TSH, Free T4, Free T3 Optimal Ranges
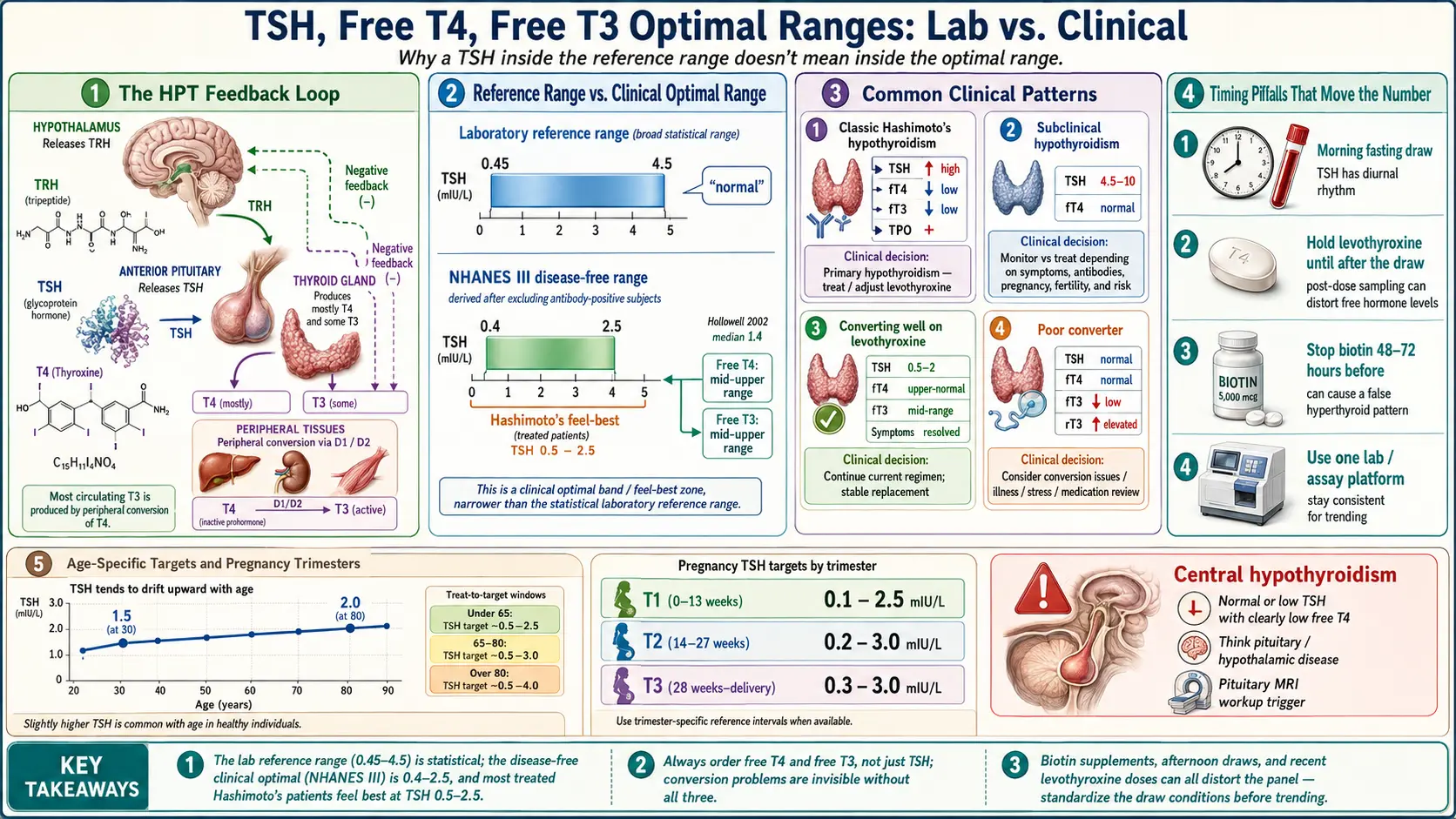
Table of Contents
- How TSH Works — The Pituitary Feedback Loop
- The Lab Reference Range vs. the Clinical "Optimal" Range
- Where Hashimoto's Patients Tend to Feel Best
- Free T4 — The Storage Hormone
- Free T3 — The Active Hormone at the Cell
- Reverse T3 and the fT3:rT3 Ratio
- TPO and TgAb — Always at Baseline
- The Full Panel to Request
- Common Clinical Patterns
- Timing of Blood Draws — Details That Move the Number
- Pharmacy and Lab Differences
- Age-Specific Ranges
- Gender and Lifecycle
- When to Suspect Central Hypothyroidism
- How to Advocate for the Full Panel
- Home Testing Options
- Key Research Papers
- Connections
- Featured Videos
How TSH Works — The Pituitary Feedback Loop
Thyroid-stimulating hormone (TSH) is not made by your thyroid. It is made by your pituitary gland, a pea-sized organ tucked at the base of your brain. The pituitary acts as a thermostat. It constantly samples the level of thyroid hormone floating in your blood, compares it to a set point, and dials its output of TSH up or down to keep the level steady.
The loop runs like this. Your hypothalamus releases TRH (thyrotropin-releasing hormone), which tells the pituitary to release TSH. TSH then travels to the thyroid and stimulates it to produce T4 (mostly) and T3 (a little). When T4 and T3 levels rise, they loop back and suppress TRH and TSH release. When thyroid hormone drops, TRH and TSH rise. A falling thyroid pushes TSH up; a rising thyroid pulls TSH down.
That is why TSH is the first test doctors order. It is a proxy for how your pituitary perceives your thyroid status. A high TSH means the pituitary is shouting at a slow thyroid. A low TSH means the pituitary is telling a hot thyroid to quiet down. But proxies can mislead. TSH reflects what the pituitary sees, not necessarily what every cell in your body feels.
The Lab Reference Range vs. the Clinical "Optimal" Range
Open any lab report and TSH will usually have a reference range of roughly 0.45 to 4.5 mIU/L. Anything inside is flagged as "normal." Anything outside is flagged as abnormal. This simple binary is the source of more frustrated Hashimoto's patients than almost any other single fact in medicine.
Reference ranges are statistical, not biological. A lab takes a sample of "apparently healthy" people, measures their TSH, and reports the middle 95%. That is it. The problem: the reference population is usually not screened for thyroid autoimmunity. Undiagnosed Hashimoto's patients end up inside the reference cohort, widening the "normal" range upward.
In 2002, the landmark NHANES III analysis by Hollowell and colleagues re-examined the U.S. population after rigorously excluding people with detectable thyroid antibodies, personal or family history of thyroid disease, or medications affecting the thyroid. In this "disease-free" subset, 95% of people fell between a TSH of 0.4 and 2.5 mIU/L, with a median near 1.4. The upper quarter of the old reference range — 2.5 to 4.5 — was populated disproportionately by people who actually had subclinical disease.
This is why many endocrinologists and functional-medicine practitioners distinguish between the laboratory reference range (statistical, 0.45–4.5) and the clinical optimal range (what healthy people without autoimmunity actually show, roughly 0.4–2.5). When your TSH is 3.8 and your doctor says "normal," both of you can be right and wrong at the same time.
Where Hashimoto's Patients Tend to Feel Best
Symptom studies and clinical observation converge on a narrower window for treated Hashimoto's patients:
- TSH: 0.5–2.5 mIU/L — most patients on levothyroxine report best energy, mood, cognition, and menstrual regularity in this band.
- Free T4: mid-to-upper third of the reference range.
- Free T3: mid-to-upper third of the reference range.
These are not regulatory targets. The American Thyroid Association's 2014 guideline for adult hypothyroidism accepts a TSH anywhere inside the laboratory reference range as adequate. The narrower "feel best" band is an observation from people who live in their own bodies and report how those bodies function at different numbers. Use it as a hypothesis to test with your clinician, not as a weapon to demand medication changes.
Free T4 — The Storage Hormone
Total T4 in your blood is mostly bound to carrier proteins (thyroxine-binding globulin, transthyretin, albumin). Bound hormone is biologically inert. Only the small unbound fraction — free T4 — can enter cells, be converted to T3, and do work. Free T4 is the measurement that matters.
Typical reference ranges are 0.8 to 1.8 ng/dL (sometimes reported as 10–23 pmol/L), though labs vary. Many clinicians treating Hashimoto's aim for a free T4 in the 1.2 to 1.6 ng/dL zone — comfortably mid-to-upper range, not suppressed.
Free T4 is the steadier of the active hormones. It has a long half-life (about a week), so day-to-day fluctuation is small. It is your storage pool. Conversion enzymes in the liver, kidney, muscle, and brain take T4 and remove one iodine atom to make T3, the active form. A low free T4 means the storage tank is low; a mid-to-upper free T4 means your cells have something to work with.
Free T3 — The Active Hormone at the Cell
T3 is the hormone that actually binds the thyroid hormone receptor inside your cells and switches on the genes that govern metabolism. It is three to four times more potent than T4. Of the T3 in your bloodstream, roughly 80% is made outside the thyroid by enzymatic conversion of T4; the thyroid itself produces only a fraction directly.
Typical reference ranges are 2.3 to 4.2 pg/mL (3.5–6.5 pmol/L). A clinical target often cited for symptomatic patients is 3.2 to 3.8 pg/mL — upper-middle of the range.
Free T3 has a short half-life (roughly a day) and fluctuates more than free T4. It is also the most likely test to reveal a conversion problem: a patient on enough levothyroxine to produce a pretty free T4 but whose deiodinase enzymes are not efficiently turning T4 into T3. The TSH and free T4 look textbook, the patient still feels cold, tired, foggy, and constipated — and free T3 is sitting near the bottom of its range. Without that third number, the conversion problem is invisible.
Reverse T3 and the fT3:rT3 Ratio
T4 can be deiodinated in two ways. Removing one iodine from the outer ring yields active T3. Removing one from the inner ring yields reverse T3 (rT3), a structural mirror image that binds the receptor without activating it. Reverse T3 is a natural brake — a way for the body to throttle metabolism during stress, starvation, severe illness, trauma, and intense caloric restriction.
A high rT3 is generally not a thyroid problem; it is a signal of systemic stress. Common drivers include chronic infection, prolonged caloric deficit, over-training, sleep deprivation, cortisol excess, liver disease, and critical illness. Many practitioners use the free T3 to reverse T3 ratio as a rough indicator of conversion health, targeting a ratio above 20 (when fT3 is in pg/mL and rT3 in ng/dL). Mainstream endocrinology considers this ratio controversial — assay standardization is poor and prospective outcome data are thin — but the test is cheap, so many patients order it once to rule out a gross problem.
For a deeper treatment of rT3 biology, low-T3 syndrome, and non-thyroidal illness, see the Reverse T3 article.
TPO and TgAb — Always at Baseline
Anti-thyroid peroxidase (TPO) and anti-thyroglobulin (TgAb) antibodies are the immunologic fingerprint of Hashimoto's disease. TPO is positive in about 90% of Hashimoto's cases; TgAb is positive in about 60–80%. Together they catch almost everyone. These belong on every initial thyroid workup, because a "normal TSH" in an antibody-positive person carries very different implications from a normal TSH in an antibody-negative person.
For how to interpret antibody titers, trend them over time, and use them to track disease activity, see the sibling article on TPO and TgAb antibodies.
The Full Panel to Request
Ask for these tests at baseline, ideally before starting any thyroid medication:
- TSH — pituitary signal.
- Free T4 — active, unbound storage hormone.
- Free T3 — active hormone at the cell.
- Reverse T3 — conversion brake; useful once to rule out a gross problem.
- TPO antibodies — autoimmune fingerprint.
- Thyroglobulin antibodies (TgAb) — the other autoimmune fingerprint.
Once you are on therapy and stable, the typical follow-up set is TSH, free T4, and free T3, drawn every 6–8 weeks after a dose change and every 6–12 months once stable. Antibodies and reverse T3 do not need repeating at every visit; once or twice a year is plenty unless something changes clinically.
Common Clinical Patterns
The same set of numbers tells different stories depending on how they move together. A few recurring patterns:
Classic Hashimoto's hypothyroidism. TSH elevated (often >4.5), free T4 low or low-normal, free T3 low or low-normal, TPO strongly positive. Clear diagnosis; levothyroxine is the first-line response.
Subclinical hypothyroidism. TSH 4.5–10, free T4 still inside the reference range, symptoms variable. Treatment is debated. Most guidelines recommend treating if TSH is above 10, if the patient is pregnant or trying to conceive, if symptoms are disabling, or if antibodies are positive and TSH is trending upward. Otherwise, watchful monitoring every 6–12 months is acceptable.
Converting well on levothyroxine. TSH 0.5–2, free T4 upper-normal, free T3 mid-range, symptoms resolved. This is the outcome most patients and clinicians are aiming for.
Poor converter. TSH normal, free T4 normal or high-normal, free T3 low, sometimes rT3 elevated. The patient still has cold hands, stubborn weight, fatigue, and brain fog. This is the pattern that drives the clinical conversation about adding T3 (liothyronine) or switching to natural desiccated thyroid — see the levothyroxine vs NDT vs T3 article.
Thyroid hormone resistance or treatment failure. Numbers look optimal by every yardstick and the patient still feels unwell. Before concluding resistance, rule out iron deficiency, ferritin below 50, low vitamin D, B12 deficiency, sleep apnea, depression, perimenopause, adrenal insufficiency, and the POTS/MCAS overlap syndromes. "Optimal thyroid" is not always the full story.
Timing of Blood Draws — Details That Move the Number
Small procedural details meaningfully shift thyroid numbers. Standardize them so you are trending real physiology, not noise:
- Draw in the morning, fasting. TSH follows a daily rhythm, peaking overnight and hitting its lowest point in the afternoon. An afternoon draw can read a full point lower than a morning one in the same person.
- Hold your levothyroxine dose until after the draw. Levothyroxine absorbed hours before a test can transiently spike your free T4 reading and undervalue your true baseline. Take the pill immediately after blood is drawn.
- Stop biotin 48–72 hours beforehand. High-dose biotin (commonly 5,000–10,000 mcg in hair/skin/nail supplements) interferes with many immunoassay platforms and can artifactually lower TSH and raise free T4 and free T3 — mimicking hyperthyroidism on paper. This is a famous real-world source of misdiagnosis.
- Be consistent. Always draw at about the same time of day, under the same fasting conditions, relative to the same medication timing. Trending requires reproducibility.
Pharmacy and Lab Differences
Not all labs run the same assay. Free T3, free T4, and especially reverse T3 are measured on different analyzer platforms (Roche, Siemens, Abbott, DiaSorin, LC-MS/MS reference methods) with subtly different reference ranges and calibrations. A free T3 of 3.2 pg/mL at LabCorp is not numerically identical to a 3.2 at Quest.
Practical rule: use the same lab for every draw you plan to trend. Switching labs midstream introduces noise that can look like disease activity when nothing has changed.
Pharmacy also matters. Levothyroxine brands (Synthroid, Levoxyl, Tirosint, Unithroid, generic) are not truly bioequivalent for everyone, despite FDA labeling. If you are stabilized on one brand and the pharmacy silently substitutes another, your numbers can drift. Ask your prescriber to mark "dispense as written" and stay with one manufacturer.
Age-Specific Ranges
The TSH upper limit drifts upward with age. Studies of healthy older adults show a median TSH of 1.5 at age 30 and nearly 2.0 at age 80, with the 97.5th percentile rising past 5 or 6 in people over 70. Treating an 80-year-old to a TSH of 1 may cause more harm (atrial fibrillation, bone loss) than benefit.
Rough age guidance many geriatricians use:
- Adults under 65: target TSH 0.5–2.5.
- Ages 65–80: target TSH roughly 1–4.
- Over 80: a TSH of 4–7 may be physiologic and well-tolerated.
At the other end, infants and children have higher TSH set points than adults and require pediatric-specific ranges.
Gender and Lifecycle
Sex per se does not shift reference ranges much, but lifecycle events do. Estrogen raises thyroxine-binding globulin, which increases total T4 without changing free T4 — one of several reasons total T4 is not a useful test anymore.
Pregnancy imposes much tighter targets because fetal brain development depends on maternal thyroid hormone, especially in the first trimester before the fetal thyroid is active. Broadly, first-trimester TSH targets of 0.1–2.5, second trimester 0.2–3.0, and third trimester 0.3–3.0 are cited, with free T4 kept in the upper half of a trimester-specific range. Pre-conception counseling and medication adjustment at the positive pregnancy test are standard. See Pregnancy and Hashimoto's for the full protocol.
Menopause can unmask or aggravate Hashimoto's. Many women first receive a diagnosis in the perimenopausal window because symptom overlap (fatigue, weight gain, brain fog, hair thinning, mood shifts) triggers the lab workup that finally catches the antibodies.
When to Suspect Central Hypothyroidism
Primary hypothyroidism is thyroid failure: the thyroid is dying, so thyroid hormones fall and TSH climbs. Central hypothyroidism is pituitary failure: the pituitary cannot produce TSH, so despite a starving thyroid, TSH stays normal or even low. Free T4 and free T3 fall anyway, because the signal to the thyroid is missing.
It is rare but regularly missed, because the reflex "TSH is normal, you are fine" habit blinds clinicians to a low free T4. Suspect central hypothyroidism when:
- TSH is normal or low but free T4 is clearly below range.
- A history of pituitary surgery, radiation, head trauma, or postpartum hemorrhage with severe blood loss (Sheehan syndrome).
- Other pituitary hormone deficiencies are present — low cortisol, low sex hormones, diabetes insipidus.
- Mass-effect symptoms: new headaches, visual field changes.
Workup includes pituitary MRI and a full anterior-pituitary hormone screen. This is one of the strongest reasons to always look at free T4 alongside TSH, rather than stopping at TSH alone.
How to Advocate for the Full Panel
Many primary care offices run only TSH, sometimes with reflex free T4. Getting free T3, reverse T3, and antibodies often requires specifically asking. Scripts that work:
- "Would you order a full thyroid panel including free T3 and reverse T3? I want to see conversion, not just TSH."
- "I have Hashimoto's disease, so my antibodies confirm I have an autoimmune thyroid condition. I would like my TSH, free T4, and free T3 checked together so we can see the whole picture."
- "I understand TSH is usually sufficient for screening. I am asking for the full panel because I am still symptomatic and want to rule out a conversion issue before I assume nothing is wrong."
If your insurance pushes back on reverse T3, know that it is usually inexpensive to pay cash ($30–60 at most labs). Antibody testing is almost always covered once at baseline.
If your current clinician declines, you have three ethical options: ask again at your next visit with more specifics about your symptoms, seek a second opinion with an endocrinologist or functional-medicine physician, or order direct-to-consumer testing and bring the results to your next appointment.
Home Testing Options
Direct-to-consumer thyroid testing has become reliable and affordable in the last decade. Well-established options in the United States include:
- Paloma Health — at-home finger-stick thyroid panel (TSH, free T4, free T3, TPO) with optional physician consultation. Designed specifically for Hashimoto's monitoring.
- Everlywell — finger-stick thyroid tests in several tiers; widely available.
- LetsGetChecked — similar mail-in finger-stick model, with CLIA-certified lab processing.
- Ulta Lab Tests, Private MD Labs, Walk-In Lab — order standard venous draws at a local Quest or LabCorp draw station without a physician's order, in most U.S. states. Typically the cheapest way to get a full panel including reverse T3.
Two caveats. First, finger-stick capillary assays are accurate but can differ slightly from venous assays — pick one method and stay with it for trending. Second, home testing gives you data, not treatment. A full panel with abnormal numbers is a starting point for a conversation with a licensed prescriber, not a do-it-yourself prescription.
Becoming lab-literate is a form of self-advocacy. You are not trying to replace your doctor; you are trying to arrive at the appointment with enough understanding to ask the right questions, interpret the answers, and recognize when "your numbers are normal" is the end of the story or the beginning of it.
Key Research Papers
Foundational and recent peer-reviewed publications on the TSH reference range debate, the clinical utility of free T3, the subclinical-hypothyroidism treatment literature, and the assay-interference issues that complicate panel interpretation. Each citation links to the full text via DOI.
- Hollowell JG, Staehling NW, Flanders WD, et al. Serum TSH, T4, and Thyroid Antibodies in the United States Population (NHANES III). Journal of Clinical Endocrinology & Metabolism. 2002;87(2):489–499.
- Jonklaas J, Bianco AC, Bauer AJ, et al. Guidelines for the Treatment of Hypothyroidism (American Thyroid Association). Thyroid. 2014;24(12):1670–1751.
- Wartofsky L, Dickey RA. The Evidence for a Narrower Thyrotropin Reference Range Is Compelling. Journal of Clinical Endocrinology & Metabolism. 2005;90(9):5483–5488.
- Surks MI, Goswami G, Daniels GH. The Thyrotropin Reference Range Should Remain Unchanged. Journal of Clinical Endocrinology & Metabolism. 2005;90(9):5489–5496.
- Rodondi N, den Elzen WPJ, Bauer DC, et al. Subclinical Hypothyroidism and the Risk of Coronary Heart Disease and Mortality. JAMA. 2010;304(12):1365–1374.
- Razvi S, Shakoor A, Vanderpump M, Weaver JU, Pearce SHS. The Influence of Age on the Relationship Between Subclinical Hypothyroidism and Ischemic Heart Disease: A Metaanalysis. Journal of Clinical Endocrinology & Metabolism. 2008;93(8):2998–3007.
- Bunevicius R, Kazanavicius G, Zalinkevicius R, Prange AJ Jr. Effects of Thyroxine as Compared with Thyroxine plus Triiodothyronine in Patients with Hypothyroidism. New England Journal of Medicine. 1999;340(6):424–429.
- Gulseren D, Gulseren L, Bozkurt N, Hekimsoy Z. Free Thyroxine and Free Triiodothyronine Reference Intervals: A Critical Appraisal. Clinical Endocrinology. 2016;84(1):153–158.
- Surks MI, Hollowell JG. Age-Specific Distribution of Serum Thyrotropin and Antithyroid Antibodies in the U.S. Population: Implications for the Prevalence of Subclinical Hypothyroidism. Journal of Clinical Endocrinology & Metabolism. 2007;92(12):4575–4582.
- Hoermann R, Midgley JEM, Larisch R, Dietrich JW. Recent Advances in Thyroid Hormone Regulation: Toward a New Paradigm for Optimal Diagnosis and Treatment. Frontiers in Endocrinology. 2017;8:364.
- Barbesino G. Misdiagnosis of Graves' Disease with Apparent Severe Hyperthyroidism in a Patient Taking Biotin Megadoses. Thyroid. 2016;26(6):860–863.
- Caturegli P, De Remigis A, Rose NR. Hashimoto Thyroiditis: Clinical and Diagnostic Criteria. Autoimmunity Reviews. 2014;13(4-5):391–397.
Live PubMed Searches
Live PubMed queries that update as new papers are indexed.
- PubMed: TSH reference range narrowing
- PubMed: free T3 clinical utility
- PubMed: reverse T3 clinical significance
- PubMed: subclinical hypothyroidism Rx
- PubMed: levothyroxine + T3 conversion
- PubMed: biotin assay interference
- PubMed: age-specific TSH ranges
- PubMed: central hypothyroidism
Connections
- How Your Thyroid Is Controlled — interactive animation
- Levothyroxine vs NDT vs T3
- TPO and TgAb Antibodies
- Reverse T3 and Low T3 Syndrome
- Pregnancy and Hashimoto's
- Hashimoto, POTS & MCAS Overlap
- Thyroid Panel
- AIP and Gluten Elimination
- Selenium, Zinc, Iron & Iodine
- Hashimoto's Thyroiditis
- Thyroid Disorders
- Iodine
- Fatigue
- Brain Fog
- Graves' Disease
- Selenium
- POTS
- MCAS
- Gut-Thyroid Axis and Intestinal Permeability