Edema and Swelling
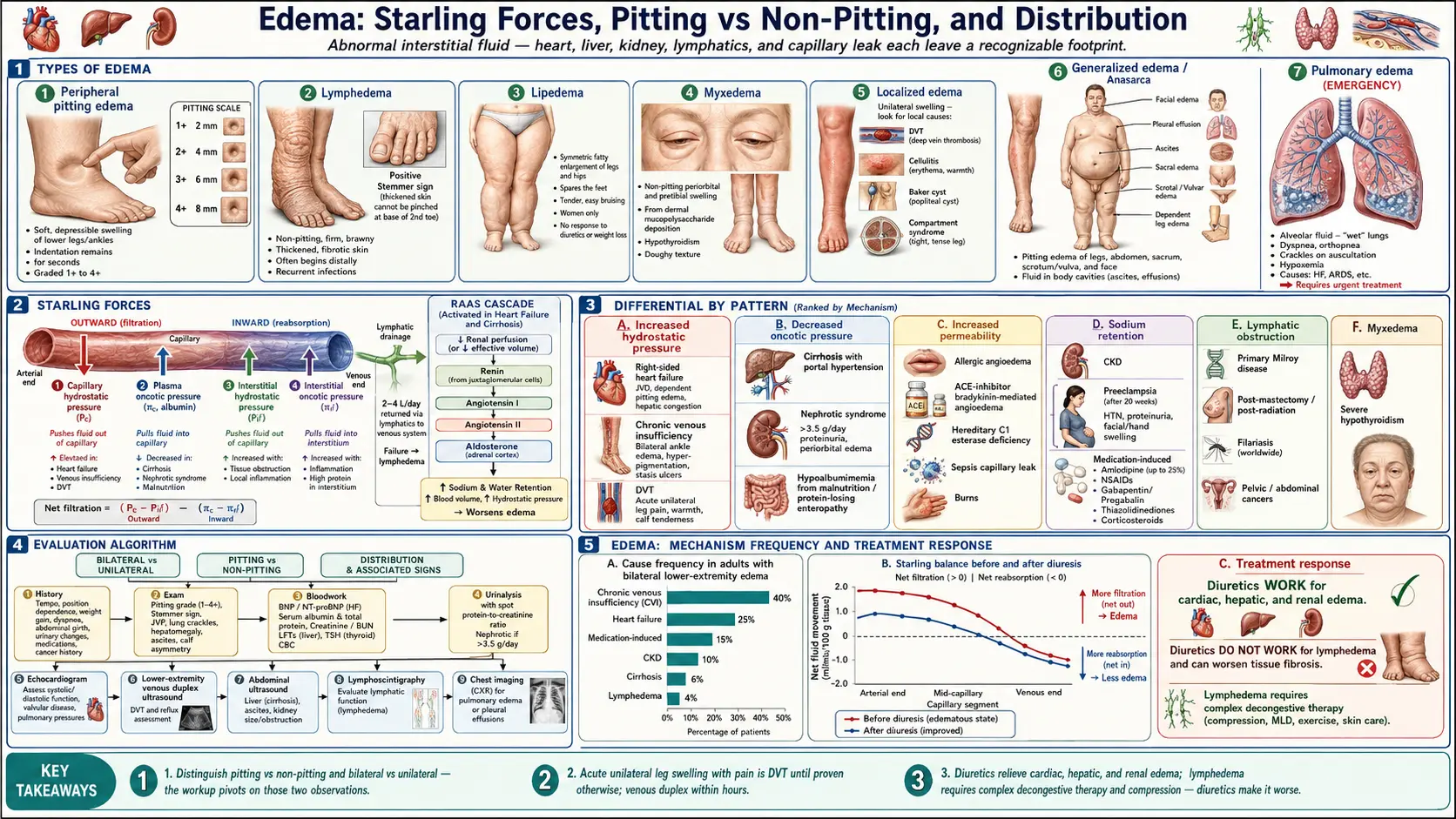

Table of Contents
- Overview
- Types of Edema
- Common Causes
- Mechanisms
- Evaluation
- Management
- When to Seek Medical Care
- Connections
- References & Research
- Featured Videos
Overview
Edema is the abnormal accumulation of fluid in the interstitial spaces of the body, producing visible swelling and, in many forms, an indentation that persists when the skin is pressed (pitting edema). When edema is generalized and severe enough to involve the entire body — including the trunk, face, and serous cavities — it is called anasarca. Edema may be pitting (the typical fluid-overload pattern of heart, kidney, and liver disease) or non-pitting (lymphatic obstruction, myxedema, lipedema). Distribution matters: bilateral lower-extremity edema points toward systemic causes, unilateral leg swelling raises concern for deep vein thrombosis or local lymphatic obstruction, and facial or periorbital swelling suggests nephrotic syndrome, hypothyroidism, or angioedema. Edema is not a disease in itself but a sign that capillary fluid balance has been disrupted — finding the underlying cause is the entire point of the workup.
Types of Edema
- Peripheral pitting edema — the most common form. Soft, indents with thumb pressure, and is graded 1+ to 4+ by depth and recovery time. Driven by elevated capillary hydrostatic pressure (cardiac), reduced plasma oncotic pressure (renal, hepatic, hypoalbuminemic), or increased capillary permeability.
- Lymphedema — non-pitting, firm, and brawny. Begins distal (toes, dorsum of foot) and progresses proximally. The Stemmer sign — inability to pinch a fold of skin at the base of the second toe — is pathognomonic. Skin becomes thickened and fibrotic over time.
- Lipedema — symmetric fatty enlargement of the legs and hips that spares the feet, almost exclusively in women. Tender to palpation, does not pit, and does not respond to weight loss or diuretics.
- Myxedema — non-pitting swelling from deposition of mucopolysaccharides in the dermis, classically in severe hypothyroidism. Periorbital and pretibial distribution; doughy texture.
- Localized edema — unilateral and confined to one region. Causes include deep vein thrombosis, cellulitis, ruptured Baker cyst, compartment syndrome, and post-surgical lymphatic disruption.
- Generalized edema (anasarca) — widespread pitting edema involving the legs, abdomen, sacrum, scrotum or vulva, and face, often with ascites and pleural effusion. Seen in advanced heart failure, end-stage liver disease, severe nephrotic syndrome, and protein-losing enteropathy.
- Pulmonary edema — fluid in the alveoli and interstitium of the lung, producing dyspnea, orthopnea, and crackles. A medical emergency in its acute form, usually from left-sided heart failure or acute respiratory distress syndrome.
Common Causes
- Right-sided heart failure — the right ventricle cannot keep up with venous return, raising central venous and capillary hydrostatic pressure. Produces dependent pitting edema (ankles in ambulatory patients, sacrum in bedridden), often with jugular venous distension and hepatic congestion.
- Cirrhosis with portal hypertension — reduced hepatic albumin synthesis and splanchnic vasodilation activate the renin-angiotensin-aldosterone system, causing sodium and water retention. See Liver Disease. Manifests as ascites and lower-extremity edema.
- Nephrotic syndrome — massive urinary protein loss (>3.5 g/day) drops serum albumin, lowers oncotic pressure, and causes generalized pitting edema with prominent periorbital and lower-extremity involvement.
- Chronic kidney disease — impaired sodium and water excretion produces volume overload. Edema worsens as glomerular filtration rate declines.
- Hypoalbuminemia — from severe malnutrition (kwashiorkor), protein-losing enteropathy, severe burns, or chronic illness. Low oncotic pressure allows fluid to leak into the interstitium.
- Chronic venous insufficiency — incompetent venous valves in the legs raise capillary hydrostatic pressure during standing. Produces bilateral ankle edema, hyperpigmentation, and venous stasis ulcers.
- Lymphedema — primary (congenital, Milroy disease) or secondary, most commonly post-mastectomy, post-radiation, or from filariasis worldwide. Pelvic and abdominal cancers can obstruct lymphatic drainage.
- Deep vein thrombosis (DVT) — acute unilateral leg swelling with pain, warmth, and calf tenderness. A diagnostic emergency because of pulmonary embolism risk. See Pulmonary Embolism.
- Medications — calcium-channel blockers (especially amlodipine) cause precapillary arteriolar dilation and dependent edema in up to 25 percent of users; NSAIDs reduce renal sodium excretion; gabapentin and pregabalin commonly cause peripheral edema; thiazolidinediones (pioglitazone, rosiglitazone) cause sodium retention and worsen heart failure; corticosteroids cause mineralocorticoid-driven retention.
- Preeclampsia — pregnancy-associated hypertension with proteinuria; sudden facial and hand swelling after 20 weeks gestation, often with headache or visual changes, is a medical emergency.
- Hypothyroidism — severe disease produces myxedema and periorbital puffiness. See Thyroid Disorders.
- Allergic angioedema — rapid-onset swelling of the lips, tongue, and face from histamine (allergic) or bradykinin (ACE-inhibitor-induced or hereditary). Airway compromise is the lethal complication.
Mechanisms
Edema is best understood through the Starling forces that govern fluid movement across the capillary wall — any imbalance among them allows interstitial fluid to accumulate faster than the lymphatics can clear it:
- Increased capillary hydrostatic pressure — the dominant mechanism in heart failure, venous insufficiency, and DVT. Elevated pressure inside the capillary pushes fluid out into the interstitium.
- Decreased plasma oncotic pressure — albumin is the chief plasma protein keeping fluid inside vessels. Hypoalbuminemia from cirrhosis, nephrotic syndrome, or malnutrition allows fluid to leak out.
- Increased capillary permeability — inflammation, sepsis, burns, and angioedema enlarge the gaps between endothelial cells, allowing protein-rich fluid to escape.
- Impaired lymphatic drainage — the lymphatic system normally clears 2–4 liters of interstitial fluid daily. Obstruction or destruction (surgery, radiation, filariasis, malignant invasion) produces lymphedema.
- RAAS activation in heart failure — reduced cardiac output triggers renin release, generating angiotensin II and aldosterone. The kidney retains sodium and water, expanding plasma volume and worsening congestion.
- Hepatic and renal sodium handling — in cirrhosis, splanchnic vasodilation underfills the arterial circulation, activating RAAS and avidly retaining sodium. In nephrotic syndrome, both decreased oncotic pressure and primary renal sodium retention contribute.
Evaluation
Evaluation is anchored on three observations: bilateral or unilateral, pitting or non-pitting, and distribution. These narrow the differential before any labs are drawn.
- History — onset and tempo, position dependence, weight gain, dyspnea, abdominal girth, urinary changes, medications, prior cancer or surgery, travel to filariasis-endemic regions.
- Physical exam — pitting grade, distribution (dependent vs generalized vs facial), Stemmer sign, jugular venous pressure, lung crackles, hepatomegaly, ascites, calf asymmetry, skin changes (hyperpigmentation, ulcers, peau d'orange).
- Bloodwork — BNP or NT-proBNP for heart failure, serum albumin and total protein for hypoalbuminemia, creatinine and BUN for renal function, liver function tests for hepatic disease, TSH for hypothyroidism, complete blood count.
- Urinalysis with protein quantification — spot urine protein-to-creatinine ratio or 24-hour collection; nephrotic-range proteinuria is >3.5 g/day.
- Echocardiogram — assesses ventricular function, valvular disease, pulmonary pressures, and pericardial disease.
- Lower-extremity venous duplex ultrasound — the test of choice for suspected DVT; also evaluates chronic venous reflux.
- Abdominal ultrasound — evaluates liver, spleen, ascites, and renal parenchyma.
- Lymphoscintigraphy — the gold standard for diagnosing lymphedema and distinguishing it from lipedema or chronic venous edema.
- Chest imaging — chest X-ray or CT for suspected pulmonary edema, pleural effusion, or mediastinal lymphatic obstruction.
Management
Treating the underlying cause is everything. Diuretics relieve congestion but do not address why the fluid accumulated, and they can be harmful in lymphedema, where they reduce intravascular volume without improving lymphatic clearance.
- Treat the underlying disease — heart failure regimen (ACE inhibitor or ARNI, beta-blocker, mineralocorticoid antagonist), albumin replacement and large-volume paracentesis for cirrhosis, immunosuppression for nephrotic syndromes, dialysis for renal failure, anticoagulation for DVT, levothyroxine for hypothyroidism, antihistamines or icatibant for angioedema.
- Loop diuretics — furosemide, bumetanide, torsemide. The mainstay for fluid overload in heart failure, cirrhosis, and renal disease. IV dosing is required when gut absorption is impaired by intestinal edema.
- Thiazide diuretics — hydrochlorothiazide, chlorthalidone, metolazone. Often added to a loop diuretic for synergistic distal sodium blockade in resistant edema.
- Potassium-sparing and aldosterone antagonists — spironolactone is first-line for cirrhotic ascites and a guideline-directed therapy in heart failure with reduced ejection fraction; eplerenone is an alternative.
- Salt restriction — sodium intake under 2 g/day in heart failure and cirrhosis; the single most underused intervention.
- Compression stockings — graduated 20–30 or 30–40 mmHg knee-high stockings for chronic venous insufficiency and lymphedema; contraindicated in arterial insufficiency.
- Leg elevation — raising the legs above heart level for 30 minutes several times a day reduces dependent edema.
- Complex decongestive therapy — the standard of care for lymphedema. Includes manual lymphatic drainage, multilayer bandaging, exercise, and skin care. Diuretics do not work for lymphedema and can worsen tissue fibrosis.
- Paracentesis — large-volume removal of ascites for tense or symptomatic distension; albumin replacement (6–8 g per liter removed) prevents post-paracentesis circulatory dysfunction.
- Anticoagulation — DOACs (apixaban, rivaroxaban) or warfarin for DVT and pulmonary embolism, with duration determined by provoked vs unprovoked status and ongoing risk factors.
- Stop or substitute offending medications — switch amlodipine to a non-dihydropyridine calcium-channel blocker or another antihypertensive class; discontinue NSAIDs, gabapentin, or thiazolidinediones if implicated.
When to Seek Medical Care
- Acute unilateral leg swelling with pain, warmth, or calf tenderness — concern for DVT; requires immediate venous duplex ultrasound.
- Shortness of breath with leg swelling — possible heart failure, pulmonary edema, or pulmonary embolism.
- Facial, lip, or tongue swelling — angioedema or anaphylaxis; airway compromise is a true emergency.
- Sudden generalized swelling with foamy urine — nephrotic syndrome or rapidly progressive glomerulonephritis.
- Painful, warm, red, expanding swelling — cellulitis or necrotizing soft-tissue infection; needs urgent antibiotics or surgical evaluation.
- Pregnancy with sudden facial or hand swelling, headache, visual changes, or right-upper-quadrant pain — preeclampsia, possibly severe features or HELLP syndrome.
- Rapidly enlarging abdominal girth — new ascites from heart failure, cirrhosis, malignancy, or nephrotic syndrome.
- Anasarca with confusion, hypotension, or oliguria — hepatorenal syndrome, cardiorenal syndrome, or septic capillary leak; needs hospitalization.
Connections
- Heart Failure
- Pulmonary Embolism
- Liver Disease
- Kidney Disease
- Thyroid Disorders
- Hypertension
- Shortness of Breath
- Preeclampsia
- Cardiomyopathy
- Magnesium
- Anemia
- Pulmonary Hypertension
- Nephrotic Syndrome
- Cirrhosis
- Deep Vein Thrombosis
- Pleural Effusion
- Atrial Fibrillation
- Acute Kidney Injury
- Varicose Veins
References & Research
Historical Background
The understanding of edema has been shaped by a series of physiological insights spanning more than a century. In 1896, Ernest Starling published his hypothesis on capillary fluid exchange — that the balance between capillary hydrostatic pressure and plasma oncotic pressure governs the movement of water across the vascular wall — which remains the conceptual backbone of modern edema medicine. The mid-twentieth century delineation of nephrotic syndrome and the renin-angiotensin-aldosterone axis explained why heart, liver, and kidney disease all converge on sodium retention. The 1960s introduction of furosemide and the loop-diuretic class transformed the management of pulmonary edema and refractory congestion. Lymphedema therapy was revolutionized by Michael Földi and his colleagues in Germany during the 1970s and 1980s with the codification of complex decongestive therapy, which remains the cornerstone of lymphatic care. The 2018 international consensus guidelines from the International Society of Lymphology formalized staging and treatment standards still in use today.
Key Research Papers
- Mortimer PS, Rockson SG. New developments in clinical aspects of lymphatic disease. The Lancet. 2014;383(9912):1158-1166.
- Search PubMed
- Felker GM, Lee KL, Bull DA, et al. Diuretic strategies in patients with acute decompensated heart failure. New England Journal of Medicine. 2011;364(9):797-805.
- Cho S, Atwood JE. Peripheral edema. The American Journal of Medicine. 2002;113(7):580-586.
- Heidenreich PA, Bozkurt B, Aguilar D, et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure. Circulation. 2022;145(18):e895-e1032.
- Search PubMed
- Eknoyan G. A history of edema and its management. Kidney International Supplements. 1997;59:S118-S126.
- Rockson SG. Lymphedema. New England Journal of Medicine. 2018;378(20):1937-1944.
- Eberhardt RT, Raffetto JD. Chronic venous insufficiency. Circulation. 2014;130(4):333-346.
- Schrier RW. Decreased effective blood volume in edematous disorders: what does this mean? Journal of the American Society of Nephrology. 2007;18(7):2028-2031.
PubMed Topic Searches
- Peripheral edema evaluation and management
- Lymphedema and complex decongestive therapy
- Heart failure and diuretic therapy
- Nephrotic syndrome and edema pathophysiology
- Chronic venous insufficiency
- Cirrhosis and ascites management