Selenium, Zinc, Iron, and Iodine for Hashimoto's
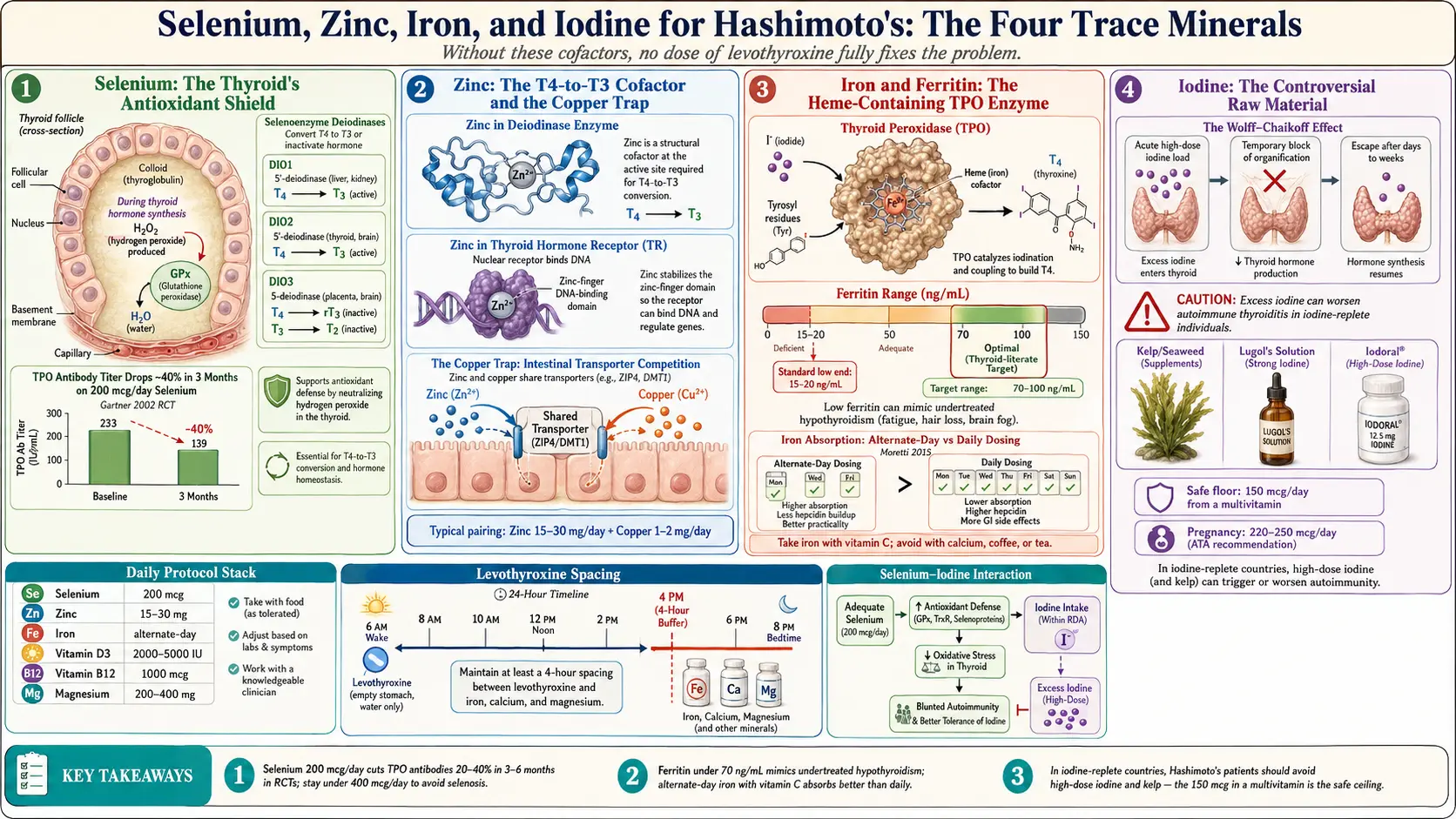
Table of Contents
- Why Trace Minerals Matter
- Selenium — The Thyroid's Antioxidant Shield
- Selenium — What the Trials Show
- Selenium Dosing and Forms
- Selenium Toxicity — The Upper Limit
- Zinc — The T4-to-T3 Cofactor
- Zinc Dosing and the Copper Problem
- Zinc Testing — What Actually Works
- Iron and Ferritin — The Missing Piece
- Iron Dosing — Alternate-Day Is Better
- Ferritin Targets for Thyroid Patients
- Iron Pitfalls
- Iodine — The Controversial One
- When Iodine Is OK
- Kelp and Seaweed — Why to Be Careful
- The Selenium-Iodine Interaction
- Other Relevant Cofactors
- A Practical Stack for Hashimoto's
- Cost, Brands, and Quality
- Timing Around Levothyroxine
- Key Research Papers
- Connections
- Featured Videos
Why Trace Minerals Matter
Your thyroid is not a standalone organ. It is a chemistry lab that depends on a specific set of trace minerals to build hormones, convert them to their active form, and protect itself from the oxidative damage generated as a byproduct of that very chemistry. When these minerals are low, no dose of levothyroxine fully fixes the problem — because the drug replaces T4, but T4 still has to be converted to T3, and that conversion needs minerals the pill cannot provide.
Four minerals dominate the thyroid literature: selenium, zinc, iron, and iodine. Each sits at a specific enzymatic step. Selenium powers the deiodinase enzymes that strip an iodine atom off T4 to make T3. Zinc is a structural cofactor for the same deiodinases and for the thyroid hormone receptor itself. Iron is required for thyroid peroxidase (TPO), the enzyme that builds thyroid hormone in the first place. Iodine is the raw material — four atoms per T4, three per T3.
In Hashimoto's, the system is already under immune attack. Running it on depleted cofactors is like asking a damaged engine to perform on low-octane fuel. This article walks through each mineral in order of clinical impact: what it does, how to test it, how to dose it, how much is too much, and what to do when standard labs come back "normal" but you still feel sick.
Selenium — The Thyroid's Antioxidant Shield
The thyroid gland contains the highest concentration of selenium per gram of any tissue in the body. That is not a coincidence. Making thyroid hormone generates hydrogen peroxide as a necessary intermediate, and hydrogen peroxide is toxic to the cells producing it. Selenium-containing enzymes neutralize the peroxide before it can damage thyroid tissue.
Three selenium-dependent jobs matter for Hashimoto's:
- Glutathione peroxidase (GPx). The thyroid's antioxidant defense. Without enough selenium, GPx activity drops and thyroid follicles accumulate oxidative damage, feeding the autoimmune attack.
- Deiodinases (DIO1, DIO2, DIO3). All three selenoproteins. These enzymes convert T4 to active T3 (DIO1, DIO2) or inactivate thyroid hormone (DIO3). No selenium, no T3.
- TPO antibody reduction. Multiple trials have shown that selenium supplementation drops TPO antibody titers by 20–40% over 3–6 months. This does not cure the disease, but it correlates with less inflammation and, in many patients, better day-to-day energy.
Selenium — What the Trials Show
Selenium is one of the few Hashimoto's supplements with real randomized trial evidence:
- Gärtner 2002 (the seminal RCT). 72 Hashimoto's patients, 200 mcg/day sodium selenite for 3 months. TPO antibodies dropped ~40% in the treatment group versus minimal change in placebo. Nine patients normalized their antibodies completely.
- Turker 2006. Compared 200 mcg/day to lower doses; 200 mcg/day was the minimum effective dose for TPO reduction, and the effect plateaued above that.
- Toulis meta-analysis 2010. Pooled data from four RCTs; confirmed that 3 months of selenium supplementation significantly lowers TPO antibodies in Hashimoto's patients, though heterogeneity in trial quality was substantial.
- CATALYST trial (larger pragmatic study). Mixed findings on quality-of-life endpoints, reminding us that antibody reduction is a surrogate marker. Lower antibodies do not automatically equal symptom relief for every patient — but they correlate often enough to justify a trial.
The honest summary: selenium is one of the most evidence-backed interventions in Hashimoto's, but do not expect miracles. Think of it as tuning the engine, not rebuilding it.
Selenium Dosing and Forms
Standard dose: 200 mcg per day. Take with food, typically breakfast.
Form matters. In order of bioavailability and retention:
- Selenomethionine — the amino-acid-bound form; well absorbed and incorporates into body stores. A solid default.
- Selenium yeast (high-selenium yeast) — a mix of selenomethionine and other organic selenoamino acids; used in most of the big RCTs and comparable to pure selenomethionine.
- Sodium selenite / selenate — inorganic forms; absorbed but not retained as well. Gärtner 2002 used selenite successfully, so it works, but organic forms are the modern preference.
Food source: Brazil nuts. One to two Brazil nuts per day is the classic folk-medicine approach and can deliver 70–200 mcg depending on the nut. The problem is extreme variability: selenium in Brazil nuts comes from the soil where the tree grew, and a single nut can range from 10 mcg to over 90 mcg. If you rely on Brazil nuts, do not stack a supplement on top — you can overshoot without knowing it.
Selenium Toxicity — The Upper Limit
Selenium has a narrow therapeutic window. The U.S. tolerable upper intake level for adults is 400 mcg/day, and chronic intake above that causes selenosis. Signs include:
- Brittle, ridged, or shedding nails
- Hair loss (paradoxical — you thought selenium was supposed to help)
- A distinct garlic odor on the breath and sweat (a classic tell)
- Peripheral neuropathy — tingling or numbness in the hands and feet
- Gastrointestinal upset, fatigue, and irritability
The practical rules: do not exceed 200 mcg/day from a dedicated supplement. Check your multivitamin — many contain 50–100 mcg of selenium, which stacks on top. If you eat Brazil nuts daily, skip the supplement. And if you start growing garlic-scented sweat, stop and your levels will normalize within a few weeks.
Zinc — The T4-to-T3 Cofactor
Zinc is less studied than selenium in Hashimoto's but its role is well established. Three thyroid-relevant functions:
- Deiodinase structure. Zinc is a structural cofactor in the deiodinases that selenium powers. Zinc-deficient animals show reduced T4-to-T3 conversion even when selenium status is normal.
- TSH receptor and thyroid hormone receptor function. Zinc is required for the three-dimensional folding of the nuclear thyroid hormone receptor. Without zinc, T3 can bind but downstream gene transcription suffers.
- Immune modulation. Zinc balances Th1/Th2/Th17 signaling. Deficiency tilts toward autoimmune inflammation; repletion calms it.
Patients with hypothyroidism often have low zinc on blood testing, and zinc-deficient patients often have low T3 — a chicken-and-egg relationship that, in practice, is treated by repleting both.
Zinc Dosing and the Copper Problem
Standard dose: 15–30 mg elemental zinc per day, taken with food (zinc on an empty stomach causes nausea in most people).
Forms worth buying:
- Zinc picolinate — well absorbed, widely available, inexpensive.
- Zinc glycinate (bisglycinate) — gentle on the stomach; good for people who get queasy on picolinate.
- Zinc citrate — decent absorption, cheap.
- Avoid zinc oxide — poorly absorbed; fine for sunscreen, not for supplementation.
The copper trap. Zinc and copper compete for the same intestinal transporter. Taking 30 mg/day of zinc for more than 4–6 weeks without copper induces copper deficiency, which itself causes anemia, neuropathy, and immune dysfunction — exactly the symptoms you were trying to fix. Pair zinc with 1–2 mg of copper (as copper bisglycinate or copper gluconate), taken at a different time of day. Many zinc products are sold as "zinc + copper" combos for this reason.
Zinc Testing — What Actually Works
Zinc testing is notoriously unreliable. Standard serum zinc has a broad reference range (typically 60–120 mcg/dL) and can look normal even in functional deficiency, because the body pulls zinc out of tissues to keep serum stable. It is also affected by recent meals and time of day.
Better options:
- Red blood cell (RBC) zinc — reflects longer-term status; less affected by acute fluctuation. Available through most specialty labs.
- Plasma zinc after a 12-hour fast, drawn in the morning — the most reproducible version of the standard test.
The pragmatic approach. If serum zinc is in the lower third of the reference range and you have suggestive symptoms — slow wound healing, frequent colds, changes in taste or smell, new white spots on fingernails, hair thinning — a 2–3 month trial of 15–30 mg/day with copper is reasonable and low-risk. Re-test after 3 months and reassess symptoms.
Iron and Ferritin — The Missing Piece
Iron is the most commonly missed thyroid cofactor in primary care. A classic presentation: the thyroid labs look "optimal" on paper — TSH around 1.5, free T4 mid-range, free T3 acceptable — and the patient still has fatigue, hair loss, cold intolerance, and brain fog. Check ferritin. It is often under 30 ng/mL.
Why iron matters for thyroid:
- TPO enzyme. Thyroid peroxidase, the enzyme that builds T4 from iodine and tyrosine, is a heme-containing enzyme. Iron-deficient TPO cannot synthesize hormone at full capacity.
- T4-to-T3 conversion. Low iron impairs deiodinase activity indirectly via mitochondrial dysfunction.
- Hair, nails, skin. Three tissues that fail first when either iron or thyroid hormone is low. Combined deficiency is devastating.
- Oxygen delivery. Low ferritin without overt anemia still compromises tissue oxygenation, which the patient experiences as crushing fatigue even at a hemoglobin of 12.
Standard labs call anemia at hemoglobin below 12 (women) or 13.5 (men). But the thyroid patient with ferritin of 25 and hemoglobin of 13 is functionally iron-deficient — the stores are empty even though the circulating red cell count has not yet fallen.
Iron Dosing — Alternate-Day Is Better
A 2015 landmark study by Moretti and colleagues in the journal Blood changed how we dose iron. Daily dosing triggers a hormone called hepcidin that blocks intestinal iron absorption for 24–48 hours after each dose. In plain English: alternate-day dosing absorbs more iron than daily dosing and causes fewer side effects.
Practical protocol:
- Dose: 40–65 mg elemental iron, every other day, in the morning on an empty stomach.
- Take with 250–500 mg of vitamin C to enhance absorption.
- Avoid coffee, tea, dairy, and calcium supplements for 2 hours before and after — all block absorption.
- Space from levothyroxine by at least 4 hours. Iron binds levothyroxine in the gut and torpedoes its absorption. Most patients take thyroid medication on waking and iron mid-morning or lunchtime on alternate days.
Forms, in order of tolerability:
- Ferrous bisglycinate — gentle on the gut, well absorbed; the modern first choice. Typical dose 25–27 mg elemental per capsule.
- Heme iron polypeptide — very well absorbed, expensive.
- Ferrous sulfate — cheapest, proven; rougher on the stomach and more likely to cause constipation and black stools.
- Ferrous fumarate / gluconate — middle of the road on both counts.
Ferritin Targets for Thyroid Patients
General population reference ranges (ferritin above 15 or 20 ng/mL) are too low for thyroid patients. A thyroid-literate target is 70–100 ng/mL. Hair-loss clinicians often push for 70 minimum; some endocrinologists are happy at 50.
Retest ferritin, CBC, and iron saturation at 3 months. If ferritin has not moved at least 20 points, investigate why: ongoing blood loss (heavy periods, GI bleeding), celiac disease or gluten-related malabsorption, H. pylori infection, or poor stomach acid (common in Hashimoto's because autoimmune gastritis frequently overlaps).
Once you hit 70–100 ng/mL, drop to a maintenance dose or stop and recheck in 6 months. Continuing to supplement past a good ferritin level risks iron overload, which is its own problem.
Iron Pitfalls
- Do not supplement without labs. Iron overload (hemochromatosis) is genetic and more common than most people realize; supplementing blindly can accelerate organ damage. Check ferritin and transferrin saturation before starting.
- Screen for hemochromatosis if a first-degree relative has it, or if your ferritin comes back unexpectedly high (over 300 ng/mL with no obvious cause).
- Too much iron causes oxidative stress. Iron drives Fenton-reaction free radicals; in excess it feeds the exact oxidative damage selenium is protecting the thyroid from.
- Men and postmenopausal women rarely need iron supplementation and should be extra cautious — they are not losing iron monthly and accumulate it more readily.
Iodine — The Controversial One
Iodine is the single most misunderstood nutrient in the Hashimoto's world. The logic sounds airtight: the thyroid makes iodine-containing hormones, so iodine must help. In practice, for Hashimoto's patients in an iodine-replete country like the United States, high-dose iodine supplementation often makes the disease worse.
The mechanism has two parts:
- The Wolff-Chaikoff effect. A sudden surge of iodine temporarily shuts down thyroid hormone production. Most healthy thyroids escape this within a few days; Hashimoto's thyroids often do not, and hypothyroidism worsens.
- Antigenic modification. Iodine incorporation into thyroglobulin makes it a more visible target for autoimmune antibodies. Studies in iodine-deficient regions show that iodine repletion programs are followed by an uptick in Hashimoto's incidence. This is not a reason to reverse public-health iodization — it prevents far more goiter and developmental disability than it causes — but it tells you that iodine is not benign in autoimmune thyroid disease.
The populations at highest risk from high-dose iodine are exactly the patients most likely to be self-medicating: those who have already been diagnosed with Hashimoto's, who read online that "iodine fixes thyroid," and who start 12.5 mg or 50 mg daily doses of Lugol's solution or Iodoral. This is a common route into worsening disease and rising TPO titers.
When Iodine Is OK
Iodine is not always bad. The cases where supplementation is appropriate:
- Documented deficiency. Spot urinary iodine concentration under 100 mcg/L (ideally confirmed on a 24-hour urine or a second spot test) is the standard cutoff for population-level deficiency.
- Pregnancy and breastfeeding. Fetal brain development requires iodine. The American Thyroid Association recommends 150 mcg/day preconception and 220–250 mcg/day in pregnancy, usually delivered through a prenatal multivitamin. Even Hashimoto's patients should hit this floor.
- Restrictive diets. Strict vegans who avoid iodized salt, dairy, eggs, and seafood can become deficient. A standard multivitamin dose of 150 mcg/day is reasonable.
The safe everyday dose for an adult with Hashimoto's is the 150 mcg included in most multivitamins. Above that, ask for a urinary iodine level first.
Kelp and Seaweed — Why to Be Careful
Kelp, kombu, bladderwrack, and other seaweeds are marketed as "natural thyroid support." The problem is dose unpredictability. A single serving of kelp can contain 500 to 10,000 mcg of iodine, depending on species, harvest location, and processing — routinely ten to fifty times the recommended daily intake.
Case reports and small series link daily kelp consumption to new-onset thyroiditis, worsening Hashimoto's, and iodine-induced hyperthyroidism. If you have Hashimoto's:
- Avoid daily kelp or seaweed supplements unless your clinician is monitoring urinary iodine and TSH.
- Occasional sushi (a nori wrap, a miso soup) is fine. Daily miso, daily seaweed snacks, and kelp capsules are where people get in trouble.
- Check your multivitamin and any "thyroid support" blend for hidden kelp — it is a surprisingly common ingredient.
The Selenium-Iodine Interaction
Selenium and iodine work as a team. Iodine is the raw material for hormone synthesis; selenium protects the thyroid from the oxidative damage that synthesis generates. When iodine intake rises without enough selenium, the thyroid is flooded with peroxide it cannot neutralize, and follicular cells suffer.
Animal models and observational human data suggest that selenium adequacy blunts iodine-induced thyroid autoimmunity. In practical terms: if a Hashimoto's patient must take iodine (pregnancy, documented deficiency), ensuring selenium sufficiency first is prudent. Never supplement high-dose iodine without selenium on board — it is the combination most likely to spike TPO antibodies.
Other Relevant Cofactors
A brief tour of the supporting cast:
- Vitamin D. Low vitamin D is nearly universal in autoimmune thyroid disease. Target a 25-hydroxyvitamin D level of 40–60 ng/mL. Most Hashimoto's patients need 2,000–5,000 IU/day of D3, with K2 (100–200 mcg MK-7) as a useful companion for calcium metabolism.
- Vitamin B12. Autoimmune gastritis and parietal-cell antibodies cluster with Hashimoto's, and B12 deficiency is common. Keep serum B12 above 500 pg/mL; supplement 1,000 mcg methylcobalamin daily if low.
- Tyrosine. Thyroid hormone is built from tyrosine plus iodine. Tyrosine deficiency is rare in anyone eating adequate protein. Supplementation rarely helps unless you are on a very restricted diet.
- Magnesium. A cofactor in hundreds of enzymes, including some in the deiodinase pathway. Most people are low. 200–400 mg/day of magnesium glycinate or citrate is a safe, broadly useful add-on.
A Practical Stack for Hashimoto's
Pulling it together into a starting protocol most Hashimoto's patients tolerate well:
- Selenium 200 mcg/day (selenomethionine or selenium yeast) with breakfast.
- Zinc 15–30 mg/day with dinner, paired with copper 1–2 mg/day taken at a different meal.
- Iron — dose based on ferritin. If ferritin is under 70 ng/mL, 40–65 mg elemental ferrous bisglycinate every other day with vitamin C, on an empty stomach, at least 4 hours from levothyroxine.
- Vitamin D3 2,000–5,000 IU/day with a fat-containing meal if your 25(OH)D is under 40 ng/mL. Retest at 3 months.
- Vitamin B12 1,000 mcg methylcobalamin if serum B12 is under 500 pg/mL.
- Magnesium 200–400 mg/day in glycinate or citrate form, taken at bedtime.
- Iodine: skip supplementation unless a urinary iodine test shows deficiency, you are pregnant, or you are on a strict vegan diet. A 150 mcg multivitamin is fine; high-dose iodine is not.
Retest TPO antibodies, TSH, free T4, free T3, ferritin, vitamin D, and B12 at 3 months. Adjust based on numbers and symptoms, not online consensus.
Cost, Brands, and Quality
Supplements are an unregulated industry. Look for third-party certifications on the label: USP Verified, NSF Certified, or GMP-compliant. Brands with a consistent track record for third-party testing:
- Thorne — clinician-grade, more expensive, cleaner excipient lists.
- Pure Encapsulations — hypoallergenic, practitioner channel, reliable.
- Jarrow Formulas — mid-priced, good quality.
- NOW Foods — the most affordable of the reputable brands; widely tested.
- Life Extension — similar tier to Jarrow.
Approximate monthly cost for the whole stack above, at NOW or Jarrow pricing: $30–$50. At Thorne or Pure Encapsulations: $60–$100. Generic drugstore multivitamins are inexpensive but often use oxide forms of minerals (poorly absorbed) and may contain hidden kelp or iodine — read the label.
Timing Around Levothyroxine
Thyroid hormone absorption is easy to sabotage. A short cheat sheet:
- Take levothyroxine on waking, with water only, at least 30–60 minutes before food or coffee.
- Iron, calcium, magnesium: space at least 4 hours from levothyroxine.
- Selenium and zinc: take with food to reduce nausea. Timing relative to thyroid medication matters less, but keeping them at lunch or dinner is simplest.
- Vitamin D and B12: no strong interaction with levothyroxine; take whenever convenient. Vitamin D wants fat to absorb.
- Coffee: delays levothyroxine absorption by up to an hour even without cream. Wait at least 30 minutes after the pill, ideally 60.
The simplest schedule that works for most people: thyroid pill on waking, coffee and breakfast an hour later with selenium, zinc and dinner, iron on alternate days at lunch with vitamin C, magnesium at bedtime. Write it on a card and tape it to your medicine cabinet until it becomes automatic.
Key Research Papers
Foundational and recent peer-reviewed publications on the four micronutrients most implicated in thyroid function — selenium, zinc, iron, and iodine — plus the absorption-and-dosing literature that shapes practical use. Each citation links to the full text via DOI.
- Gärtner R, Gasnier BCH, Dietrich JW, Krebs B, Angstwurm MWA. Selenium Supplementation in Patients with Autoimmune Thyroiditis Decreases Thyroid Peroxidase Antibodies Concentrations. Journal of Clinical Endocrinology & Metabolism. 2002;87(4):1687–1691.
- Toulis KA, Anastasilakis AD, Tzellos TG, Goulis DG, Kouvelas D. Selenium Supplementation in the Treatment of Hashimoto's Thyroiditis: A Systematic Review and a Meta-Analysis. Thyroid. 2010;20(10):1163–1173.
- Wichman J, Winther KH, Bonnema SJ, Hegedus L. Selenium Supplementation Significantly Reduces Thyroid Autoantibody Levels in Patients with Chronic Autoimmune Thyroiditis: A Systematic Review and Meta-Analysis. Thyroid. 2016;26(12):1681–1692.
- Mazokopakis EE, Papadakis JA, Papadomanolaki MG, et al. Effects of 12 Months Treatment with L-Selenomethionine on Serum Anti-TPO Levels in Patients with Hashimoto's Thyroiditis. Thyroid. 2007;17(7):609–612.
- Zimmermann MB, Boelaert K. Iodine Deficiency and Thyroid Disorders. Lancet Diabetes & Endocrinology. 2015;3(4):286–295.
- Moretti D, Goede JS, Zeder C, et al. Oral Iron Supplements Increase Hepcidin and Decrease Iron Absorption from Daily or Twice-Daily Doses in Iron-Depleted Young Women. Blood. 2015;126(17):1981–1989.
- Stoffaneller R, Morse NL. A Review of Dietary Selenium Intake and Selenium Status in Europe and the Middle East. Nutrients. 2015;7(3):1494–1537.
- Rayman MP. Multiple Nutritional Factors and Thyroid Disease, with Particular Reference to Autoimmune Thyroid Disease. Proceedings of the Nutrition Society. 2019;78(1):34–44.
- Sategna-Guidetti C, Volta U, Ciacci C, et al. Prevalence of Thyroid Disorders in Untreated Adult Celiac Disease Patients and Effect of Gluten Withdrawal: An Italian Multicenter Study. American Journal of Gastroenterology. 2001;96(3):751–757.
- Betsy A, Binitha MP, Sarita S. Zinc Deficiency Associated with Hypothyroidism: An Overlooked Cause of Severe Alopecia. International Journal of Trichology. 2013;5(1):40–42.
- Hess SY. The Impact of Common Micronutrient Deficiencies on Iodine and Thyroid Metabolism: The Evidence from Human Studies. Best Practice & Research Clinical Endocrinology & Metabolism. 2010;24(1):117–132.
- Centanni M, Gargano L, Canettieri G, et al. Thyroxine in Goiter, Helicobacter pylori Infection, and Chronic Gastritis. New England Journal of Medicine. 2006;354(17):1787–1795.
Live PubMed Searches
Live PubMed queries that update as new papers are indexed.
- PubMed: selenium RCTs Hashimoto's
- PubMed: ferritin + thyroid + hair loss
- PubMed: iodine + Hashimoto's controversy
- PubMed: zinc + T4-to-T3 conversion
- PubMed: alternate-day iron + hepcidin
- PubMed: vitamin D + autoimmune thyroiditis
- PubMed: Wolff-Chaikoff + iodine excess
- PubMed: selenium-iodine interaction
Connections
- How Your Thyroid Is Controlled — interactive animation
- Selenium
- Iodine
- Zinc
- Iron
- Magnesium
- Hashimoto's Thyroiditis
- Vitamin D3
- Vitamin B12
- TSH, T4 & T3 Optimal Ranges
- AIP and Gluten Elimination
- Levothyroxine vs NDT vs T3
- TPO and TgAb Antibodies
- Reverse T3 and Low T3 Syndrome
- Copper & Iron Dysregulation
- Copper
- Tyrosine
- Anemia
- Celiac Disease