuss creatine with a nephrologist before starting, both because the small filtration burden is more meaningful in compromised kidneys and because the elevated creatinine can confuse staging.
For more on the supplement, see Creatine.
Research Papers and References
- Serum creatinine as a kidney marker — PubMed search
- KDIGO AKI definition — PubMed search
- Creatine supplementation and kidney function — PubMed search
- Drugs blocking creatinine secretion — PubMed search
- Rhabdomyolysis and kidney injury — PubMed search
- Jaffe vs enzymatic creatinine assay — PubMed search
- Sarcopenia and creatinine in elderly CKD — PubMed search
External Authoritative Resources
- MedlinePlus — Creatinine Test
- National Kidney Foundation — Blood Tests
- KDIGO — Acute Kidney Injury Guideline
Connections
- Kidney Nephron — interactive animation
- eGFR
- Cystatin C
- BUN
- Kidney Function Tests
- Comprehensive Metabolic Panel
- Urinalysis
- Creatine
- Kidney Disease
- Acute Kidney Injury
- Glomerulonephritis
- Nephrotic Syndrome
- Heart Failure
- Sepsis
- Potassium
- Preeclampsia
- Hyperparathyroidism
- Cadmium
- Diabetes Complications