Bile Acid Malabsorption in IBS-D
If you have been diagnosed with IBS-D — the diarrhea-predominant form of irritable bowel syndrome — there is roughly a one-in-three chance that what you actually have is bile acid malabsorption (BAM), also called bile acid diarrhea (BAD). It behaves like IBS-D, gets diagnosed as IBS-D, and fails the standard IBS-D treatments because the underlying problem is not irritable bowel at all. It is a plumbing issue in how your small intestine recycles bile acids — and unlike classic IBS, it has a cheap, specific, often dramatically effective treatment: a bile acid sequestrant.
This article walks through what BAM is, why it causes the urgent, watery, morning-and-after-fatty-meal stools that patients describe, how it is diagnosed (and why the diagnosis is much harder in the United States than in the UK), and exactly how the medications that treat it are dosed. If you have been stuck on a low-FODMAP diet, loperamide, and rifaximin without real relief — especially if your diarrhea is worst in the first two hours of the day or after a greasy meal — this is the page for you.
Interactive Visualization The Gut Barrier & Your Microbiome Watch fibre become butyrate and butyrate tighten the gut wall — then starve the microbes and see them eat your mucus layer instead. Launch →Table of Contents
- What Bile Acid Malabsorption Is
- How Common Is It in IBS-D?
- The Mechanism — Why Extra Bile Acids Make You Run
- The Three Types of BAM
- What BAM Feels Like
- How It Is Diagnosed
- Bile Acid Sequestrants — The Treatment
- Dosing, Timing, and Drug Interactions
- Red Flags That Warrant a GI Workup
- Key Research Papers
- Connections
- Featured Videos
What Bile Acid Malabsorption Is
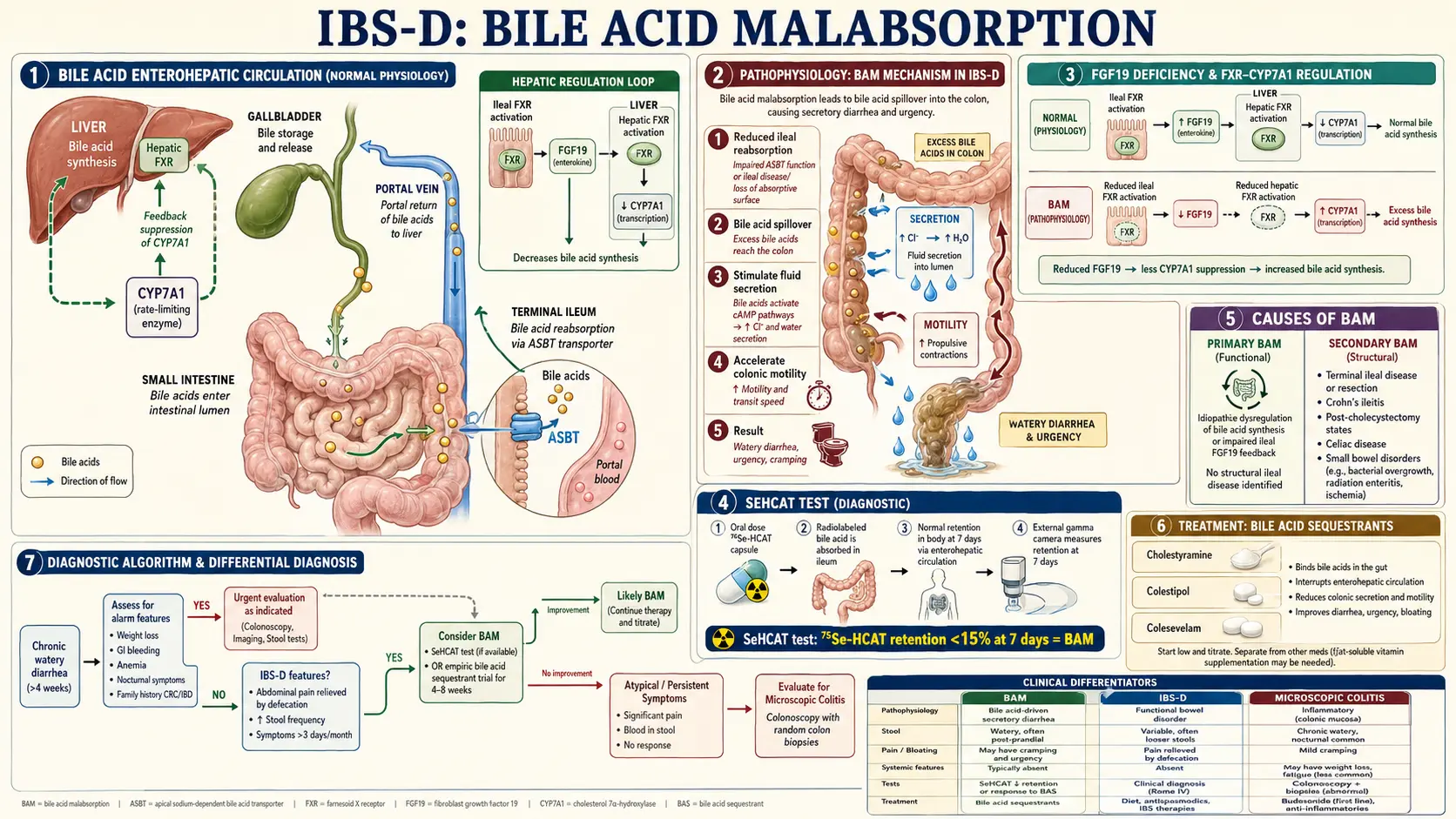
Every day your liver makes about 500–600 mg of bile acids (mostly cholic and chenodeoxycholic acid) and ships them out in bile. Bile is stored in the gallbladder, released into the duodenum after a meal, and used to emulsify dietary fat — breaking large fat globules into tiny droplets so lipases can digest them.
Here is the critical part: bile acids are supposed to be recycled. After doing their job in the upper small intestine, they travel down to the terminal ileum (the last 60–100 cm of the small intestine, right before the colon) where specialized transporters pull them back into the bloodstream. They return to the liver through the portal vein and are reused. This loop — the enterohepatic circulation — runs about six to eight times per day. Under normal conditions, only about 5% of bile acids escape reabsorption and reach the colon.
In BAM, that reabsorption fails. Instead of 5%, something like 15–40% of your bile acids spill into the colon. Once they are there, they cause trouble.
How Common Is It in IBS-D?
This is the number most patients — and many general practitioners — have never heard. Multiple studies, including the landmark 2009 meta-analysis by Wedlake and colleagues, have shown that roughly 25–30% of people diagnosed with IBS-D actually meet criteria for bile acid malabsorption. In some cohorts the figure exceeds 30%.
In plain terms: if you are in a waiting room with nine other IBS-D patients, two or three of you have BAM and do not know it. And of those who are correctly diagnosed and started on a bile acid sequestrant, a large majority report clinically meaningful improvement — often within days.
That prevalence gap is why BAM is sometimes called "the most under-diagnosed treatable cause of chronic diarrhea in Western medicine." The treatment is decades old, off-patent, and cheap. The diagnosis is simply not being pursued.
The Mechanism — Why Extra Bile Acids Make You Run
Bile acids are natural detergents. In the colon, when they arrive in excess concentration, they do three things:
- Stimulate water and electrolyte secretion. Bile acids activate signaling pathways in colonic epithelial cells (including cAMP and calcium-dependent chloride secretion) that pump water and salt into the bowel lumen. The stool becomes watery.
- Speed up colonic motility. Bile acids accelerate the smooth-muscle contractions that push contents through the colon. Faster transit means less time for water reabsorption — compounding the watery stool — and sudden, hard-to-ignore urgency.
- Irritate the colonic mucosa. High concentrations of deoxycholic and chenodeoxycholic acid are mildly inflammatory, contributing to cramping and discomfort.
Put those three effects together and you get the signature BAM stool: urgent, watery, often explosive, frequently yellow or greenish, sometimes floating or greasy-looking, and sometimes accompanied by a burning sensation at the anus. The timing is also distinctive — see the symptoms section below.
The Three Types of BAM
Gastroenterologists classify bile acid malabsorption by mechanism. Knowing your type matters because it points at whether there is another underlying disease to treat.
Type 1 — Ileal disease. The terminal ileum, where bile acids are supposed to be reabsorbed, is structurally damaged or has been surgically removed. Causes include Crohn's disease of the ileum, prior ileal resection (for Crohn's, trauma, or cancer), and radiation damage. Here BAM is a consequence of the underlying disease, and the primary problem still needs management.
Type 2 — Idiopathic / Primary BAM. The ileum looks structurally normal, but the bile-acid feedback loop is broken. The current leading explanation is impaired production of FGF19, a hormone made by ileal cells that normally tells the liver "enough bile acids — stop making more." When FGF19 is low, the liver overproduces bile acids, the ileum cannot reabsorb the flood, and the excess spills into the colon. This is the type most often mistaken for IBS-D. Patients have no structural disease visible on colonoscopy and no prior surgery.
Type 3 — Secondary BAM. The ileum is intact and FGF19 may be fine, but another condition is disrupting the loop. Common culprits:
- Post-cholecystectomy — removal of the gallbladder causes continuous (rather than meal-triggered) bile-acid release, overwhelming ileal reabsorption capacity. This is one of the most common presentations; diarrhea that starts weeks to years after gallbladder removal is often BAM.
- Small intestinal bacterial overgrowth (SIBO) — bacteria in the small intestine deconjugate bile acids prematurely, and deconjugated bile acids are absorbed less efficiently.
- Celiac disease — villous atrophy reduces reabsorption capacity.
- Chronic pancreatitis and pancreatic insufficiency — altered digestive chemistry changes bile-acid handling.
- Post-vagotomy and other upper-GI surgeries.
What BAM Feels Like
BAM and generic IBS-D overlap heavily, but there is a pattern that should raise suspicion:
- Morning urgency. Many patients describe racing to the bathroom two to four times within the first hour or two of getting out of bed, then stabilizing for the rest of the day. This reflects the overnight accumulation of bile in the gallbladder being dumped into the gut with the first meal or even with the standing-up gastrocolic reflex.
- Post-fatty-meal diarrhea. A heavy or greasy meal — pizza, fried food, cream-based sauces, fatty cuts of meat — triggers a flare within one to three hours. Fat is the strongest signal for gallbladder emptying, so fat means more bile delivered to an ileum that cannot keep up.
- Watery or "fluffy" stools. Bristol type 6 or 7, often yellow or greenish.
- Anal burning. A raw, stinging sensation at the anus during or after a bowel movement, from direct bile-acid irritation.
- Urgency out of proportion to cramping. Unlike classic IBS where cramping builds first, BAM urgency can arrive with little warning.
- Nocturnal diarrhea. Some patients are woken by the need to defecate. Nocturnal diarrhea is a red flag in general (see that section below), but in BAM it is part of the pattern.
- Poor response to loperamide alone, low-FODMAP diet, and antispasmodics. These treatments target other IBS mechanisms and rarely fix bile-acid-driven diarrhea.
How It Is Diagnosed
This is where geography matters. The diagnostic options are very different depending on where you live.
SeHCAT scan (UK / EU / Canada). The gold standard. You swallow a capsule containing a synthetic, radiolabeled bile acid (75-selenium homocholic acid taurine). A gamma camera measures how much is retained in your body after 7 days. Normal retention is >15%. Retention of 10–15% is mild BAM, 5–10% is moderate, and <5% is severe. The test is highly accurate and well validated. It is not available in the United States — the FDA has never approved it despite decades of European use.
Serum 7α-hydroxy-4-cholesten-3-one (C4). A blood test measuring a precursor of bile-acid synthesis. When the liver is overproducing bile acids (as in Type 2 BAM), C4 is elevated. Available in specialty labs in the US and Europe; less sensitive than SeHCAT but useful.
Serum FGF19. A fasting blood test measuring the ileal hormone that brakes bile-acid synthesis. Low FGF19 supports Type 2 BAM. Available mainly as a research test; combined with C4 it performs reasonably well.
48-hour fecal bile acid collection. Direct measurement of bile acids in stool. Accurate but unpleasant to collect and not widely offered.
Empiric therapeutic trial. In the United States, where SeHCAT is unavailable and C4/FGF19 are not routinely offered outside academic centers, the most common diagnostic approach is a treatment trial. A gastroenterologist prescribes a bile acid sequestrant (usually cholestyramine or colesevelam) and asks the patient to track symptoms for two to four weeks. A strong, rapid response — diarrhea frequency halved, urgency resolved, morning attacks gone — is treated as diagnostic. A lack of response suggests BAM is not the problem. This pragmatic approach is endorsed in the 2020 British Society of Gastroenterology BAM guidelines as a reasonable second-line strategy when SeHCAT is not available.
Bile Acid Sequestrants — The Treatment
A bile acid sequestrant (also called a bile acid binding resin) is a non-absorbable polymer you swallow. It travels through your gut, binds loose bile acids like a sponge, and leaves with them in the stool. The bile acids can no longer stimulate secretion or irritate the colon. For a patient with BAM, this can transform symptoms within a few days.
There are three sequestrants commonly used for BAM in the US and UK:
- Cholestyramine (Questran, Questran Light, Prevalite). The oldest and cheapest. Sold as a flavored powder you mix with water or juice. Standard starting dose for BAM: 4 g once daily, usually taken with or just before breakfast. Many patients do well on 4 g once daily; some need 4 g twice or three times daily. The major downside is taste and texture — it is gritty and has a sandy mouthfeel many patients dislike.
- Colestipol (Colestid). Similar mechanism, available as granules or tablets. Dosing is roughly 5–10 g daily split into one to three doses. Tablets are large and numerous, but granules are available for those who prefer mixing.
- Colesevelam (Welchol). A newer, higher-potency sequestrant supplied as 625 mg tablets. Typical dose for BAM is 1875–3750 mg daily (three to six tablets), usually split with meals. Far better tolerated than cholestyramine — no powder to mix, minimal taste, less constipation, fewer GI side effects. The tradeoff is cost: it is still on-patent in some formulations and can be expensive without insurance coverage. When tolerability is an issue (and with cholestyramine it often is), colesevelam is worth fighting your insurance for.
All three work through the same mechanism. If one is not tolerated, try another before concluding that sequestrants do not work for you.
Dosing, Timing, and Drug Interactions
Sequestrants are safe and non-absorbed, but their binding is indiscriminate — they will grab many other medications along with bile acids, dragging your other prescriptions out in the stool unabsorbed. This makes timing critical.
The 4-hour rule. Take all other oral medications at least 1 hour before OR 4 hours after your sequestrant dose. The 4-hour buffer is the standard recommendation; 1 hour before is acceptable for medications taken on an empty stomach.
Medications most affected. Pay particular attention to:
- Levothyroxine (thyroid hormone) — absorption is dramatically reduced if co-administered.
- Warfarin — INR can swing.
- Digoxin.
- Oral contraceptives — efficacy can be reduced.
- Statins — especially if you are on them for cholesterol.
- Fat-soluble vitamins (A, D, E, K). Long-term high-dose sequestrant use can modestly reduce absorption of these; periodic vitamin D monitoring is reasonable.
Practical schedule for many patients. Take the sequestrant with breakfast (so it is in the gut when the gallbladder dumps its overnight load of bile), take thyroid medication or other daily prescriptions first thing in the morning on an empty stomach at least 1 hour before breakfast, and space other meds to the afternoon or evening. If you take a second sequestrant dose, place it with dinner and keep evening medications 4 hours away.
Common side effects. Constipation (paradoxically — and sometimes welcome after years of diarrhea), bloating, flatulence, and mild nausea. Titrate up slowly: start with 4 g cholestyramine once daily (or 3 colesevelam tablets with a meal) and increase only if needed. A minority of patients need the higher end of the range to control symptoms; most do well at modest doses.
Red Flags That Warrant a GI Workup
Before assuming your diarrhea is BAM or IBS and treating empirically, make sure none of the following are present. These are signs that something more serious — inflammatory bowel disease, colorectal cancer, microscopic colitis, celiac disease, or infection — may be driving the symptoms, and they warrant a full workup with your gastroenterologist.
- Blood in the stool (red, maroon, or black/tarry).
- Unintentional weight loss — more than a few pounds you did not try to lose.
- Nocturnal diarrhea waking you consistently from sleep — though common in BAM, it also flags IBD and should at least get imaging and labs.
- Onset after age 50 with no prior GI history.
- Family history of colorectal cancer, IBD, or celiac disease.
- Fever, severe abdominal pain, or dehydration.
- Anemia or iron deficiency on routine labs.
- Elevated inflammatory markers (CRP, ESR) or elevated fecal calprotectin.
- Recent antibiotic use — consider C. difficile testing.
- Rapid change in bowel habit in someone previously regular.
BAM is a diagnosis of exclusion in the sense that you want to be confident you are not missing inflammatory bowel disease, celiac disease, microscopic colitis, or colorectal neoplasia before settling on it. That workup typically includes stool studies (calprotectin, ova/parasites, C. difficile), blood work (CBC, CRP, TSH, celiac serology), and in most adults at least one colonoscopy with random biopsies to rule out microscopic colitis. Once the picture is clean, a therapeutic trial of a sequestrant is reasonable, safe, and often revealing.
Key Research Papers
- Wedlake L, et al. Systematic review: the prevalence of idiopathic bile acid malabsorption as diagnosed by SeHCAT scanning in patients with diarrhea-predominant irritable bowel syndrome. Aliment Pharmacol Ther. 2009;30(7):707-17.
- Slattery SA, et al. Systematic review with meta-analysis: the prevalence of bile acid malabsorption in the irritable bowel syndrome with diarrhoea. Aliment Pharmacol Ther. 2015;42(1):3-11.
- Arasaradnam RP, et al. Guidelines for the investigation of chronic diarrhoea in adults: British Society of Gastroenterology, 3rd edition. Gut. 2018 (BSG chronic diarrhea guidelines covering BAM diagnostics).
- Walters JR, Pattni SS. Managing bile acid diarrhoea. Therap Adv Gastroenterol. 2010;3(6):349-57.
- Walters JR, et al. A new mechanism for bile acid diarrhea: defective feedback inhibition of bile acid biosynthesis. Clin Gastroenterol Hepatol. 2009;7(11):1189-94. (FGF19 hypothesis.)
- Camilleri M. Bile acid diarrhea: prevalence, pathogenesis, and therapy. Am J Gastroenterol. 2020.
Live PubMed Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on bile acid malabsorption, its diagnosis, and its treatment:
- Bile acid malabsorption in IBS-D
- SeHCAT scanning for bile acid diarrhea
- FGF19 and bile acid diarrhea
- Serum C4 (7α-hydroxy-4-cholesten-3-one) in chronic diarrhea
- Cholestyramine for bile acid diarrhea
- Colesevelam for bile acid malabsorption
- Post-cholecystectomy diarrhea and bile acids
- Terminal ileal Crohn's and bile acid malabsorption
- SIBO and bile acid deconjugation
- Bile acid sequestrant drug interactions and timing
Connections
- The Gut Barrier & Your Microbiome — interactive animation
- Irritable Bowel Syndrome
- Celiac Disease
- SIBO
- Inflammatory Bowel Disease
- Rome IV Subtypes
- IBS and SIBO Overlap
- Low-FODMAP Diet for IBS
- IBS Medications Guide
- Post-Infectious IBS
- Peppermint, Probiotics, and Herbals
- Gut-Directed Hypnotherapy and CBT
- Visceral Hypersensitivity and Brain-Gut Axis
- Chronic Diarrhea
- Constipation
- Bloating
- Taurine
- Calcium
- Pancreatitis