Pernicious Anemia
Interactive Visualization Vitamin B12’s Impossible Journey Five stages, two carrier proteins, a working stomach and one specific stretch of gut. Break any link — a PPI, metformin, pernicious anaemia — and absorption collapses. Launch →
Table of Contents
- What is Pernicious Anemia?
- Autoimmune Mechanism
- Causes and Risk Factors
- Symptoms
- Diagnosis and Lab Tests
- Conventional Treatment
- Nutritional and Natural Approaches
- Complications
- Prognosis
- Prevention
- Key Research Papers
- Connections
- Featured Videos
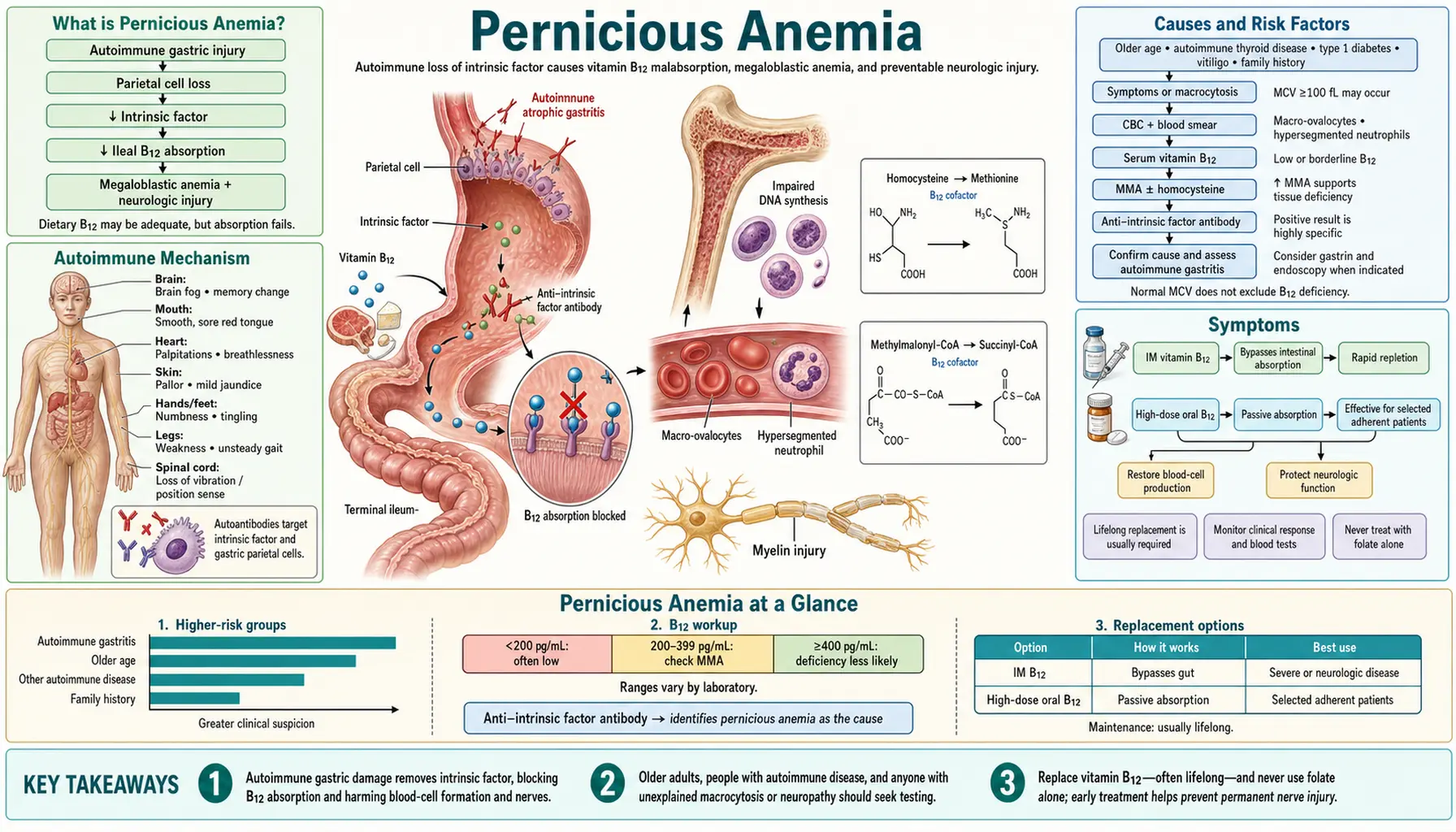
What is Pernicious Anemia?
Pernicious anemia is an autoimmune condition in which the body cannot properly absorb vitamin B12 (cobalamin) from food. The word "pernicious" means deadly or harmful — and before injectable B12 became available in the 1920s, this disease was indeed fatal. Today it is completely manageable, but it remains one of the most underdiagnosed conditions in older adults.
The defining feature of pernicious anemia is the destruction of the stomach's parietal cells by the immune system. These are the cells responsible for producing intrinsic factor — a protein that binds to vitamin B12 in the small intestine and enables its absorption. Without intrinsic factor, even a diet rich in B12 cannot prevent deficiency, because the vitamin simply cannot get into the bloodstream.
Pernicious anemia affects an estimated 1% of the general population and rises to 2–3% of adults over age 60. It is more common in women than men and disproportionately affects people of Northern European descent, though it occurs across all ethnicities. Because its symptoms develop slowly over years and overlap with many other conditions, the average time from first symptoms to diagnosis can be a decade or more.
It is critically important to distinguish pernicious anemia from dietary B12 deficiency. Someone who eats no animal products (vegans, strict vegetarians) may also develop low B12 — but their stomach and intrinsic factor work perfectly fine. Supplementing with standard oral B12 doses fixes dietary deficiency. Pernicious anemia requires much higher oral doses or, classically, bypass via injection, because the gut absorption route is broken at its root.
Autoimmune Mechanism
Pernicious anemia is, at its core, a disease of mistaken identity: the immune system attacks the stomach's own lining as if it were a foreign invader. Understanding this mechanism explains why the treatments work — and why they must continue for life.
The Role of Intrinsic Factor
Vitamin B12 from food is released in the stomach by acid and pepsin, then binds immediately to a protein called haptocorrin (R-binder). In the small intestine, pancreatic enzymes digest this complex, freeing B12 to bind to intrinsic factor (IF) — a glycoprotein secreted by parietal cells in the stomach wall. The IF-B12 complex travels to the terminal ileum (the last section of the small intestine), where it binds to a receptor called cubilin and is absorbed into the bloodstream. Without intrinsic factor, this entire pathway fails.
Anti-Intrinsic Factor Antibodies
In pernicious anemia, the immune system produces anti-intrinsic factor antibodies (anti-IF Abs), which directly disable intrinsic factor in two ways:
- Type I (blocking) antibodies bind to the vitamin B12 binding site on intrinsic factor, preventing IF from ever picking up B12.
- Type II (binding) antibodies bind to the IF-B12 complex itself, blocking it from attaching to the cubilin receptor in the ileum.
These antibodies are highly specific for pernicious anemia — if they are present, the diagnosis is confirmed. However, they are only detectable in about 50–60% of patients, which means a negative test does not rule out the disease.
Anti-Parietal Cell Antibodies and Gastric Atrophy
Most patients with pernicious anemia also carry anti-parietal cell antibodies (APCA), which target a proton pump enzyme (H+/K+ ATPase) on stomach parietal cells. Over years to decades, this immune attack destroys the parietal cell population, leading to autoimmune gastritis — widespread atrophy of the stomach's acid-secreting and intrinsic-factor-secreting glands. The result is:
- Markedly reduced or absent stomach acid (achlorhydria)
- Loss of intrinsic factor secretion
- Reduced pepsin production, impairing early protein digestion
- Elevated gastrin levels (the body attempts to stimulate an atrophied stomach)
APCA are present in 70–90% of pernicious anemia patients but are less specific — they also appear in about 10% of healthy older women. The combination of APCA with low B12 and clinical symptoms is diagnostically meaningful even without positive anti-IF antibodies.
Causes and Risk Factors
Pernicious anemia is fundamentally an autoimmune disease, meaning the root cause is an immune system that attacks its own tissues. No single trigger has been identified, but several factors significantly increase risk.
Genetic Predisposition
Family history is one of the strongest risk factors. First-degree relatives of people with pernicious anemia have a 3- to 5-fold increased risk of developing it themselves. The disease runs in families in a pattern suggesting a polygenic genetic contribution, though no single dominant gene has been identified. Certain HLA types (notably HLA-DR5 and HLA-DR3) are associated with increased susceptibility.
Age
Pernicious anemia is predominantly a disease of middle age and older adults, with peak incidence between ages 60 and 70. However, a juvenile form exists that can affect children under age 10, typically caused by a genetic inability to produce intrinsic factor rather than autoimmune destruction of parietal cells.
Sex
Women are diagnosed with pernicious anemia approximately 1.6 times more often than men — consistent with the general female predominance of autoimmune diseases. However, men tend to be diagnosed later and may have more severe neurological involvement at diagnosis.
Ethnicity and Geography
Pernicious anemia is most prevalent among people of Northern European descent, particularly Scandinavians, Irish, and British populations. It also occurs at higher-than-average rates in African Americans, who tend to develop it at a younger age (mean age ~10 years earlier than white Americans) and with more severe hematological disease. It is less common in Asian and Hispanic populations.
Co-occurring Autoimmune Conditions
Pernicious anemia rarely appears in isolation. It clusters with other organ-specific autoimmune diseases:
- Autoimmune thyroid disease (Hashimoto's thyroiditis, Graves' disease) — the most common association, present in 10–40% of cases
- Type 1 diabetes mellitus
- Addison's disease (autoimmune adrenal insufficiency)
- Vitiligo
- Rheumatoid arthritis
- Myasthenia gravis
When a patient has one autoimmune condition, regular B12 screening becomes especially important.
Helicobacter pylori Infection
H. pylori infection is implicated as a possible trigger for autoimmune gastritis. The bacterium may initiate molecular mimicry — the immune system generates antibodies against H. pylori proteins that cross-react with parietal cell antigens. Studies show higher rates of H. pylori seropositivity in pernicious anemia patients, and eradicating H. pylori in early autoimmune gastritis may slow progression in some patients, though it does not reverse established atrophy.
Medications That Reduce Acid or B12 Absorption
Long-term use of proton pump inhibitors (PPIs) or metformin can independently reduce B12 absorption and should be considered in the differential of low B12 — though they do not cause true pernicious anemia (intrinsic factor remains intact). In patients already predisposed to pernicious anemia, these medications may accelerate the clinical presentation.
Symptoms
Pernicious anemia develops insidiously. Because the liver stores roughly 2–5 years' worth of B12, it can take years of unrecognized malabsorption before symptoms emerge. When they do appear, they span hematological, neurological, gastrointestinal, and psychiatric domains — and not every patient has all of them.
Hematological Symptoms
Low B12 impairs DNA synthesis, which hits the fastest-dividing cells first — including red blood cell precursors in the bone marrow. The result is megaloblastic anemia: large, immature, structurally abnormal red blood cells that don't function properly.
- Fatigue and weakness — often the first complaint; can be profound and disabling
- Pallor — pale skin, pale conjunctiva
- Shortness of breath on exertion
- Palpitations
- Lightheadedness and postural dizziness
- Lemon-yellow tint to skin — caused by mild hemolysis of fragile megaloblasts releasing bilirubin
Neurological Symptoms
The neurological effects of B12 deficiency are the most dangerous aspect of pernicious anemia and can occur even in the absence of anemia. B12 is essential for maintaining the myelin sheath that coats nerve fibers. Without it, nerves demyelinate — a process called subacute combined degeneration (SCD) of the spinal cord, primarily affecting the posterior and lateral columns.
- Paresthesias — tingling, numbness, or "pins and needles," typically starting in the hands and feet and progressing proximally
- Balance problems and ataxia — difficulty walking, especially in the dark (Romberg sign positive)
- Weakness in the legs
- Loss of vibration sense and proprioception
- Spasticity and hyperreflexia (upper motor neuron signs)
- Lhermitte's sign — electric shock sensation down the spine on neck flexion (in severe cases)
- Cognitive decline — memory problems, difficulty concentrating, confusion
Psychiatric Symptoms
Severe B12 deficiency can produce dramatic psychiatric manifestations, sometimes called "megaloblastic madness":
- Depression and mood changes
- Irritability and personality changes
- Paranoia, hallucinations, and frank psychosis
- Cognitive impairment resembling dementia
These symptoms can appear before anemia is detectable on blood tests, which is why B12 levels should be checked in any patient presenting with unexplained neuropsychiatric symptoms.
Gastrointestinal Symptoms
- Glossitis — a smooth, red, painful, swollen tongue (Hunter's glossitis) caused by atrophy of tongue papillae
- Angular cheilitis — cracking at the corners of the mouth
- Nausea and anorexia
- Diarrhea or constipation
- Abdominal discomfort
Achlorhydria (absence of stomach acid due to parietal cell loss) is common and may cause bloating and early satiety.
Diagnosis and Lab Tests
Diagnosing pernicious anemia requires combining clinical suspicion with a panel of blood tests. No single test is definitive on its own.
Serum Vitamin B12
Serum B12 is the first-line screening test. Interpretation guidelines:
- Below 200 pg/mL (148 pmol/L) — consistent with deficiency; treat
- 200–300 pg/mL — grey zone; clinical symptoms and confirmatory tests determine next steps
- Above 300 pg/mL — generally normal (but some laboratories use 200 pg/mL as the lower limit, leaving a diagnostic gap)
Serum B12 has limitations: it measures total B12 including biologically inactive forms. Approximately 50% of patients in the grey zone (200–300 pg/mL) are actually functionally deficient. This is why functional markers are essential when clinical suspicion is high.
Methylmalonic Acid (MMA)
MMA is a metabolite that accumulates when B12-dependent enzymes cannot function. Elevated serum MMA (normal: 70–270 nmol/L) is the most sensitive functional marker of cellular B12 deficiency — it rises before serum B12 falls into the deficient range. MMA is also elevated in renal insufficiency, so kidney function must be considered.
Homocysteine
Homocysteine also accumulates in B12 deficiency (as well as folate deficiency). Elevated total homocysteine (normal: <15 µmol/L) supports B12 deficiency but is non-specific. Together, elevated MMA and elevated homocysteine with normal or low serum B12 make deficiency highly probable.
Complete Blood Count (CBC)
Classic CBC findings in pernicious anemia:
- Macrocytosis: Mean Corpuscular Volume (MCV) >100 fL (normal: 80–100 fL)
- Low hemoglobin — anemia, often severe (<8 g/dL in advanced cases)
- Hypersegmented neutrophils — neutrophils with 5 or more lobes; a hallmark of megaloblastic anemia (finding ≥5% five-lobed neutrophils, or any six-lobed neutrophil is diagnostic)
- Low reticulocyte count — bone marrow is producing cells ineffectively
- Thrombocytopenia and leukopenia may occur in severe cases
Anti-Intrinsic Factor Antibodies
Anti-IF antibodies are highly specific for pernicious anemia (~99% specificity). A positive result confirms the diagnosis. However, sensitivity is only ~50–60%, so a negative result does not rule it out. They should be ordered whenever pernicious anemia is suspected.
Anti-Parietal Cell Antibodies (APCA)
APCA are more sensitive (70–90%) but less specific — they appear in ~10% of healthy older adults and in autoimmune thyroid disease. A positive APCA with low B12 in the right clinical context strongly supports pernicious anemia, especially if anti-IF antibodies are negative.
Gastroscopy and Gastric Biopsy
Upper endoscopy with biopsy can confirm autoimmune gastritis (corpus-restricted atrophic gastritis with intestinal metaplasia). This is important not only for diagnosis but also for gastric cancer surveillance, since autoimmune gastritis carries a 3- to 4-fold increased risk of gastric adenocarcinoma and a higher risk of gastric carcinoid tumors.
Historical: The Schilling Test
The Schilling test — which used radiolabeled B12 to distinguish pernicious anemia from other causes of malabsorption — was the gold standard for decades but is no longer available in most countries. Modern antibody testing and functional markers have largely replaced it.
Conventional Treatment
The goal of treatment is to restore B12 to normal levels, resolve anemia, and — most critically — halt and reverse neurological damage before it becomes permanent. Treatment is lifelong, because the underlying autoimmune gastritis does not resolve.
Intramuscular (IM) Vitamin B12 Injections
For most of the past century, IM injection was the only reliable treatment, since it bypasses the gut entirely. Standard regimens:
- Loading phase: Cyanocobalamin or hydroxocobalamin 1000 mcg IM daily for 7 days, then weekly for 4 weeks
- Maintenance: 1000 mcg IM every 1–3 months for life
Hydroxocobalamin (used in the UK and Europe) is preferred over cyanocobalamin for injections because it is retained in the body longer, allowing less frequent dosing. Cyanocobalamin (more commonly used in the US) is equally effective but requires more frequent maintenance injections.
Injections rapidly correct anemia — reticulocyte count begins rising within 3–5 days, with peak response at 5–10 days. Hemoglobin normalizes within 6–8 weeks. A dramatic increase in reticulocytes (reticulocytosis) after the first injection is itself confirmation of B12 deficiency.
High-Dose Oral Vitamin B12
Approximately 1–2% of orally ingested B12 is absorbed by passive diffusion through the gut wall — a process that does not require intrinsic factor. At high enough doses (1000–2000 mcg/day), this passive absorption is sufficient to maintain B12 levels even in pernicious anemia.
Multiple randomized trials and systematic reviews (including Cochrane analyses) have confirmed that high-dose oral B12 is as effective as IM injections for correcting deficiency in most patients. British and Scandinavian guidelines have incorporated high-dose oral as a standard option. US guidelines are more cautious but increasingly recognize it.
The advantage is obvious: no needles, no clinic visits, lower cost. The main concerns are:
- Adherence — patients must remember to take a high-dose tablet daily
- Variability in passive absorption between individuals
- Uncertainty about adequacy in severe neurological disease (most clinicians still prefer injections initially for neurological pernicious anemia)
Sublingual Vitamin B12
Sublingual B12 (dissolved under the tongue) may provide additional absorption through the oral mucosa, though evidence for superior efficacy over standard oral high-dose is limited. It remains an option for patients who prefer not to swallow pills or receive injections.
Response Timeline
Patients often feel markedly better within days of starting treatment — energy improves rapidly. Anemia resolves over weeks to months. Neurological recovery is slower and less complete — improvement in paresthesias and balance may take 6 months or longer, and damage that has been present for years may be only partially reversible. This is why early diagnosis matters so much: neurological injury that has been present for a short time is far more likely to recover fully than injury sustained over years of unrecognized deficiency.
Monitoring
After initiating treatment, follow-up testing includes:
- Serum B12 and CBC at 1–3 months to confirm response
- MMA and homocysteine if initial levels were elevated (should normalize)
- Potassium monitoring in the first 48 hours of treatment in patients with severe anemia (rapid red cell production can transiently lower potassium — "hungry bone" equivalent)
- Endoscopic surveillance for gastric cancer (every 3–5 years; guidelines vary by country)
Nutritional and Natural Approaches
Nutritional approaches do not replace medical treatment for pernicious anemia — the intrinsic factor deficit is a structural problem that diet alone cannot fix. However, dietary choices and supplementation strategy meaningfully affect overall B12 status, co-nutrient support, and long-term health in people on treatment.
Dietary Vitamin B12 Sources
Even though dietary B12 cannot be properly absorbed in pernicious anemia, understanding B12-rich foods matters for general health context and for family members who may be at risk:
- Beef liver — richest source (70+ mcg per 3 oz serving)
- Clams, oysters, mussels — exceptionally high (84 mcg per 3 oz clams)
- Fish (salmon, tuna, sardines, trout)
- Beef, lamb, pork
- Dairy products (milk, cheese, yogurt)
- Eggs
- Nutritional yeast (fortified varieties)
Methylcobalamin vs. Cyanocobalamin
B12 supplements come in several forms. The debate between methylcobalamin and cyanocobalamin is ongoing:
- Cyanocobalamin is the most studied and stable form, widely used in clinical trials and medical practice. The body must convert it to active forms (methylcobalamin and adenosylcobalamin).
- Methylcobalamin is the active form found in the nervous system and is increasingly popular, particularly among patients who prefer to avoid the tiny cyanide moiety in cyanocobalamin (though toxicologically insignificant at therapeutic doses).
- Hydroxocobalamin is the preferred injection form due to its longer half-life and superior retention.
For oral supplementation in pernicious anemia, both cyanocobalamin and methylcobalamin at doses of 1000–2000 mcg/day appear effective. There is limited head-to-head trial data favoring one form over the other for neurological outcomes.
The Folate Caution
A critical nutritional consideration in pernicious anemia is the relationship between folate and B12. High folate intake (from fortified foods or folic acid supplements) can partially correct megaloblastic anemia without correcting the underlying B12 deficiency. This "masking" effect is dangerous: the blood count improves, giving false reassurance, while B12 deficiency continues to silently damage the nervous system.
This is why high-dose folic acid supplementation should not be started in isolation when B12 status is unknown. In the US, folic acid food fortification began in 1998, and some researchers believe this has led to cases of masked neurological B12 deficiency — particularly in older adults.
B-Complex Support
Folate (B9) participates in the same one-carbon metabolism pathway as B12, and adequate folate is needed for the methylation cycle to function properly once B12 is repleted. However, folate supplementation should only follow B12 repletion, not precede it. B6 supports transsulfuration of homocysteine and provides complementary metabolic support. A balanced B-complex after B12 levels are confirmed normal is a reasonable adjunct.
Iron
After B12 treatment is initiated, the bone marrow rapidly ramps up red cell production. This sudden demand for iron can reveal or unmask underlying iron deficiency — particularly in premenopausal women or patients with achlorhydria (who absorb dietary iron poorly). Monitoring iron stores (ferritin, serum iron, transferrin saturation) at the 4–6 week mark is prudent.
Complications
Untreated or undertreated pernicious anemia carries serious long-term consequences. Several complications can become permanent if the diagnosis is delayed.
Subacute Combined Degeneration (SCD) of the Spinal Cord
This is the most feared neurological complication. B12 deficiency impairs myelin synthesis, causing degeneration of the posterior columns (carrying proprioception and vibration) and lateral columns (carrying corticospinal motor tracts) of the spinal cord. Symptoms include progressive sensory ataxia, weakness, spasticity, and eventual paralysis if untreated. Partial recovery is possible with treatment, but damage present for more than 6–12 months is often irreversible. This is why spinal cord involvement is a neurological emergency warranting immediate B12 repletion.
Peripheral Neuropathy
Demyelination affects peripheral nerves as well as the spinal cord, producing numbness, tingling, burning pain, and weakness in the extremities. Unlike SCD, peripheral neuropathy may recover more completely with treatment, though recovery takes months to years.
Cognitive Impairment and Dementia
B12 deficiency is a recognized — and reversible — cause of cognitive decline. Chronic untreated deficiency can produce a dementia-like syndrome with memory loss, executive dysfunction, and confusion. The crucial point: this is potentially reversible with prompt B12 repletion, making B12 screening an essential step in any dementia workup. However, if dementia has been present for years, improvement may be incomplete.
Increased Gastric Cancer Risk
Chronic autoimmune gastritis leads to progressive mucosal atrophy and intestinal metaplasia — the same precancerous changes seen in H. pylori-driven gastritis. Patients with pernicious anemia have approximately a 3- to 4-fold increased risk of gastric adenocarcinoma and a significantly elevated risk of gastric carcinoid tumors (enterochromaffin-like cell tumors driven by elevated gastrin). Endoscopic surveillance every 3–5 years is recommended in most guidelines.
Infertility
B12 is required for normal DNA replication. Severe deficiency can impair sperm production and maturation, and is associated with ovulatory dysfunction in women. B12 deficiency in early pregnancy is a risk factor for neural tube defects (comparable to folate deficiency) and has been linked to recurrent miscarriage.
Cardiovascular Risk via Elevated Homocysteine
Elevated homocysteine (a consequence of B12 deficiency) is an independent risk factor for atherosclerosis, myocardial infarction, stroke, and venous thromboembolism. Whether B12 supplementation to lower homocysteine reduces cardiovascular events in the general population remains controversial, but correcting frank deficiency clearly normalizes homocysteine and removes this risk contribution.
Prognosis
With appropriate and lifelong treatment, the prognosis for pernicious anemia is excellent. The hematological features (anemia, macrocytosis) resolve completely within weeks to months. Most patients experience a dramatic improvement in energy, mood, and cognitive function within days to weeks of starting treatment.
The key determinant of long-term outcome is whether neurological damage was caught early. Neurological symptoms that have been present for less than 3–6 months have a good chance of complete recovery. Symptoms present for longer — years, in some cases — may improve but often do not resolve fully. This is the strongest argument for aggressive population screening in at-risk groups.
Because pernicious anemia is an autoimmune disease, the gastric atrophy does not reverse with B12 treatment. Patients remain at elevated risk for gastric complications throughout their lives, and endoscopic surveillance should continue indefinitely. The concurrent risk of other autoimmune diseases also persists — patients with pernicious anemia should have thyroid function checked regularly and be evaluated for other autoimmune conditions if new symptoms arise.
Adherence to treatment is the most modifiable prognostic factor. Patients who understand that treatment is permanent — not just until they "feel better" — consistently do best. Education about why injections or high-dose oral therapy must continue for life is an essential part of clinical care.
Prevention
Pernicious anemia itself — being autoimmune — cannot be fully prevented. However, its consequences are almost entirely preventable through early recognition and treatment.
Screening in At-Risk Populations
The following groups warrant proactive B12 screening, even without obvious symptoms:
- Adults over age 65 — B12 deficiency (from pernicious anemia or achlorhydria of aging) affects 5–15% of older adults
- First-degree relatives of patients with pernicious anemia
- Patients with other autoimmune diseases — especially autoimmune thyroid disease, type 1 diabetes, Addison's disease
- Vegans and long-term vegetarians — to distinguish dietary from malabsorptive deficiency
- Long-term users of PPIs or metformin
- Anyone with unexplained fatigue, neuropathy, balance problems, or cognitive decline
Recognizing Early Signs
Public awareness matters. Many patients with pernicious anemia spend years attributed to "aging," "depression," or fibromyalgia before the correct diagnosis is made. Knowing that tingling in the hands and feet, extreme fatigue, balance problems, and a smooth painful tongue are symptoms of a treatable vitamin deficiency — not inevitable aging — can prompt earlier evaluation.
Caution with Folic Acid
Individuals in at-risk populations who are considering high-dose folic acid supplementation (for example, during preconception planning) should have B12 status confirmed first to avoid masking a developing B12 deficiency.
H. pylori Eradication
In patients found to have early autoimmune gastritis with concurrent H. pylori infection, eradicating the bacterium may slow progression of gastric atrophy. While this does not reverse established pernicious anemia, early intervention in at-risk relatives who test positive for H. pylori may reduce future risk.
Key Research Papers
- Lahner E, Annibale B. Pernicious anemia: new insights from a gastroenterological point of view. World J Gastroenterol. 2009;15(41):5121–5128. PMID 19891010. DOI 10.3748/wjg.15.5121
- Toh BH. Diagnosis and classification of autoimmune gastritis. Autoimmun Rev. 2014;13(4–5):459–462. PMID 24424186.
- Stabler SP. Clinical practice. Vitamin B12 deficiency. N Engl J Med. 2013;368(2):149–160 — Search PubMed. DOI 10.1056/NEJMcp1210134
- Green R. Vitamin B12 deficiency from the perspective of a practicing hematologist. Blood. 2017;129(19):2603–2611 — Search PubMed. DOI 10.1182/blood-2016-10-569186
- Andres E, Loukili NH, Noel E, et al. Vitamin B12 (cobalamin) deficiency in elderly patients. CMAJ. 2004;171(3):251–259. PMID 15289425.
- Devalia V, Hamilton MS, Molloy AM; British Committee for Standards in Haematology. Guidelines for the diagnosis and treatment of cobalamin and folate disorders. Br J Haematol. 2014;166(4):496–513 — Search PubMed. DOI 10.1111/bjh.12959
- Carmel R. Efficacy and safety of fortification and supplementation with vitamin B12. Food Nutr Bull. 2008;29(2 Suppl):S177–S187 — Search PubMed.
- Stover PJ. Vitamin B12 and older adults. Curr Opin Clin Nutr Metab Care. 2010;13(1):24–27 — Search PubMed.
- Langan RC, Goodbred AJ. Vitamin B12 Deficiency: Recognition and Management. Am Fam Physician. 2017;96(6):384–389. PMID 28925645.
- Kozyraki R, Cases O. Vitamin B12 absorption: mammalian physiology and acquired and inherited disorders. Biochimie. 2013;95(5):1002–1007 — Search PubMed. DOI 10.1016/j.biochi.2012.11.004
PubMed topic searches:
- Pernicious anemia
- Vitamin B12 deficiency treatment
- Intrinsic factor antibodies
- Autoimmune gastritis B12
Connections
- Vitamin B12’s Impossible Journey — interactive animation
- Vitamin B12
- Anemia
- Vitamin B12 Test
- Complete Blood Count
- Iron-Deficiency Anemia
- Aplastic Anemia
- Thrombocytopenia
- Leukopenia
- Sickle Cell Disease
- Thalassemia
- Hemochromatosis
- Hemophilia
- Von Willebrand Disease
- Deep Vein Thrombosis
- Folate (B9)
- Gastritis
- Peripheral Neuropathy
- Fatigue
- Hematology
- Vitamin B12 for Anemia and Hematology