Deep Vein Thrombosis
CRITICAL WARNING: Deep vein thrombosis (DVT) is a medical emergency. If you suspect you have a DVT — particularly if you experience sudden leg swelling, pain, warmth, or redness — seek immediate medical attention. Pulmonary embolism, a life-threatening complication of DVT, can occur without warning. The natural approaches discussed in this article are for prevention and adjunct support only and must never replace anticoagulant therapy or emergency medical care.
Interactive Visualization How Blood Clots — and how thinners stop it Build a platelet plug, weave a fibrin mesh, then watch aspirin, warfarin and a DOAC each break a different step — with a live INR. Launch → Interactive Visualization How Clots Dissolve — snip the mesh or blast it with tPA Watch plasmin snip the fibrin mesh strand by strand and D-dimer wash away — then add a tPA clot-buster to blast it, or tranexamic acid to hold it shut. Launch →
Table of Contents
- Table of Contents
- What Is Deep Vein Thrombosis?
- Virchow's Triad
- Risk Factors
- Signs and Symptoms
- Pulmonary Embolism
- Diagnosis
- Conventional Treatment
- Natural Prevention Support
- Compression Stockings
- Movement, Exercise, and Hydration
- Hydration and Travel Precautions
- Post-Thrombotic Syndrome
- Important Cautions
- Research Papers
- Connections
- Featured Videos
What Is Deep Vein Thrombosis?
Deep vein thrombosis (DVT) is a condition in which a blood clot (thrombus) forms in one or more of the deep veins of the body, most commonly in the legs (iliac, femoral, and popliteal veins). Unlike superficial vein clots, which are generally less dangerous, deep vein clots can break free, travel through the bloodstream, and lodge in the pulmonary arteries, causing a potentially fatal pulmonary embolism (PE).
DVT affects an estimated 1-2 per 1,000 people per year in the general population, with incidence rising sharply with age. Together, DVT and PE are collectively referred to as venous thromboembolism (VTE), which is the third most common cardiovascular disease after heart attack and stroke.
From a naturopathic perspective, understanding and addressing the underlying factors that promote clot formation — including inflammation, endothelial dysfunction, blood stagnation, and hypercoagulability — offers opportunities for meaningful prevention. However, once a DVT has formed, conventional anticoagulant therapy is essential and life-saving.
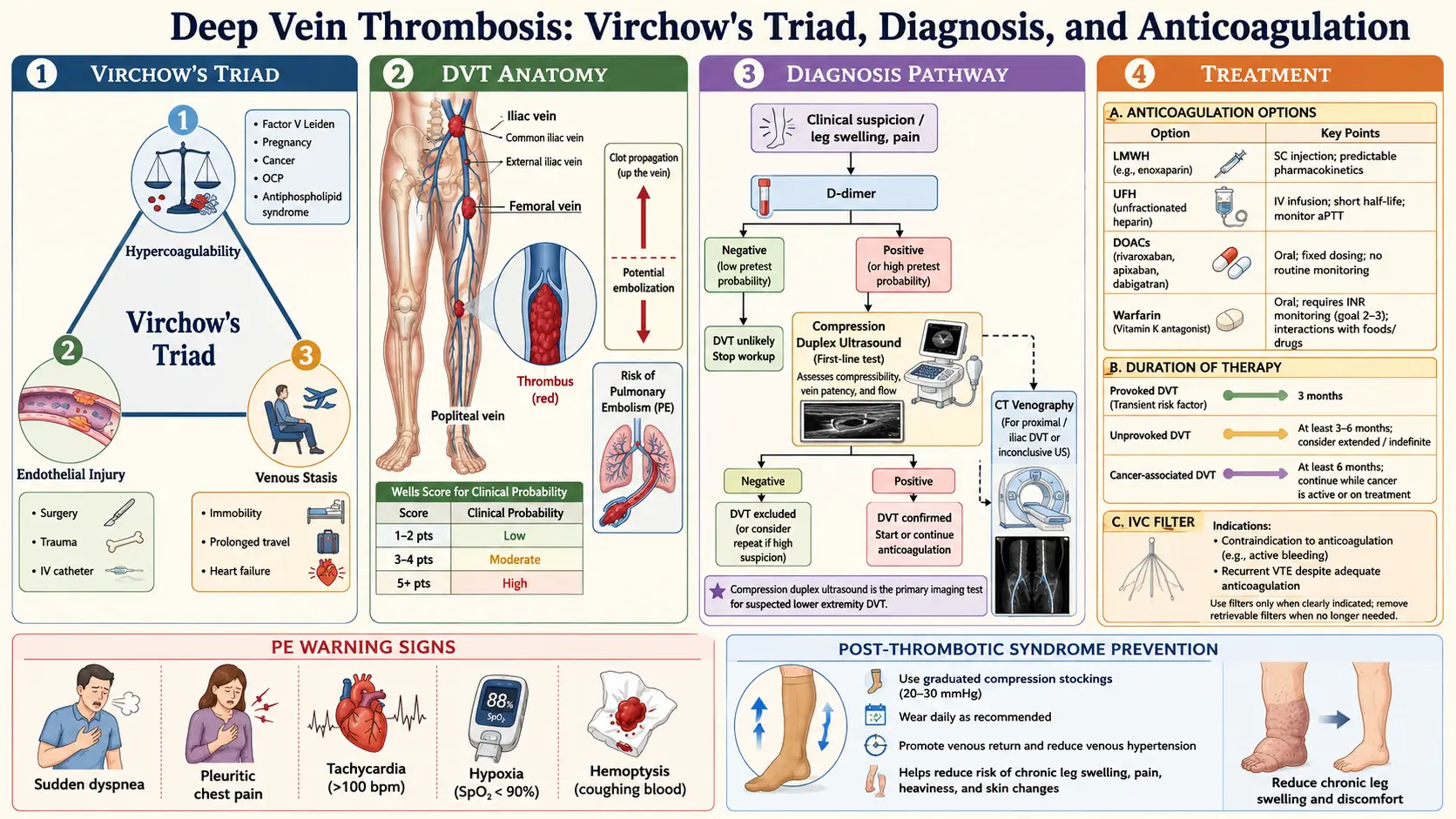
Virchow's Triad
The German physician Rudolf Virchow described three broad categories of factors that contribute to thrombus formation, known as Virchow's triad. DVT typically occurs when one or more of these factors are present:
1. Venous Stasis (Reduced Blood Flow)
When blood flows sluggishly through the veins, it is more likely to clot. Stasis can result from:
- Prolonged immobility — bed rest, long flights or car trips, sedentary lifestyle
- Paralysis or limb immobilization (casts, splints)
- Congestive heart failure (reduced cardiac output)
- Obesity (external compression of veins)
- Varicose veins with venous insufficiency
2. Endothelial Injury (Damage to Blood Vessel Walls)
Damage to the inner lining of veins exposes collagen and tissue factor, triggering the clotting cascade:
- Surgical trauma, especially orthopedic procedures (hip and knee replacement)
- Fractures and major trauma
- Central venous catheters
- Previous DVT causing scarring
- Chemotherapy and radiation
- Chronic inflammation
3. Hypercoagulability (Increased Tendency to Clot)
Certain conditions make the blood more prone to clotting:
- Inherited thrombophilias (Factor V Leiden, prothrombin gene mutation, protein C or S deficiency, antithrombin deficiency)
- Cancer and cancer treatment
- Pregnancy and postpartum period
- Oral contraceptives and hormone replacement therapy
- Antiphospholipid syndrome
- Elevated homocysteine levels
- Dehydration
Risk Factors
DVT risk factors span genetic, lifestyle, medical, and situational categories:
Medical and Surgical Risk Factors
- Recent surgery — Especially orthopedic (hip/knee replacement), abdominal, and pelvic surgery. Risk is highest in the first 2-4 weeks post-operatively.
- Cancer — Malignancy increases DVT risk 4-7 fold. Certain cancers (pancreatic, brain, lung, ovarian) carry particularly high risk. Chemotherapy further elevates risk.
- Previous DVT or PE — History of VTE is one of the strongest risk factors for recurrence (up to 30% within 10 years).
- Hospitalization and bed rest — Immobilization during illness is a leading cause of DVT.
- Central venous catheters — Upper extremity DVT is increasingly recognized in patients with central lines.
- Heart failure — Reduced cardiac output leads to venous stasis.
- Inflammatory bowel disease — Crohn's disease and ulcerative colitis increase VTE risk.
- Nephrotic syndrome — Loss of antithrombin and other anticoagulant proteins in urine.
Genetic Risk Factors
- Factor V Leiden mutation — The most common inherited thrombophilia, present in approximately 5% of Caucasians. Heterozygous carriers have a 3-8 fold increased risk; homozygous carriers have a 50-80 fold increased risk.
- Prothrombin G20210A mutation — Increases prothrombin levels and DVT risk 2-3 fold.
- Protein C deficiency
- Protein S deficiency
- Antithrombin deficiency — The most severe inherited thrombophilia
Lifestyle and Hormonal Risk Factors
- Obesity — BMI above 30 increases DVT risk 2-3 fold
- Smoking — Damages blood vessel walls and increases clotting tendency
- Pregnancy and postpartum — DVT risk increases 5-10 fold during pregnancy and is highest in the 6 weeks after delivery
- Oral contraceptives — Estrogen-containing pills increase DVT risk 3-4 fold, particularly in the first year of use
- Hormone replacement therapy — Increases DVT risk, especially oral formulations
- Sedentary lifestyle
- Long-distance travel — Flights or car journeys exceeding 4 hours ("economy class syndrome")
- Age — Risk doubles approximately every 10 years after age 40
- Dehydration — Increases blood viscosity and clotting tendency
Signs and Symptoms
DVT may present with classic symptoms or may be clinically silent. Up to 50% of DVTs produce no noticeable symptoms, which is why the condition can be so dangerous.
Classic Symptoms of Leg DVT
- Unilateral leg swelling — Swelling in one leg (particularly the calf) is the most characteristic sign. The affected leg may be noticeably larger than the other.
- Pain and tenderness — Often described as a cramping or aching sensation in the calf or thigh. Pain may worsen when walking or standing.
- Warmth — The skin over the affected area may feel warm to the touch compared to the other leg.
- Redness or discoloration — The skin may appear red, bluish, or purple.
- Distended superficial veins — Visible engorgement of superficial veins on the affected leg.
- Homan's sign — Pain in the calf upon dorsiflexion of the foot. However, this sign is unreliable and not recommended for clinical diagnosis.
When to Seek Emergency Care
Seek immediate emergency medical attention if you experience any of the following, which may indicate a pulmonary embolism:
- Sudden shortness of breath
- Sharp chest pain that worsens with deep breathing
- Rapid heart rate
- Coughing up blood
- Dizziness, lightheadedness, or fainting
Pulmonary Embolism
Pulmonary embolism (PE) is the most feared complication of DVT and occurs when a fragment of a deep vein clot breaks loose, travels through the venous system and right side of the heart, and lodges in a pulmonary artery, blocking blood flow to a portion of the lung.
Severity Spectrum
- Small PE — May cause mild breathlessness or may be asymptomatic (incidentally found on imaging)
- Moderate PE — Causes significant breathlessness, chest pain, and tachycardia. Right heart strain may be visible on echocardiography.
- Massive PE — Causes hemodynamic collapse (low blood pressure, shock), loss of consciousness, and can be rapidly fatal. Mortality without treatment exceeds 30%.
- Saddle PE — A large clot straddling the main pulmonary artery bifurcation, often immediately life-threatening
Statistics
- Approximately 25-50% of DVT patients develop PE
- PE causes an estimated 100,000-200,000 deaths annually in the United States
- PE is the leading preventable cause of hospital death
- Rapid diagnosis and treatment dramatically improve survival
Diagnosis
D-Dimer Test
The D-dimer is a blood test that measures a fibrin degradation product, released when the body breaks down blood clots:
- A negative D-dimer in a low-risk patient effectively rules out DVT (high sensitivity, high negative predictive value)
- An elevated D-dimer does not confirm DVT, as it can be raised by many conditions including infection, inflammation, surgery, pregnancy, cancer, and advanced age
- Most useful in outpatients with low to moderate clinical probability
Compression Ultrasound
Duplex ultrasonography is the primary imaging test for DVT diagnosis:
- Non-invasive, readily available, and highly accurate (sensitivity and specificity above 95% for proximal DVT)
- A vein that does not compress under the ultrasound probe is considered positive for thrombosis
- Color Doppler can assess blood flow and identify partial obstruction
- Less sensitive for calf (distal) DVT and iliac vein DVT
Clinical Probability Scores
The Wells score is widely used to assess the pre-test probability of DVT, combining clinical features such as active cancer, paralysis, recent immobilization, localized tenderness, leg swelling, pitting edema, and whether an alternative diagnosis is more likely.
Additional Imaging
- CT venography — For suspected iliac or pelvic DVT not well visualized by ultrasound
- MR venography — Alternative when CT is contraindicated
- CT pulmonary angiography (CTPA) — Gold standard for diagnosing pulmonary embolism
Thrombophilia Testing
Testing for inherited clotting disorders may be considered in:
- Patients with unprovoked DVT under age 50
- Recurrent VTE
- Strong family history of VTE
- DVT in unusual sites (cerebral, mesenteric, hepatic veins)
Conventional Treatment
Anticoagulant Therapy
Anticoagulation is the cornerstone of DVT treatment, preventing clot extension and PE while the body's natural fibrinolytic system gradually dissolves the existing clot:
- Unfractionated heparin (UFH) — Administered intravenously in the hospital setting. Used primarily for massive DVT/PE or when rapid reversal may be needed (such as peri-operatively).
- Low-molecular-weight heparin (LMWH) — Enoxaparin (Lovenox), dalteparin. Subcutaneous injections, often used as initial treatment. Predictable dosing allows outpatient management.
- Warfarin (Coumadin) — Traditional oral anticoagulant. Requires regular INR monitoring (target 2.0-3.0). Interacts with many foods (vitamin K-rich vegetables) and medications. Typically started alongside heparin and continued for 3-12 months or longer.
- Direct oral anticoagulants (DOACs) — Rivaroxaban (Xarelto), apixaban (Eliquis), edoxaban (Savaysa), dabigatran (Pradaxa). Increasingly preferred due to fixed dosing, no routine monitoring requirement, and fewer dietary interactions. Some can be used as monotherapy without initial heparin.
Duration of Anticoagulation
- Provoked DVT (clear trigger such as surgery or immobilization) — Typically 3 months
- Unprovoked DVT — Minimum 3-6 months, with consideration of extended or indefinite therapy based on bleeding risk and patient preference
- Recurrent DVT — Often indefinite anticoagulation
- Cancer-associated DVT — Anticoagulation continued as long as cancer is active
Thrombolysis and Thrombectomy
- Catheter-directed thrombolysis — Delivery of clot-dissolving medication directly into the thrombus via catheter. Reserved for extensive iliofemoral DVT in patients at low bleeding risk.
- Surgical thrombectomy — Rarely performed, reserved for life-threatening cases where anticoagulation and thrombolysis fail or are contraindicated.
- IVC filter — A device placed in the inferior vena cava to prevent clot migration to the lungs. Used when anticoagulation is contraindicated (active bleeding, recent surgery) or when PE occurs despite adequate anticoagulation.
Natural Prevention Support
Important: The following natural approaches are for DVT prevention and as adjunct support only. They must never replace anticoagulant therapy in patients with active DVT or those at high risk for VTE. Always discuss natural supplements with your physician, especially if you are taking anticoagulant medications, as interactions can increase bleeding risk.
Nattokinase
Nattokinase is a fibrinolytic enzyme derived from natto (fermented soybeans), a traditional Japanese food. Research suggests nattokinase has direct clot-dissolving activity and may also inhibit platelet aggregation and reduce blood viscosity. Studies have shown it can reduce fibrinogen levels and improve blood flow. Typical supplemental doses range from 2,000-4,000 fibrinolytic units (FU) daily. Nattokinase should be vitamin K2-free (labeled "NSK-SD") to avoid interference with anticoagulant therapy.
Omega-3 Fatty Acids
EPA and DHA from fish oil or algae sources have anti-inflammatory and mild anti-platelet properties. Omega-3s reduce blood viscosity, decrease fibrinogen levels, and improve endothelial function. Doses of 2-4 grams of combined EPA/DHA daily may provide cardiovascular and anti-thrombotic benefit. Higher doses should be monitored due to potential bleeding risk.
Vitamin E
Vitamin E (natural mixed tocopherols and tocotrienols) has mild anti-platelet activity and protects endothelial cells from oxidative damage. It may help reduce DVT risk by improving vascular health and reducing inflammation. Moderate doses (200-400 IU daily) are generally considered safe, though high doses may increase bleeding risk.
Garlic (Allium sativum)
Garlic contains allicin and ajoene, compounds with well-documented anti-platelet and fibrinolytic properties. Regular garlic consumption has been associated with improved blood flow and reduced clotting tendency. Aged garlic extract (600-1,200 mg daily) is commonly used for cardiovascular support with fewer gastrointestinal side effects than raw garlic.
Ginger (Zingiber officinale)
Ginger contains gingerols and shogaols that inhibit platelet aggregation and have anti-inflammatory effects. Ginger may reduce thromboxane production, a key mediator of platelet activation. It also supports healthy circulation and reduces inflammation that can contribute to endothelial damage.
Turmeric (Curcuma longa)
Curcumin, the active compound in turmeric, has anti-platelet, anti-inflammatory, and antioxidant properties. It inhibits platelet activation through multiple pathways and reduces the inflammatory processes that contribute to endothelial dysfunction and hypercoagulability. Bioavailability-enhanced formulations (with piperine or as liposomal preparations) are recommended for therapeutic benefit.
Bromelain
Bromelain, an enzyme complex from pineapple, has demonstrated fibrinolytic and anti-platelet activity. It may help reduce fibrin formation and improve blood flow. Typical doses range from 500-2,000 GDU daily, taken on an empty stomach for systemic (rather than digestive) effects.
Compression Stockings
Graduated compression stockings are a cornerstone of DVT prevention and management:
For DVT Prevention
- Recommended for hospitalized patients, post-surgical patients, and during long-distance travel
- Graduated compression (tightest at the ankle, decreasing up the leg) promotes venous return and reduces stasis
- Compression levels of 15-20 mmHg are appropriate for travel and mild prevention
- Medical-grade compression of 20-30 mmHg is recommended for higher-risk situations
For Post-DVT Management
- Compression stockings (30-40 mmHg) worn daily for at least 2 years after DVT may reduce the risk and severity of post-thrombotic syndrome
- Should be properly fitted by a trained professional for optimal benefit
- Replace stockings every 3-6 months as they lose elasticity
Proper Use
- Put on stockings first thing in the morning before the legs swell
- Ensure smooth fit without wrinkles or bunching, which can create tourniquet effects
- Remove overnight unless otherwise directed
- Contraindicated in patients with peripheral arterial disease — check ankle-brachial index if uncertain
Movement, Exercise, and Hydration
Regular movement and exercise are among the most effective natural strategies for DVT prevention:
Exercise Benefits
- Calf muscle pump — The calf muscles act as a "second heart," propelling venous blood back to the heart. Walking, calf raises, and ankle exercises activate this pump and reduce venous stasis.
- Regular aerobic exercise — Walking, swimming, cycling, and other aerobic activities improve venous return, reduce inflammation, maintain healthy body weight, and lower overall VTE risk.
- Post-surgical early mobilization — Getting out of bed and walking as soon as safely possible after surgery is one of the most important DVT prevention measures.
- Desk and workplace movement — For sedentary workers, take breaks every 1-2 hours to walk, stretch, and perform calf exercises.
Specific Exercises for Venous Health
- Ankle pumps — Point toes up and down repeatedly (10-20 repetitions every hour when seated)
- Ankle circles — Rotate feet in circles in both directions
- Calf raises — Rise up on toes and slowly lower (helps activate the calf muscle pump)
- Knee lifts — While seated, alternately lift knees toward chest
- Walking — Even brief walks (5-10 minutes) significantly improve venous flow
Hydration and Travel Precautions
Long-distance travel (flights, car rides, or train journeys exceeding 4 hours) is a well-recognized risk factor for DVT:
Hydration
- Drink water regularly — Aim for at least 8 ounces (250 mL) per hour during travel. Dehydration increases blood viscosity and clotting tendency.
- Avoid alcohol — Alcohol is dehydrating and a vasodilator that can promote venous pooling
- Limit caffeine — Excessive caffeine can contribute to dehydration
- Avoid sedatives — Sleeping pills reduce movement and worsen venous stasis during flights
In-Flight and Travel Strategies
- Request an aisle seat to allow easy movement
- Walk the aisle every 1-2 hours
- Perform seated exercises — Ankle pumps, calf raises, and knee lifts while seated
- Wear graduated compression stockings (15-20 mmHg) during flights exceeding 4 hours
- Avoid crossing legs for prolonged periods
- Wear loose, comfortable clothing that does not restrict circulation
- Store carry-on luggage overhead to maximize leg room
High-Risk Travelers
Individuals with additional DVT risk factors (previous VTE, cancer, recent surgery, thrombophilia, obesity) should consult their physician before long-distance travel. In some cases, a single prophylactic dose of LMWH may be recommended before a long flight.
Post-Thrombotic Syndrome
Post-thrombotic syndrome (PTS) is a chronic condition that develops in 20-50% of patients after a DVT, caused by damage to the venous valves and persistent venous obstruction:
Symptoms
- Chronic leg pain — Aching, heaviness, and cramping, often worse at the end of the day or with prolonged standing
- Persistent swelling — Edema that may fluctuate but never fully resolves
- Skin changes — Hyperpigmentation (brownish discoloration), eczema, thickening, and induration of the skin around the ankle
- Venous ulcers — In severe cases, painful ulcers develop near the ankle that are slow to heal (the most debilitating manifestation, affecting 5-10% of PTS patients)
- Varicose veins — New or worsening varicose veins from collateral venous circulation
Prevention and Management
- Adequate initial anticoagulation — Proper treatment of the initial DVT reduces PTS risk
- Graduated compression stockings — Worn daily for at least 2 years post-DVT
- Leg elevation — Elevating the legs above heart level for 20-30 minutes several times daily reduces edema and improves venous drainage
- Regular exercise — Walking and calf exercises improve the muscle pump and venous return
- Weight management — Obesity worsens venous insufficiency
- Skin care — Moisturize daily to prevent skin breakdown; treat eczema promptly
- Horse chestnut seed extract (Aesculus hippocastanum) — Contains aescin, which has anti-edema and venotonic properties. Studies support its use for chronic venous insufficiency symptoms.
- Butcher's broom (Ruscus aculeatus) — A venotonic herb that may reduce leg heaviness, swelling, and discomfort
Important Cautions
- DVT is a medical emergency. If you experience sudden leg swelling, pain, warmth, or redness, seek immediate medical evaluation. Do not attempt to self-treat with natural remedies.
- Pulmonary embolism can be fatal within minutes. Sudden shortness of breath, chest pain, rapid heart rate, or coughing up blood requires emergency medical care (call emergency services immediately).
- Natural supplements are for prevention and adjunct support ONLY. They must never replace anticoagulant therapy. Nattokinase, omega-3s, vitamin E, garlic, ginger, turmeric, and bromelain are not substitutes for heparin, warfarin, or DOACs.
- Bleeding risk with combined therapies. Many natural anti-thrombotic supplements can interact with anticoagulant medications and increase bleeding risk. Always inform your physician and pharmacist about all supplements you take. Key interactions include:
- Nattokinase + anticoagulants = significantly increased bleeding risk
- High-dose fish oil + anticoagulants = increased bleeding tendency
- Garlic, ginger, turmeric, and bromelain each have mild blood-thinning effects that can be additive
- Vitamin E in high doses (above 400 IU) may increase bleeding
- Stop natural blood-thinning supplements before surgery. Discontinue nattokinase, fish oil, vitamin E, garlic, ginger, turmeric, and bromelain at least 7-14 days before any surgical procedure, as directed by your surgeon.
- Do not use compression stockings if you have peripheral arterial disease (poor arterial circulation to the legs), as compression can further reduce blood flow. Consult your physician before using compression therapy.
- Thrombophilia testing should be performed at an appropriate time (not during acute DVT or while on anticoagulation), as results may be unreliable during these periods.
- Pregnancy-associated DVT requires specialized management. Warfarin and DOACs are contraindicated in pregnancy; LMWH is the standard of care.
- Consult a qualified healthcare professional — preferably a naturopathic doctor or integrative physician working in collaboration with a hematologist or vascular medicine specialist — before beginning any natural supplement protocol for DVT prevention.
Research Papers
The following PubMed topic searches return current peer-reviewed literature relevant to this condition. Each link opens a live PubMed query.
- Deep vein thrombosis epidemiology
- Deep vein thrombosis anticoagulation
- DVT D-dimer
- DVT compression ultrasound
- DOAC deep vein thrombosis
- Pulmonary embolism deep vein thrombosis
- DVT prophylaxis
- Post-thrombotic syndrome
- Catheter-directed thrombolysis DVT
- Wells score DVT
- DVT pregnancy
- Venous thromboembolism guidelines
Connections
- Hematology
- How Blood Clots Dissolve — Fibrinolysis & Clot-Busters — interactive animation
- How Blood Clots — interactive animation
- Pulmonary Embolism
- Thrombocytopenia
- Disseminated Intravascular Coagulation
- Polycythemia Vera
- Stroke
- Atrial Fibrillation
- Peripheral Artery Disease
- Heart Failure
- Obesity
- Edema
- Nattokinase
- Garlic
- Omega-3 Fatty Acids
- Vitamin K
- Vitamin E
- Turmeric
- Complete Blood Count
- Anemia
- Varicose Veins