Levothyroxine vs NDT vs Combination T4+T3 for Hashimoto's
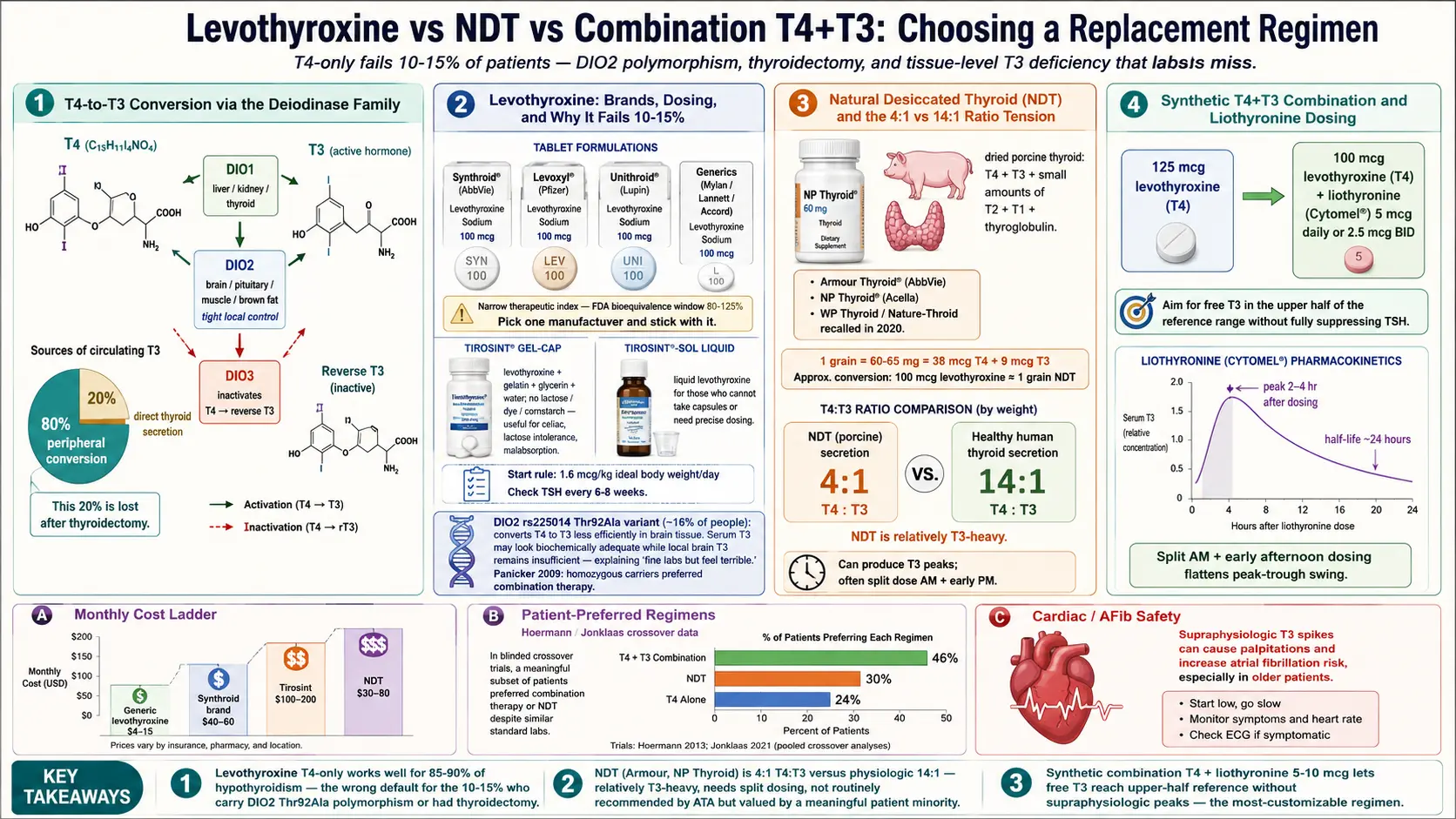
Table of Contents
- Levothyroxine — the T4-Only Standard
- Brand vs. Generic
- Tirosint — the Liquid-Gel Option
- Dosing and How to Take Levothyroxine
- Why T4-Only Fails Some Patients
- Natural Desiccated Thyroid (NDT)
- Converting From Levo to NDT
- The NDT Controversy
- Combination T4 + T3 (Synthetic)
- Liothyronine Dosing
- Slow-Release Compounded T3
- Evidence Review — What the Trials Show
- DIO2 Polymorphism Testing
- How to Advocate for a Trial
- Compounded T4+T3 Slow-Release
- Side Effects and Cardiac Safety
- Practical Tips for Any Regimen
- When to Reconsider Thyroid as the Problem
- Key Research Papers
- Connections
- Featured Videos
Levothyroxine — the T4-Only Standard
Levothyroxine is synthetic thyroxine (T4), identical in molecular structure to the T4 your thyroid gland would have produced on its own. It is sold in the United States under the brand names Synthroid, Levoxyl, Tirosint, and Unithroid, plus multiple generic versions made by companies like Mylan, Lannett, and Accord. Worldwide, it is one of the most commonly prescribed drugs on the planet — in the top five by U.S. prescription volume for more than a decade.
T4 itself is mostly a prohormone. The biologically active thyroid hormone is T3 (triiodothyronine), which binds thyroid receptors inside cells and drives metabolic gene expression. Your body is expected to take the T4 you swallow, circulate it, and convert it to T3 as needed, tissue by tissue. The enzymes that perform that conversion are the deiodinases: DIO1 (mostly liver, kidney, thyroid), DIO2 (brain, pituitary, muscle, brown fat — the tissues that want tight local control), and DIO3, which inactivates thyroid hormone by converting T4 to reverse T3.
For roughly 85–90% of people with hypothyroidism, this T4-to-T3 conversion system works well. They take one tablet a day, their TSH normalizes, their symptoms resolve, and they never think about thyroid hormone metabolism again. Levothyroxine is cheap (generic costs $4–$10 per month with insurance, often under $15 cash at warehouse pharmacies), stable, and extensively studied. It is the correct first-line treatment for Hashimoto's hypothyroidism, and the American Thyroid Association's 2014 and 2021 guidelines both reaffirm that position.
Brand vs. Generic
Levothyroxine has a narrow therapeutic index — the dose that works and the dose that causes symptoms are close together. Patients sometimes report that switching between Synthroid, a generic, and a different generic leaves them feeling off even when their TSH looks similar on paper.
The FDA allows generic levothyroxine to be between 80% and 125% of the labeled dose (the bioequivalence window for most drugs). For a narrow-therapeutic-index hormone, that range is wide enough to matter. A 100 mcg tablet from manufacturer A containing 95 mcg of actual drug, followed by a 100 mcg tablet from manufacturer B containing 112 mcg, is technically legal but biologically a 17% dose change.
The practical takeaway is simple: pick one manufacturer and stick with it. If your pharmacy switches generics because of supply, re-test TSH in six weeks. If you notice symptoms after a refill, check the manufacturer name (on the bottle label) against the last refill. Some endocrinologists write "dispense as written" or "brand necessary" on Synthroid prescriptions specifically to prevent substitution. Insurance may or may not honor this — expect to pay $40–$60 per month out of pocket for brand-name Synthroid if your plan refuses it.
Tirosint — the Liquid-Gel Option
Tirosint is a levothyroxine gel capsule containing just four ingredients: levothyroxine, gelatin, glycerin, and water. No lactose, no dyes, no cornstarch, no talc, no acacia. For patients with celiac disease, lactose intolerance, dye allergies, or significant malabsorption (post-bariatric surgery, atrophic gastritis, long-term PPI use), Tirosint often works when tablets do not.
It is also available as Tirosint-SOL, a liquid solution in single-dose ampoules, useful for patients who cannot swallow pills or need doses between standard tablet strengths. The downside is cost: Tirosint typically runs $100–$200 per month with insurance and significantly more cash. Manufacturer copay cards sometimes reduce the price to $25–$50. For most patients a standard tablet is fine; Tirosint is a targeted tool for a specific subset.
Dosing and How to Take Levothyroxine
The rough starting dose for full replacement (e.g., after thyroidectomy or in long-standing Hashimoto's with near-zero gland function) is 1.6 mcg per kilogram of ideal body weight per day. A 70 kg adult with ideal body weight close to that number starts around 112 mcg. In older adults, patients with cardiac disease, or anyone with subclinical hypothyroidism, a lower starting dose of 25–50 mcg is safer, titrated upward.
Re-check TSH (and ideally free T4 and free T3) every 6 to 8 weeks after a dose change. Earlier testing catches only transient shifts; the steady-state TSH lags the dose change by about six weeks.
Timing matters more than people realize. Levothyroxine is best absorbed on an empty stomach. The standard advice:
- Take it 30 to 60 minutes before food or coffee in the morning, with plain water.
- Or take it at bedtime, at least three hours after your last meal. Bedtime dosing produces slightly higher and steadier T4 levels for some patients, and it is an option if morning fasting is impractical.
- Space it by at least four hours from calcium, iron, magnesium, multivitamins, antacids, sucralfate, cholestyramine, soy protein, high-fiber foods, and espresso.
- Proton-pump inhibitors (omeprazole, pantoprazole) reduce absorption by about 10–15% by raising gastric pH. If you must take a PPI, expect a slightly higher levothyroxine dose requirement.
Why T4-Only Fails Some Patients
Large patient surveys consistently find that 10–15% of levothyroxine-treated patients report ongoing symptoms — fatigue, weight gain they cannot shift, cognitive fog, mood changes, cold intolerance — despite a TSH that the lab calls normal. This is not trivial. Ten percent of millions of prescriptions is a very large group of people who have been told "your labs are fine" while still feeling ill.
Two mechanisms are plausible and partially documented:
DIO2 polymorphism (rs225014, also called Thr92Ala). A common variant in the DIO2 gene produces a deiodinase enzyme that converts T4 to T3 less efficiently, especially in tissues like the brain. About 16% of people carry at least one copy. Carriers on T4-only therapy may have biochemically adequate serum T3 but locally insufficient brain T3, which would explain the subjective fog and low mood that lab numbers do not capture. Panicker and colleagues reported in 2009 that homozygous carriers showed significantly better psychological well-being on combination T4+T3 than on T4 alone.
Thyroidectomy effect. A healthy thyroid secretes both T4 and a small amount of T3 directly. When the gland is surgically removed (for cancer, nodules, or Graves), the direct-T3 source is gone, and the patient must make all their T3 from peripheral conversion. Thyroidectomized patients are disproportionately represented in the "still symptomatic on levo" group, and serum T3 tends to run in the low-normal range on T4-only therapy even when TSH is suppressed.
There are other hypotheses — chronic inflammation and elevated reverse T3, low ferritin, cortisol dysregulation, undiagnosed sleep apnea — and they matter too. But DIO2 variation and thyroidectomy are the two biologically cleanest reasons why T4-only does not work for everyone.
Natural Desiccated Thyroid (NDT)
NDT is dried, powdered pig thyroid gland compressed into tablets. It contains both T4 and T3, plus small amounts of T2, T1, and thyroglobulin. It predates synthetic levothyroxine by about 80 years — it was the standard hypothyroid treatment from the 1890s until the 1960s, when levothyroxine displaced it.
Current U.S. brands include Armour Thyroid (AbbVie) and NP Thyroid (Acella). WP Thyroid and Nature-Throid (RLC Labs) were recalled in 2020 for sub-potency issues and have not returned reliably to the market. ERFA Thyroid is available in Canada and by limited import. Dosing is measured in grains: 1 grain = 60 or 65 mg depending on manufacturer, delivering about 38 mcg T4 and 9 mcg T3 per grain.
The ratio is the key feature. NDT is roughly 4:1 T4 to T3 by weight, whereas a healthy human thyroid secretes closer to 14:1. In other words, NDT is relatively T3-heavy. This is a double-edged feature: patients who feel better on NDT usually credit the extra T3, but the same T3 load can produce transient peaks that cause palpitations or anxiety, particularly if a full daily dose is taken at once.
Converting From Levo to NDT
A standard equivalence used clinically: 100 mcg levothyroxine is approximately equal to 1 grain (60–65 mg) of NDT. This is only approximate; the T3 component in NDT is biologically more potent than its weight suggests, so many patients end up on a slightly lower "equivalent" NDT dose than the math predicts.
A reasonable conversion protocol:
- Start with the approximate equivalence (e.g., 125 mcg levo → about 1.25 grains NDT).
- Split the dose — half in the morning, half early afternoon — to blunt the T3 peak.
- Re-test TSH, free T4, and free T3 at 4–6 weeks. Expect TSH to run lower on NDT than on levo at equivalent symptomatic doses because circulating T3 suppresses TSH more strongly.
- Titrate by quarter-grain (about 15 mg) increments every 4–6 weeks based on symptoms and labs.
The NDT Controversy
Mainstream endocrinology is skeptical of NDT for reasonable reasons: the T4:T3 ratio is not physiologic, batch-to-batch potency has historically varied, and head-to-head randomized controlled trials have been mixed. The American Thyroid Association's 2014 guideline and the 2021 joint ATA/ETA/BTA consensus statement both state that NDT is not routinely recommended.
Yet patient-preference data tell a different story. Hoermann and colleagues in Europe and Jonklaas and colleagues in the U.S. have run trials asking patients who had been on stable T4 monotherapy to blindly compare T4 alone, T4+T3 combination, and NDT. In several of these studies, a significant minority of patients preferred NDT or combination therapy despite no difference in standard biochemical markers. A 2013 Hoermann-group analysis and a 2018 Jonklaas follow-up both concluded that patient-reported outcomes sometimes diverge from lab-based outcomes.
The fair summary: NDT is not magic, it is not dangerous in properly titrated doses, and for a subset of patients it produces better subjective function than T4 alone. It deserves a place in the toolkit, especially after a T4-only trial has been given a fair run.
Combination T4 + T3 (Synthetic)
An alternative to NDT is to combine standard levothyroxine with synthetic T3 (liothyronine, sold as Cytomel or generic). This lets the clinician pick any T4:T3 ratio rather than being locked into NDT's 4:1.
A common starting approach for a patient on, say, 125 mcg levothyroxine who still has symptoms:
- Reduce levothyroxine by about 12.5–25 mcg.
- Add liothyronine 5 mcg once daily (or 2.5 mcg twice daily).
- Re-test at 6 weeks; aim for free T3 in the upper half of the reference range without TSH fully suppressed.
Some endocrinologists target a T4:T3 ratio closer to physiologic (around 13:1 to 16:1), which is more conservative than NDT's 4:1. Others aim higher T3 based on symptoms.
Liothyronine Dosing
Synthetic T3 (liothyronine) has a short half-life of roughly 24 hours, with peak levels about 2–4 hours after dosing. This produces a daily peak-and-trough pattern that some patients tolerate fine and others find destabilizing.
Practical points:
- Start low: 5 mcg once daily in the morning.
- Titrate slowly: increase by 2.5–5 mcg every 2–4 weeks as tolerated.
- Many patients do better on split dosing — morning and early afternoon — to flatten the peak-trough swing.
- Avoid evening T3 doses if sleep becomes fragmented.
- Monitor free T3 both in the morning (pre-dose trough) and 2–4 hours after the morning dose (peak) if symptoms of overdose appear.
Slow-Release Compounded T3
Compounding pharmacies can prepare sustained-release liothyronine capsules, designed to deliver T3 gradually over 8–12 hours and permit once-daily dosing without the sharp peak. This is popular with integrative and functional-medicine prescribers.
Limitations to know about:
- Compounded preparations are not FDA-approved; potency depends entirely on the pharmacy's quality control.
- The "slow release" effect is real but variable — some preparations release faster than labeled.
- Cost runs $30–$80 per month; rarely covered by insurance.
- Use a compounding pharmacy accredited by the Pharmacy Compounding Accreditation Board (PCAB). Ask about third-party potency testing of finished product.
Evidence Review — What the Trials Show
After two dozen randomized trials over three decades, the honest summary:
- Standard biochemical outcomes (TSH, fT4, fT3) are achievable on T4 alone for most patients.
- When trials use only serum markers as the endpoint, combination therapy rarely beats T4 alone.
- When trials measure patient-reported outcomes — fatigue, mood, cognitive function, quality-of-life scores — a subset of patients (roughly 20–40% of those enrolled) prefer combination therapy, and that preference is sometimes statistically significant.
- A 2021 Jonklaas-led systematic review and a 2021 Akirov et al. meta-analysis both concluded that combination therapy offers modest benefit in a subset of patients and that better trials stratifying by DIO2 genotype and thyroidectomy status are needed.
- No trial to date has demonstrated harm from properly titrated combination therapy in non-elderly, non-cardiac patients.
The mismatch between biochemistry and lived experience is the entire story. If you measure only blood, combination therapy looks unnecessary. If you measure how people feel, a meaningful minority benefit.
DIO2 Polymorphism Testing
The DIO2 rs225014 variant (Thr92Ala) is not part of any standard clinical lab panel, but it sits in the raw data of every consumer genetic test. If you have 23andMe or AncestryDNA results, you can:
- Download your raw data from the company's website (account settings → download raw data).
- Upload it to a free interpretation tool like Promethease, SelfDecode, or Genetic Lifehacks, or search the raw-data file directly for "rs225014."
- Read your genotype: T/T (reference, efficient conversion), T/C (heterozygous carrier), C/C (homozygous, slower conversion — the clinically interesting group).
About 16% of people carry at least one C allele. Testing is worth doing if you are symptomatic on T4-only therapy; it is not worth doing preemptively, because a positive result does not predict that you will feel better on combination therapy — it only shifts the odds. A homozygous C/C result is a reasonable piece of evidence to bring to an endocrinologist when requesting a combination trial.
How to Advocate for a Trial
Most U.S. endocrinologists will prescribe T4 monotherapy readily and become visibly reluctant when asked about T3 or NDT. Getting a fair trial requires preparation.
Document persistent symptoms. Keep a written log for 4–8 weeks: daily energy, cognitive function, mood, weight, body temperature on waking, sleep quality. Bring the log to the appointment. Subjective complaints dismissed verbally carry more weight when you hand over a dated record.
Know your numbers. Bring recent TSH, free T4, free T3, and reverse T3 values. If free T3 sits in the bottom quartile of the reference range on T4-only therapy, that is a legitimate pharmacologic reason to consider adding T3.
Use the right language. Try: "I'd like a 12-week trial of combination T4+T3 therapy. I've done a lot of reading on the Jonklaas and Hoermann studies and I understand it may not help, but given my persistent symptoms and free T3 in the low-normal range, I think it's worth testing. Can we reduce my levothyroxine by 25 mcg and add liothyronine 5 mcg daily?" A concrete, time-limited request is harder to refuse than an open-ended complaint.
Find a willing clinician if yours refuses. Options include functional or integrative medicine MDs, osteopathic physicians (DOs) with endocrine interest, and some naturopathic doctors (licensed in many but not all states). A direct-primary-care clinician often has more flexibility than an insurance-contracted endocrinologist. Expect to pay out of pocket: $150–$400 for an initial consult, $75–$200 for follow-ups. The liothyronine or NDT prescription itself is usually covered by insurance even if the visit is not.
Compounded T4+T3 Slow-Release
Compounding pharmacies can also make combined T4+T3 capsules at any ratio, with T3 formulated for sustained release. This eliminates the two-pill regimen and flattens the T3 peak in one step. A typical compounded capsule might contain 100 mcg T4 plus 7.5 mcg sustained-release T3, taken once in the morning.
Cost is similar to compounded T3 alone ($40–$90 per month). The same caveats apply: pick a PCAB-accredited pharmacy, ask about potency testing, and keep the formulation consistent once you find one that works. Switching compounding pharmacies mid-therapy resets the clock.
Side Effects and Cardiac Safety
Any T3-containing regimen can push you into mild hyperthyroidism faster than pure T4 therapy. Watch for:
- Resting heart rate rising more than 10 beats per minute above baseline.
- Palpitations, especially in the afternoon 3–4 hours after a T3 dose.
- Fine tremor in the outstretched hands.
- New or worsened anxiety, jitteriness, insomnia.
- Unintentional weight loss beyond what you intended.
- Heat intolerance and excess sweating.
In patients over 60 and anyone with coronary artery disease, atrial fibrillation history, or significant osteoporosis risk, T3 adds real cardiovascular and skeletal risk. A baseline ECG is reasonable before starting. Bone density monitoring every two years is reasonable on long-term T3.
Pregnancy. The placenta actively metabolizes T3 and preferentially delivers T4 to the fetus, whose own thyroid produces T4 in the second and third trimesters. Current guidelines recommend tapering T3 off and converting to pure T4 before conception or at the first positive pregnancy test. Dose requirements rise by roughly 25–30% during pregnancy; increase levothyroxine proactively and re-test TSH every 4 weeks. See the pregnancy and Hashimoto's article for the full protocol.
Practical Tips for Any Regimen
- Consistent timing. Pick a time (morning fasting, or bedtime three hours post-meal) and hold to it. Day-to-day variation in timing creates day-to-day variation in absorption.
- Empty stomach. Coffee, milk, calcium, iron, and fiber all reduce absorption. Space by at least four hours.
- One manufacturer. Whether on levo, NDT, or combo, keep the same manufacturer across refills.
- Storage. Keep thyroid medication in its original container, away from heat, humidity, and direct light. Bathroom medicine cabinets are a bad choice; a bedroom drawer is fine.
- Track, don't guess. A simple spreadsheet of date, dose, TSH, fT4, fT3 at every blood draw reveals trends that a single abnormal value does not.
- Re-test at 6–8 weeks after any change — new dose, new manufacturer, new brand, added or removed T3.
When to Reconsider Thyroid as the Problem
If you have optimized TSH to 1–2, pushed free T4 into the upper half of the range, raised free T3 into the upper half as well — and still feel unwell — the thyroid regimen is probably not the limiting factor. Other causes worth investigating:
- Iron deficiency. Serum ferritin under 70 ng/mL is a common and underdiagnosed driver of fatigue even when hemoglobin is normal. See the selenium, zinc, iron, iodine article.
- Vitamin B12. Levels under 400 pg/mL can cause fatigue and cognitive symptoms that mimic hypothyroidism.
- Adrenal dysregulation and chronic stress. Cortisol-driven fatigue is not fixed by thyroid hormone.
- Sleep apnea. Surprisingly common in Hashimoto's patients, particularly those who have gained weight; a home sleep study is low-friction and often diagnostic.
- Perimenopause. Overlapping fatigue, brain fog, and weight changes. Hormone assessment is worthwhile in women 40 and up.
- POTS, MCAS, dysautonomia. Overlap with Hashimoto's is well documented. See the POTS/MCAS overlap article.
- Depression. A separate condition with real overlap, worth assessing and treating in its own right.
Thyroid hormone is powerful but not a panacea. When the numbers are right and the symptoms remain, look elsewhere before stacking more thyroid medication on top.
Key Research Papers
Foundational and recent peer-reviewed publications on monotherapy levothyroxine, T4+T3 combination therapy, desiccated thyroid extract, the DIO2 polymorphism, and the patient-reported quality-of-life literature. Each citation links to the full text via DOI.
- Jonklaas J, Bianco AC, Bauer AJ, et al. Guidelines for the Treatment of Hypothyroidism (American Thyroid Association). Thyroid. 2014;24(12):1670–1751.
- Bunevicius R, Kazanavicius G, Zalinkevicius R, Prange AJ Jr. Effects of Thyroxine as Compared with Thyroxine plus Triiodothyronine in Patients with Hypothyroidism. New England Journal of Medicine. 1999;340(6):424–429.
- Hoang TD, Olsen CH, Mai VQ, Clyde PW, Shakir MK. Desiccated Thyroid Extract Compared with Levothyroxine in the Treatment of Hypothyroidism: A Randomized, Double-Blind, Crossover Study. Journal of Clinical Endocrinology & Metabolism. 2013;98(5):1982–1990.
- Wiersinga WM, Duntas L, Fadeyev V, Nygaard B, Vanderpump MPJ. 2012 ETA Guidelines: The Use of L-T4 + L-T3 in the Treatment of Hypothyroidism. European Thyroid Journal. 2012;1(2):55–71.
- Panicker V, Saravanan P, Vaidya B, et al. Common Variation in the DIO2 Gene Predicts Baseline Psychological Well-Being and Response to Combination Thyroxine plus Triiodothyronine Therapy in Hypothyroid Patients. Journal of Clinical Endocrinology & Metabolism. 2009;94(5):1623–1629.
- Saravanan P, Chau WF, Roberts N, Vedhara K, Greenwood R, Dayan CM. Psychological Well-Being in Patients on "Adequate" Doses of L-Thyroxine: Results of a Large, Controlled Community-Based Questionnaire Study. Clinical Endocrinology. 2002;57(5):577–585.
- Hoermann R, Midgley JEM, Larisch R, Dietrich JW. Recent Advances in Thyroid Hormone Regulation: Toward a New Paradigm for Optimal Diagnosis and Treatment. Frontiers in Endocrinology. 2017;8:364.
- Peterson SJ, Cappola AR, Castro MR, et al. An Online Survey of Hypothyroid Patients Demonstrates Prominent Dissatisfaction. Thyroid. 2018;28(6):707–721.
- Wartofsky L, Dickey RA. The Evidence for a Narrower Thyrotropin Reference Range Is Compelling. Journal of Clinical Endocrinology & Metabolism. 2005;90(9):5483–5488.
- Surks MI, Goswami G, Daniels GH. The Thyrotropin Reference Range Should Remain Unchanged. Journal of Clinical Endocrinology & Metabolism. 2005;90(9):5489–5496.
- Centanni M, Gargano L, Canettieri G, et al. Thyroxine in Goiter, Helicobacter pylori Infection, and Chronic Gastritis. New England Journal of Medicine. 2006;354(17):1787–1795.
- Caturegli P, De Remigis A, Rose NR. Hashimoto Thyroiditis: Clinical and Diagnostic Criteria. Autoimmunity Reviews. 2014;13(4-5):391–397.
Live PubMed Searches
Live PubMed queries that update as new papers are indexed.
- PubMed: DIO2 polymorphism + thyroid
- PubMed: T4 + T3 combination therapy
- PubMed: natural desiccated thyroid
- PubMed: levothyroxine bioequivalence
- PubMed: liothyronine (Cytomel)
- PubMed: post-thyroidectomy T3
- PubMed: levothyroxine absorption + drug interactions
- PubMed: patient-reported outcomes
Connections
- How Your Thyroid Is Controlled — interactive animation
- Hashimoto's Thyroiditis Overview
- Pregnancy and Hashimoto's
- Selenium, Zinc, Iron, and Iodine
- TSH, T4, and T3 Optimal Ranges
- AIP and Gluten Elimination
- TPO and TgAb Antibodies
- Reverse T3 and Low T3 Syndrome
- Hashimoto, POTS, and MCAS Overlap
- Gut-Thyroid Axis and Intestinal Permeability
- Thyroid Disorders
- Selenium
- Iron
- Zinc
- Iodine
- Magnesium
- Celiac Disease
- Fatigue
- Thyroid Panel