Leukopenia
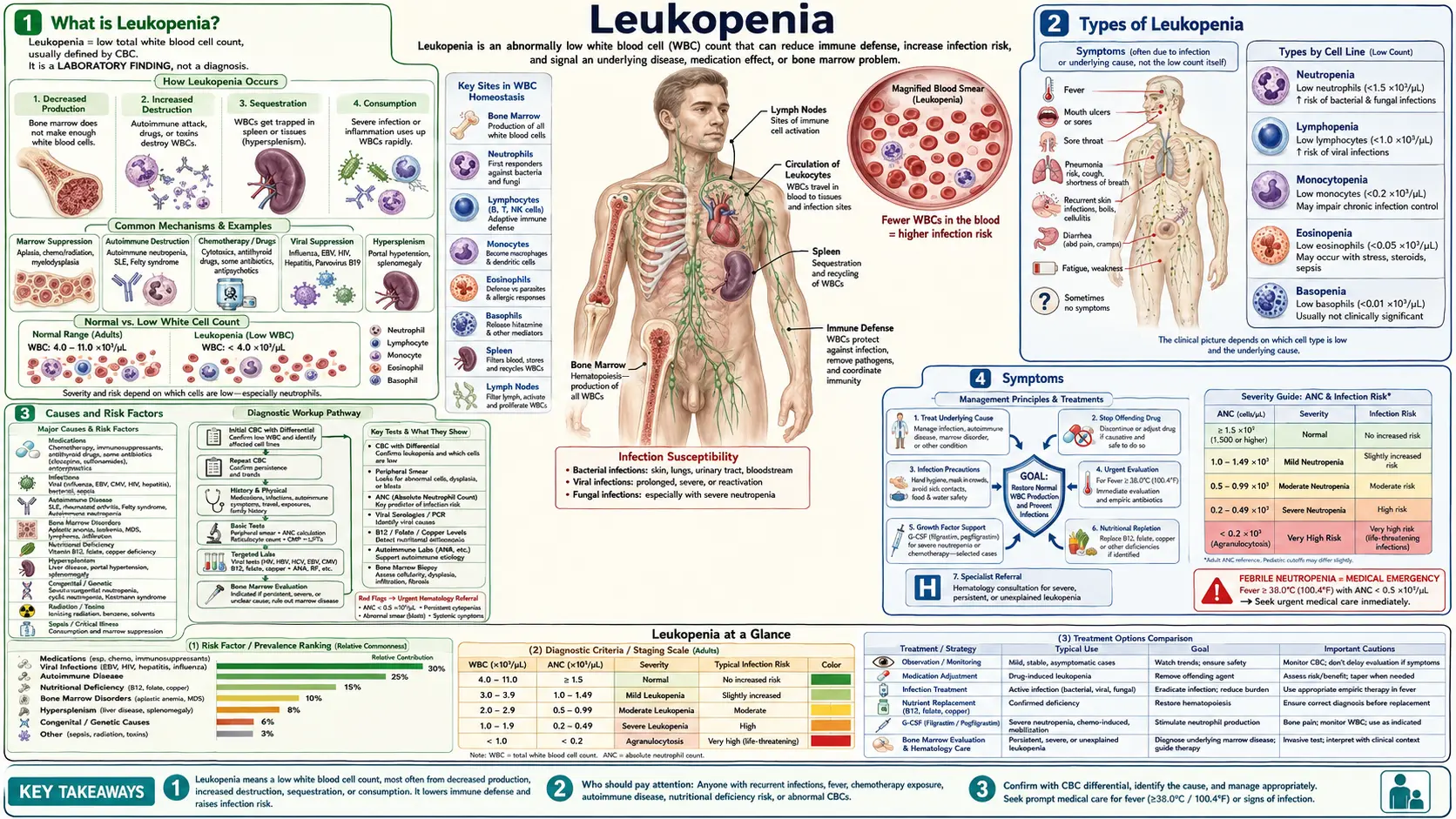
Table of Contents
- What is Leukopenia?
- Types of Leukopenia
- Causes and Risk Factors
- Symptoms
- Diagnosis and Lab Tests
- Conventional Treatment
- Nutritional and Natural Approaches
- Complications
- Prognosis
- Prevention
- Key Research Papers
- Connections
- Featured Videos
What is Leukopenia?
Leukopenia is defined as a white blood cell (WBC) count below 4,000 cells per microliter (4.0 × 10&sup9;/L) in adults. White blood cells are the cellular soldiers of your immune system, and when their numbers drop too low, your body loses a critical layer of defense against infections, bacteria, viruses, and fungi.
Your blood contains several distinct types of white blood cells, each with a specialized role:
- Neutrophils — the most numerous WBC type (50–70% of total WBCs), neutrophils are the first responders to bacterial and fungal infections. They engulf and destroy pathogens through a process called phagocytosis.
- Lymphocytes — comprising B cells (antibody production) and T cells (cell-mediated immunity), lymphocytes account for 20–40% of WBCs and are central to adaptive immune responses.
- Monocytes — large cells (2–8% of WBCs) that differentiate into macrophages and dendritic cells in tissues, coordinating long-term immune responses.
- Eosinophils — involved in allergic responses and parasitic defense (1–4% of WBCs).
- Basophils — the rarest circulating WBC (<1%), basophils release histamine during allergic reactions.
Leukopenia can reflect a reduction in any or all of these cell types. The most clinically dangerous form is neutropenia — a specific drop in the absolute neutrophil count (ANC) below 1,500 cells/mcL — because neutrophils provide the first and fastest defense against life-threatening bacterial infections. When someone with leukopenia develops a fever, it is a medical emergency until proven otherwise.
It is important to distinguish leukopenia (broad WBC reduction) from conditions that selectively reduce just one cell line. The overall WBC count may be only mildly reduced while a specific, critically important subset — particularly neutrophils — is severely depleted.
Types of Leukopenia
Leukopenia is an umbrella term. The specific type is identified by which white blood cell line is reduced, which in turn points toward different causes and carries different risks.
Neutropenia
The most clinically significant form. Defined as an absolute neutrophil count (ANC) below 1,500 cells/mcL. Severity is graded as follows:
- Mild neutropenia: ANC 1,000–1,500 cells/mcL — usually asymptomatic, minimal increased infection risk.
- Moderate neutropenia: ANC 500–1,000 cells/mcL — moderately increased risk; close monitoring required.
- Severe neutropenia: ANC <500 cells/mcL — substantially increased risk of serious bacterial and fungal infections; febrile neutropenia constitutes an oncologic emergency.
- Very severe neutropenia / Agranulocytosis: ANC <200 cells/mcL — life-threatening; even commensal organisms from the gut and skin can cause lethal sepsis.
ANC is calculated from the CBC differential: ANC = WBC × (% neutrophils + % bands) ÷ 100.
Lymphocytopenia
Defined as a lymphocyte count below 1,000 cells/mcL in adults (below 3,000 cells/mcL in children under 2 years). Lymphocytopenia impairs antibody production and cell-mediated immunity, creating vulnerability to viral infections and opportunistic organisms such as Pneumocystis jirovecii. HIV infection is a major cause of progressive CD4+ T-lymphocytopenia.
Monocytopenia
Rare; a monocyte count below 200 cells/mcL. Associated with hairy cell leukemia, aplastic anemia, and some immunodeficiency states. Monocytopenia reduces the ability to clear fungal infections and mount chronic inflammatory responses.
Eosinopenia
An eosinophil count below 100 cells/mcL. Most commonly seen during acute bacterial infections, Cushing syndrome, or steroid treatment — where cortisol drives eosinophils out of circulation into tissues. Generally not itself clinically problematic.
Pan-leukopenia
A reduction in all white blood cell types simultaneously. This pattern suggests global bone marrow failure, as seen in aplastic anemia, myelodysplastic syndrome (MDS), or following aggressive chemotherapy or radiation. Pan-leukopenia is often accompanied by anemia and thrombocytopenia (low platelets), a combination called pancytopenia.
Benign Ethnic Neutropenia
An important variant that affects a significant proportion of people of African, Afro-Caribbean, and some Middle Eastern descent. These individuals have baseline ANC values of 1,000–1,500 cells/mcL as a normal constitutional variant — not due to disease — and do not have increased susceptibility to infection. Misdiagnosis as pathologic neutropenia leads to unnecessary workup and, in some cases, disqualification from otherwise appropriate medications. Recognizing this variant requires knowledge of the patient's ethnic background and documentation of a chronically stable, infection-free course.
Causes and Risk Factors
Leukopenia arises from three fundamental mechanisms: reduced production of WBCs in the bone marrow, accelerated destruction of WBCs in circulation, or abnormal distribution (sequestration) of WBCs out of the bloodstream. Often more than one mechanism operates simultaneously.
Bone Marrow Suppression
When the factory that makes blood cells is damaged or overwhelmed, all cell lines suffer:
- Chemotherapy and radiation therapy — the most common cause in clinical practice. Most cytotoxic agents preferentially target rapidly dividing cells, including bone marrow stem cells. Nadir (lowest WBC point) typically occurs 7–14 days after a chemotherapy cycle.
- Aplastic anemia — immune-mediated destruction of hematopoietic stem cells leads to global bone marrow failure and pancytopenia.
- Myelodysplastic syndrome (MDS) — clonal stem cell disorders producing dysfunctional, ineffective blood cell production. Leukopenia is common and may precede overt leukemia.
- Leukemia and lymphoma — malignant cells crowd out normal hematopoiesis in the bone marrow.
- Metastatic cancer — solid tumor metastases to marrow (breast, prostate, lung cancers) can physically displace normal marrow.
Medications
Drug-induced leukopenia is common and often overlooked. Key offenders include:
- Clozapine — the atypical antipsychotic carries a 1–2% risk of agranulocytosis, the most dangerous drug-induced leukopenia. A mandatory ANC monitoring program (REMS protocol) is required for all clozapine prescriptions.
- Carbamazepine and other anticonvulsants — leukopenia in up to 10% of patients; rarely progresses to aplastic anemia.
- Propylthiouracil (PTU) and methimazole — antithyroid drugs causing agranulocytosis in 0.2–0.5% of patients.
- Methotrexate — suppresses folate-dependent DNA synthesis in rapidly dividing marrow cells.
- Sulfasalazine and hydroxychloroquine — used in autoimmune disease; idiosyncratic leukopenia possible.
- NSAIDs — rare but documented immune-mediated neutropenia.
- Antibiotics — chloramphenicol (dose-independent aplastic anemia); beta-lactams (rare immune-mediated neutropenia with prolonged high-dose IV therapy).
Autoimmune and Inflammatory Conditions
- Systemic lupus erythematosus (SLE) — anti-neutrophil antibodies and anti-lymphocyte antibodies are produced, marking WBCs for early destruction. Leukopenia is part of the formal SLE diagnostic criteria.
- Felty syndrome — the triad of rheumatoid arthritis, splenomegaly, and neutropenia; spleen sequesters and destroys neutrophils.
- Primary autoimmune neutropenia — more common in infants and young children; anti-neutrophil IgG antibodies destroy circulating neutrophils; usually resolves by age 2–4.
Infections
Many infections temporarily suppress WBC production or accelerate WBC destruction:
- HIV — progressive CD4+ lymphocytopenia as the virus destroys T cells; also causes neutropenia through marrow suppression and drug effects.
- Epstein-Barr virus (EBV) / Infectious mononucleosis — transient neutropenia and atypical lymphocytosis.
- Cytomegalovirus (CMV) — particularly in immunocompromised patients.
- Influenza and other respiratory viruses — transient leukopenia common during acute illness.
- Hepatitis B and C — marrow suppression and hypersplenism from cirrhosis.
- Parvovirus B19 — attacks erythroid precursors but can cause transient neutropenia; particularly dangerous in sickle cell disease.
- Bacterial sepsis — acute neutropenia via neutrophil margination (cells adhere to blood vessel walls rather than circulating freely) and accelerated consumption.
- Malaria, tuberculosis, typhoid fever — all cause marrow suppression and WBC sequestration in the spleen.
Nutritional Deficiencies
Underappreciated but correctable causes:
- Vitamin B12 deficiency — impairs DNA synthesis required for rapid WBC production. Produces characteristic hypersegmented neutrophils visible on blood smear.
- Folate (B9) deficiency — same mechanism as B12 deficiency; common in alcohol use disorder and malnutrition.
- Copper deficiency — an underrecognized cause of neutropenia (and anemia) that closely mimics MDS on bone marrow biopsy. Seen after gastric bypass surgery, zinc overdose (zinc displaces copper absorption), and prolonged parenteral nutrition without copper supplementation.
Hypersplenism
An enlarged spleen (from portal hypertension due to cirrhosis, lymphoma, storage diseases such as Gaucher disease, or chronic infection) acts as a WBC sink — sequestering and destroying circulating cells faster than the marrow can replace them. The spleen normally holds about one-third of the platelet pool; in hypersplenism, it traps an abnormally large fraction of all blood cell types.
Congenital and Inherited Causes
- Cyclic neutropenia — an ELANE gene mutation causes ANC to oscillate on a ~21-day cycle, dropping to near zero for 3–5 days, then recovering. Patients develop mouth sores, fevers, and infections predictably with each nadir.
- Severe congenital neutropenia (Kostmann syndrome) — profound neutropenia from birth; requires lifelong G-CSF therapy.
- Chediak-Higashi syndrome — rare autosomal recessive disorder causing dysfunctional neutrophil granules and partial albinism.
- Shwachman-Diamond syndrome — pancreatic insufficiency combined with bone marrow dysfunction and neutropenia.
Symptoms
Leukopenia is frequently asymptomatic when mild — many people discover a low WBC count incidentally on a routine CBC ordered for an unrelated reason. The body's reserves of mature neutrophils (both in marrow and marginated along vessel walls) provide a buffer before clinical consequences appear.
As the WBC count — and especially the ANC — falls further, the immune system's first-response capacity erodes, and characteristic problems emerge:
Recurrent and Prolonged Infections
This is the hallmark consequence. Infections that would be minor in a healthy person become prolonged, severe, or recurrent. Common patterns include:
- Frequent sinusitis, ear infections, or upper respiratory infections
- Pneumonia, sometimes with atypical organisms
- Urinary tract infections that recur or fail standard short-course antibiotics
- Skin infections (cellulitis, furuncles) that spread rapidly or heal slowly
- Perirectal abscesses (a danger sign of severe neutropenia)
Mouth Sores
Aphthous ulcers (painful open sores on the gums, tongue, and inner cheeks) are characteristic of neutropenia, particularly in cyclic neutropenia where they appear predictably during each nadir. The mouth's bacterial burden is normally kept in check by salivary neutrophils; when those disappear, minor mucosal breaks become persistent ulcers.
Fever
In a person with an ANC below 500 cells/mcL, a temperature above 38.3°C (101°F) — or 38.0°C sustained over one hour — is a medical emergency called febrile neutropenia. The fever may be the only sign of a potentially life-threatening infection because the usual inflammatory response (pus, localized pain, swelling) is blunted without adequate neutrophils. Patients should be instructed to go to an emergency department immediately.
Fatigue and Malaise
Non-specific but common, particularly when leukopenia accompanies anemia (as in pancytopenia from aplastic anemia or MDS). Chronic low-grade infections also contribute to persistent fatigue.
Delayed Wound Healing
Neutrophils are essential for clearing bacteria from wounds in the first 24–48 hours. Without adequate neutrophil activity, even minor cuts and surgical incisions heal slowly and are prone to secondary infection.
Opportunistic Infections with Lymphocytopenia
When lymphocytes are specifically depleted (as in advanced HIV or after organ transplant), the immune defects are different and in some ways more insidious — the body loses protection against organisms that a normal immune system holds in check indefinitely:
- Pneumocystis jirovecii pneumonia (PCP) — a fungal pneumonia that causes severe respiratory failure
- Toxoplasma encephalitis
- CMV retinitis or colitis
- Cryptococcal meningitis
- Disseminated Mycobacterium avium complex (MAC)
Diagnosis and Lab Tests
The diagnosis of leukopenia is straightforward — a single CBC with differential establishes it. The real diagnostic work is identifying why the WBC count is low, which requires systematic investigation.
Complete Blood Count (CBC) with Differential
The foundation of diagnosis. A CBC reports the total WBC count and the differential (percentage and absolute number of each WBC type). Key values to extract:
- Total WBC count (normal adult range: 4,500–11,000 cells/mcL)
- Absolute neutrophil count (ANC) — calculated as WBC × (% segs + % bands) / 100
- Absolute lymphocyte count (ALC)
- Hemoglobin and platelet count — pan-cytopenia points toward marrow failure
Serial CBCs over 4–8 weeks can reveal a cyclic pattern, which is diagnostic of cyclic neutropenia.
Peripheral Blood Smear
A trained hematologist examines the size, shape, and structure of blood cells under the microscope. Critical findings include:
- Hypersegmented neutrophils (nuclei with 5+ lobes) — strongly suggest B12 or folate deficiency
- Toxic granulations and Dohle bodies — neutrophil changes indicating infection or sepsis
- Blasts — immature cells that shouldn't be in peripheral blood; suggest leukemia or MDS
- Atypical lymphocytes — seen in EBV/CMV infection
- Pelger-Huet anomaly (bilobed neutrophils) — associated with MDS
Nutritional Testing
- Serum vitamin B12 and methylmalonic acid (MMA) — MMA is a more sensitive marker of functional B12 deficiency
- Red blood cell (RBC) folate — more accurate than serum folate
- Serum copper and ceruloplasmin — critical to exclude copper deficiency, especially post-bariatric surgery or with unexplained neutropenia mimicking MDS
- Zinc levels — elevated zinc can suppress copper absorption
Infectious Disease Testing
- HIV antibody/antigen and CD4+ T cell count if HIV suspected
- EBV and CMV serology (heterophile antibody / monospot, specific IgM/IgG)
- Hepatitis B surface antigen and hepatitis C antibody
- Parvovirus B19 serology
Autoimmune Testing
- Antinuclear antibody (ANA) and anti-double-stranded DNA (dsDNA) — screen for lupus
- Rheumatoid factor and anti-CCP — Felty syndrome
- Anti-neutrophil antibodies (direct and indirect) — for autoimmune neutropenia
Medication Review
A detailed timeline of all prescription medications, over-the-counter drugs, and supplements compared against the timing of the WBC drop is one of the most important diagnostic steps. Drug-induced leukopenia typically appears within days to weeks of starting the offending agent.
Bone Marrow Biopsy and Aspiration
Indicated when the cause remains unclear, when malignancy is suspected, or when the count is severely low. Allows assessment of marrow cellularity, maturation arrest (neutrophils produced but not released), fibrosis, infiltration by malignant cells, and cytogenetics (chromosomal abnormalities pointing to MDS or leukemia). Copper deficiency causes marrow changes that closely mimic MDS — vacuolation of precursors — making copper measurement essential before a marrow biopsy is interpreted.
Conventional Treatment
Treatment targets the underlying cause of leukopenia. There is no single universal therapy — a correct diagnosis drives the intervention.
Treat the Underlying Cause
- Drug-induced leukopenia: discontinue the offending medication. Recovery usually begins within days and is typically complete within 1–3 weeks. For clozapine, discontinuation must be carefully weighed against psychiatric relapse risk, under psychiatric supervision.
- Nutritional deficiency: correct B12 (intramuscular hydroxocobalamin or oral high-dose methylcobalamin), folate, and copper (oral copper gluconate or sulfate 2–4 mg/day for copper deficiency).
- Autoimmune leukopenia: immunosuppression (corticosteroids, IVIG, rituximab) for severe or refractory cases of lupus-related or primary autoimmune neutropenia.
- Hypersplenism: treat the underlying cause of splenomegaly (antiviral therapy for hepatitis, TIPS procedure or liver transplant for portal hypertension); splenectomy is reserved for refractory cases.
Granulocyte-Colony Stimulating Factor (G-CSF)
G-CSF (filgrastim, pegfilgrastim, biosimilars) is a protein that stimulates the bone marrow to produce and release neutrophils rapidly. It is the cornerstone pharmacological treatment for:
- Chemotherapy-induced neutropenia: primary prophylaxis with pegfilgrastim (long-acting G-CSF) is recommended when the risk of febrile neutropenia exceeds 20%, or in patients with additional risk factors (age >65, poor performance status, prior febrile neutropenia). Dramatically reduces hospitalization and allows chemotherapy dose intensity to be maintained.
- Severe congenital neutropenia (Kostmann): lifelong G-CSF maintains ANC above safe thresholds.
- Cyclic neutropenia: daily subcutaneous G-CSF abbreviates the nadir duration and severity.
Febrile Neutropenia: A Medical Emergency
Any patient with ANC <500 cells/mcL who develops fever (T >38.3°C or >38.0°C sustained over one hour) requires immediate hospitalization. Standard management:
- Blood cultures (two sets, including from any central line) before starting antibiotics — but do NOT delay antibiotics waiting for results
- Empiric broad-spectrum IV antibiotics within one hour of presentation: piperacillin-tazobactam or cefepime as first-line monotherapy; add vancomycin for suspected catheter infection or MRSA risk
- G-CSF to shorten neutrophil recovery time
- Antifungal coverage (caspofungin, voriconazole) if fever persists beyond 4–7 days without identified bacterial source
Risk stratification using the MASCC score identifies low-risk patients who may be candidates for oral antibiotics and outpatient management, but this should only be done at centers experienced in this approach.
Antimicrobial Prophylaxis for Prolonged Neutropenia
Patients expected to have ANC <100 cells/mcL for more than 7 days (e.g., after induction chemotherapy for acute leukemia) benefit from:
- Fluoroquinolone prophylaxis (levofloxacin or ciprofloxacin) to reduce gram-negative bacteremia
- Antifungal prophylaxis (fluconazole or posaconazole depending on risk)
- Prophylaxis against Pneumocystis jirovecii (trimethoprim-sulfamethoxazole) when lymphocytopenia is expected
Clozapine REMS Monitoring Protocol
All patients on clozapine must have mandatory ANC monitoring (weekly for the first 6 months, biweekly for the next 6 months, then monthly). If ANC falls below 1,500, clozapine must be interrupted; below 1,000, it is permanently discontinued in most protocols. Prescribers must enroll in the REMS program to prescribe clozapine.
Nutritional and Natural Approaches
Natural approaches to leukopenia are most effective when a specific deficiency or modifiable factor underlies the low WBC count. They are complementary to — not replacements for — conventional treatment in serious cases.
Correct Nutritional Deficiencies First
This is the highest-yield natural intervention:
- Vitamin B12: deficiency causes megaloblastic changes in rapidly dividing marrow cells, impairing WBC production. Oral high-dose B12 (1,000–2,000 mcg/day methylcobalamin or cyanocobalamin) is effective for dietary deficiency; intramuscular hydroxocobalamin is preferred for pernicious anemia or malabsorption. WBC count typically normalizes within 4–8 weeks of correction.
- Folate (B9): folic acid 1–5 mg/day corrects folate-deficiency leukopenia. Adequate intake from leafy greens, legumes, and fortified foods is preventive. People taking methotrexate can take supplemental folate to mitigate (though not eliminate) marrow suppression — discuss dose and timing with prescribing physician.
- Copper: copper deficiency is underdiagnosed but correctable. Oral copper gluconate or copper sulfate (2–4 mg elemental copper daily) normalizes neutrophil count within weeks to months. People who have had gastric bypass surgery, those taking high-dose zinc supplements (>40 mg/day zinc competes with copper absorption), and those on long-term parenteral nutrition are at highest risk.
Zinc
Zinc is required for neutrophil maturation and function. Mild zinc deficiency impairs the oxidative burst that neutrophils use to kill bacteria. Dietary sources include red meat, shellfish (especially oysters), legumes, and nuts. Supplementation at RDA levels (8–11 mg/day) supports immune function; do not exceed 40 mg/day chronically without monitoring copper levels.
Vitamin D
Vitamin D receptors are expressed on nearly all immune cells including neutrophils, monocytes, and lymphocytes. Deficiency (serum 25-OH vitamin D <20 ng/mL) is associated with impaired immune cell differentiation and function. Correcting deficiency with vitamin D3 (1,000–4,000 IU daily, depending on baseline level) supports overall immune competence, though evidence for a direct WBC-raising effect is limited.
Astragalus (Huang Qi)
Astragalus membranaceus root has been used in Traditional Chinese Medicine for centuries as an immune tonic. Preclinical studies suggest polysaccharide components (Astragalus polysaccharides, APS) may stimulate hematopoiesis and WBC production in animal models, and some small Chinese clinical trials have explored its use alongside chemotherapy to reduce neutropenia duration. However, evidence from large, rigorous randomized controlled trials in humans is limited. Some integrative oncology centers incorporate astragalus into supportive care protocols, but patients should discuss this with their oncologist, as herb-drug interactions and quality control of supplements are real concerns.
Beta-Glucans from Medicinal Mushrooms
Beta-1,3/1,6-glucans derived from Shiitake (Lentinula edodes), Maitake (Grifola frondosa), and Reishi (Ganoderma lucidum) are biological response modifiers that activate macrophages and natural killer cells via Dectin-1 receptors. Some clinical studies suggest that orally administered beta-glucans may modulate immune function and potentially reduce chemotherapy-induced immunosuppression, though they do not replace G-CSF for established febrile neutropenia risk management.
Echinacea
Echinacea preparations are widely used for short-term immune support. Evidence for their use specifically in leukopenia is minimal, and they should not be used as primary treatment. Echinacea is generally appropriate for short-term use (up to 10 days) in mild illness prevention but is not established as a treatment for established leukopenia.
Alcohol Reduction
Alcohol is directly toxic to bone marrow and suppresses neutrophil production. Chronic heavy alcohol use also causes folate deficiency. Reduction or elimination of alcohol intake can meaningfully improve WBC counts in people whose leukopenia is alcohol-related.
Infection Prevention Practices During Low-Count Periods
While not a "treatment" in the pharmacological sense, infection prevention is arguably the most important practical intervention for someone with leukopenia:
- Meticulous handwashing (the most evidence-supported infection prevention measure)
- Avoid undercooked meat, raw shellfish, unpasteurized dairy, and unwashed raw produce during periods of severe neutropenia (neutropenic diet, though evidence for strict implementation is mixed)
- Avoid crowds and sick contacts when ANC is below 500
- Maintain good oral hygiene to reduce oral bacteria burden
- Avoid live vaccines during active leukopenia
Complications
The severity of complications from leukopenia is directly proportional to the depth and duration of the WBC reduction, and the underlying cause.
Febrile Neutropenia
The most immediately life-threatening complication. In patients receiving chemotherapy, febrile neutropenia carries an overall mortality of 5–10% in the general population, rising to 20–30% in patients with septic shock or organ failure. Every hour's delay in antibiotic administration increases mortality. This is why febrile neutropenia protocols in oncology centers are treated with the same urgency as a STEMI protocol in cardiology.
Bacteremia and Sepsis
Organisms that the body normally clears within hours can establish bloodstream infections when neutrophils are absent. Gram-negative rods (Pseudomonas aeruginosa, Escherichia coli, Klebsiella species) are particularly dangerous. Their lipopolysaccharide outer membranes trigger massive cytokine release (septic shock), which can cause multi-organ failure within hours. Gram-positive organisms (Staphylococci, Streptococci, viridans streptococci from the mouth) are also common, particularly in patients with central venous catheters or mucositis.
Invasive Fungal Infections
Fungal infections are a particular danger during prolonged, profound neutropenia (>7 days, ANC <100). Invasive aspergillosis from inhaled mold spores can cause necrotizing pulmonary infection. Invasive candidiasis, particularly with fluconazole-resistant Candida glabrata or Candida krusei, is a major cause of mortality in neutropenic patients post-hematopoietic stem cell transplant.
Opportunistic Viral and Parasitic Infections
In lymphopenic states (HIV, organ transplantation, high-dose corticosteroids):
- Pneumocystis jirovecii pneumonia — causes severe hypoxic respiratory failure
- CMV disease — retinitis (can cause blindness), colitis, pneumonitis, encephalitis
- JC virus — progressive multifocal leukoencephalopathy (PML), a devastating brain infection
- Reactivation of latent tuberculosis or endemic fungi (histoplasma, coccidioides)
Transformation to More Severe Hematologic Disease
In patients with myelodysplastic syndrome presenting as leukopenia, there is a 10–40% lifetime risk of progression to acute myeloid leukemia (AML), depending on the MDS subtype and cytogenetic risk category. Regular hematology follow-up with surveillance bone marrow biopsies is essential.
Chronic Organ Damage from Recurrent Infections
In patients with congenital neutropenia on long-term G-CSF, chronic mouth infections and gingivitis are nearly universal and can progress to significant periodontal bone loss. Recurrent lung infections can cause bronchiectasis over years.
Prognosis
The prognosis of leukopenia depends entirely on its cause, depth, and duration. This is one of those conditions where the underlying diagnosis matters far more than the WBC number itself.
Drug-Induced Leukopenia
Generally excellent if recognized promptly. Stopping the offending medication typically leads to WBC recovery within days to 3 weeks. Agranulocytosis from clozapine, once managed with G-CSF support through the nadir, usually resolves fully — but clozapine cannot be safely restarted.
Nutritional Deficiency Leukopenia
Excellent with correction of the deficiency. B12-related neutropenia typically normalizes within 4–8 weeks of replacement therapy. Copper deficiency responds within weeks to months. These are among the most rewarding leukopenia diagnoses to make because they are fully correctable.
Chemotherapy-Induced Neutropenia
Predictable and manageable with appropriate G-CSF support and antibiotic prophylaxis. Modern supportive care has dramatically reduced mortality from febrile neutropenia and allowed more intensive chemotherapy regimens to be given safely.
Autoimmune Leukopenia
Variable. Primary autoimmune neutropenia in infants typically resolves spontaneously by age 2–4. Lupus-associated leukopenia often fluctuates with disease activity and improves with disease control. Felty syndrome can be refractory.
Aplastic Anemia-Associated Leukopenia
Depends on severity and treatment response. Severe aplastic anemia without treatment carries a high mortality; with hematopoietic stem cell transplantation (curative for eligible patients) or immunosuppression (antithymocyte globulin + cyclosporine), survival rates exceed 80–90% at specialized centers.
MDS-Associated Leukopenia
Prognosis stratified by the International Prognostic Scoring System (IPSS-R), incorporating cytogenetics, blast percentage, and cytopenias. Low-risk MDS may remain stable for years; high-risk MDS has median survival of 1–2 years without allogeneic stem cell transplantation.
Congenital Neutropenia
Lifelong condition requiring ongoing management. With modern G-CSF therapy, patients with severe congenital neutropenia lead relatively normal lives, though long-term G-CSF use carries a small but real risk of MDS/AML transformation (cumulative incidence approximately 15–20% over 10 years in Kostmann syndrome).
Prevention
Prevention strategies for leukopenia depend on the clinical context — what is preventable in one setting may not be relevant in another.
Monitoring During Myelosuppressive Therapy
Routine CBC monitoring is standard of care for any patient receiving chemotherapy, radiation therapy, or medications known to suppress bone marrow. Knowing when the nadir is expected (typically 7–14 days after cytotoxic chemotherapy) allows preemptive G-CSF administration and early detection of dangerous nadirs before febrile complications develop.
Primary G-CSF Prophylaxis
For chemotherapy regimens where the febrile neutropenia risk exceeds 20%, or in patients with risk factors (age >65, prior febrile neutropenia, poor nutritional status, comorbidities), pegfilgrastim given 24–72 hours after each chemotherapy cycle is standard preventive practice. This approach reduces hospitalization rates and allows treatment intensity to be maintained.
Mandatory Monitoring for High-Risk Medications
The clozapine REMS program is the most rigorous example — regular ANC monitoring every month (and more frequently initially) has dramatically reduced clozapine-related agranulocytosis deaths compared to the pre-monitoring era. Similar monitoring should be applied to other drugs with known bone marrow risks (carbamazepine, propylthiouracil).
Nutritional Adequacy
Ensuring adequate intake of B12 (particularly in older adults, strict vegans, and those on metformin or proton pump inhibitors long-term), folate (especially in people who drink alcohol regularly or have malabsorption), and copper (especially after bariatric surgery) prevents the nutritional causes of leukopenia. Routine post-bariatric surgery micronutrient panels should include copper and ceruloplasmin.
Infection Prevention During Neutropenic Periods
Hand hygiene, dietary precautions (avoiding high-risk foods during severe neutropenia), prophylactic antibiotics and antifungals per protocol, and patient education about fever recognition and emergency response all contribute to preventing the complications of leukopenia even when the leukopenia itself cannot be prevented.
Vaccination When Counts Allow
Annual influenza vaccination and pneumococcal vaccination (PCV15/20 or PPSV23 as appropriate) are particularly important for immunocompromised patients. Timing matters — vaccines should be given during periods of relative immune recovery, not during the nadir. Live vaccines (MMR, varicella, live attenuated influenza) are contraindicated in patients with significant leukopenia or on immunosuppressive therapy.
Key Research Papers
- Lyman GH, et al. Practical guidance on biosimilars, with focus on oncology supportive care: Filgrastim. Am J Hematol. 2020;95(7):E164–E170 — Search PubMed. DOI 10.1002/ajh.25770
- Crawford J, et al. Myeloid growth factors. J Natl Compr Canc Netw. 2013;11(10):1266–1290 — Search PubMed. DOI 10.6004/jnccn.2013.0148
- Bhatt DL, et al. Clozapine and agranulocytosis: understanding the risk. Br J Psychiatry. 2018;212(6):332–334 — Search PubMed. DOI 10.1192/bjp.2017.40
- Coates TD. Physiology and pathophysiology of the neutrophil. Reference: Neutropenia in adults — Search PubMed.
- Farruggia P, Dufour C. Diagnosis and management of primary autoimmune neutropenia in children: insights for clinicians. Ther Adv Hematol. 2015;6(1):15–24 — Search PubMed. DOI 10.1177/2040620714556642
- Hsieh MM, et al. Prevalence of neutropenia in the U.S. population: age, sex, smoking status, and ethnic differences. Ann Intern Med. 2007;146(7):486–492. PMID 17404350. DOI 10.7326/0003-4819-146-7-200704030-00004
- Palmblad J, Nilsson CC, Höglund P, Papadaki HA. How we diagnose and treat neutropenia in adults. Expert Rev Hematol. 2016;9(5):479–487 — Search PubMed. DOI 10.1586/17474086.2016.1159908
- Tafazoli A. Copper deficiency myelopathy mimicking subacute combined degeneration of the spinal cord and myeloid abnormalities. Eur J Neurol. 2016;23(9):e51–e53 — Search PubMed. DOI 10.1111/ene.13083
- Groopman JE, Itri LM. Chemotherapy-induced anemia in adults: incidence and treatment. J Natl Cancer Inst. 1999;91(19):1616–1634. PMID 10511589. DOI 10.1093/jnci/91.19.1616
- Dale DC, Bolyard AA. An update on the diagnosis and treatment of chronic idiopathic neutropenia. Curr Opin Hematol. 2017;24(1):46–53 — Search PubMed. DOI 10.1097/MOH.0000000000000305
PubMed topic searches:
Connections
- Hematology
- Anemia
- Aplastic Anemia
- Thrombocytopenia
- Pernicious Anemia
- Iron-Deficiency Anemia
- Sickle Cell Disease
- Thalassemia
- Hemochromatosis
- Hemophilia
- Von Willebrand Disease
- Deep Vein Thrombosis
- Complete Blood Count
- Vitamin B12
- Folate (B9)
- Copper
- Zinc
- Lupus (SLE)