Hashimoto's, POTS & MCAS Overlap
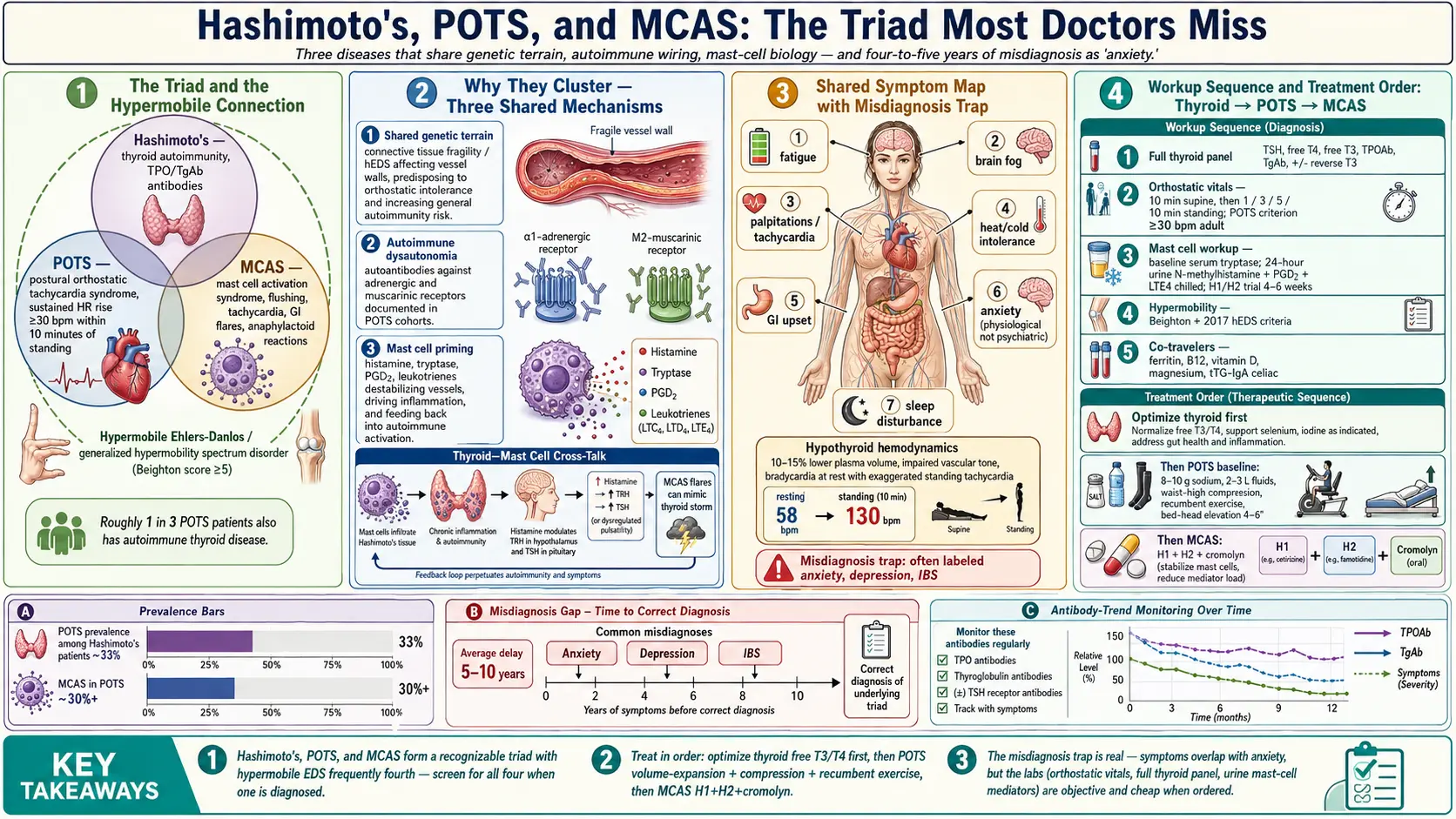
Table of Contents
- Why These Three Cluster Together
- Shared Symptoms That Cause Misdiagnosis
- How Hypothyroidism Mimics and Worsens POTS
- Mast Cells, Histamine, and Thyroid Autoimmunity
- Workup Sequence — What to Ask For and In What Order
- Treatment Ordering — Thyroid First, Then POTS, Then MCAS
- Gluten, Histamine, and Iodine — Dietary Landmines
- Practical Self-Monitoring
- When to Push Back on Your Doctor
- Key Research Papers
- Connections
- Featured Videos
Why These Three Cluster Together
If you are a woman in your twenties or thirties, you have been told your labs are "basically normal," and you still feel like your body is falling apart — exhausted, dizzy when you stand up, flushing at random, brain fog you cannot think through — there is a good chance you are not dealing with one disease. You are dealing with three.
Hashimoto's thyroiditis, postural orthostatic tachycardia syndrome (POTS), and mast cell activation syndrome (MCAS) form a recognizable triad. The fourth member that often travels with them is hypermobile Ehlers-Danlos syndrome (hEDS) or generalized hypermobility spectrum disorder. Clinicians who see this overlap regularly — Afrin, Blitshteyn, Shaw, Seneviratne — report that roughly one in three POTS patients also has an autoimmune thyroid condition, and a majority of hEDS patients will eventually meet criteria for at least two of the four.
Why do they travel together? Three mechanisms tie them:
- Shared genetic terrain. Connective tissue fragility (hEDS) affects blood vessel walls, which predisposes to orthostatic intolerance. The same patients show higher rates of autoimmunity in general, and thyroid autoimmunity in particular.
- Autoimmune dysautonomia. Autoantibodies against adrenergic and muscarinic receptors have been documented in POTS cohorts. The immune system that attacks thyroid peroxidase is the same immune system that can produce these receptor antibodies.
- Mast cell priming. Mast cells release histamine, tryptase, prostaglandins, and dozens of other mediators that destabilize blood vessels, drive inflammation, and feed back into autoimmune activation. A chronically primed mast cell compartment makes every other system noisier.
The practical takeaway: if you have been diagnosed with one of these three, actively screen for the other two. Treating Hashimoto's alone will not fix the dizziness. Treating POTS alone will not fix the flushing. You need the full picture before you can rank the fires.
Shared Symptoms That Cause Misdiagnosis
The reason this triad gets missed for years is that the symptoms overlap almost completely. A patient walks into a primary care office and says: "I'm tired, my heart races, I can't think, I get hot and cold for no reason, and I feel like I'm allergic to everything." The doctor orders a TSH, sees it sitting at 3.8, says "your thyroid is fine," and sends you home with a referral to a therapist.
Here is the overlap map — the symptoms shared by at least two of the three conditions:
- Fatigue — core feature of all three. Hypothyroid fatigue is heavy and cold. POTS fatigue is a post-exertional crash after standing or doing chores. MCAS fatigue often follows a flare, meals, or exposures.
- Brain fog. Hashimoto's slows cognition globally. POTS brain fog spikes when upright (cerebral hypoperfusion). MCAS brain fog tracks with histamine release.
- Palpitations and tachycardia. Thyroid autoimmunity can produce a transient thyrotoxic phase (Hashitoxicosis). POTS is defined by a sustained heart-rate rise of 30+ bpm on standing. MCAS flares release adrenaline-like mediators that speed the heart.
- Heat and cold intolerance. Hypothyroid patients are cold; thyrotoxic ones are hot. POTS blunts the autonomic response to temperature. MCAS flushes and sweats unpredictably.
- GI upset. Constipation (hypothyroid), gastroparesis (POTS), diarrhea and cramping (MCAS).
- Anxiety. All three produce genuine physiological anxiety that is indistinguishable from psychiatric anxiety without a workup.
- Sleep disturbance. Night sweats, middle-of-the-night adrenaline surges, non-restorative sleep.
The emotional cost of this overlap is its own problem. Many patients spend five to ten years being told they have anxiety, depression, or "it's stress." The symptoms are real. The labs just have not been ordered yet.
How Hypothyroidism Mimics and Worsens POTS
Thyroid hormone regulates blood volume, vascular tone, and the sensitivity of your heart to adrenaline. When thyroid hormone is low — or when your labs look normal but the tissue level is actually low — every one of these systems becomes unstable.
The mechanisms:
- Reduced blood volume. Hypothyroid patients run 10–15% lower plasma volume than euthyroid controls. POTS is, at its core, a low-blood-volume illness made worse by pooling. Adding hypothyroidism takes an already under-filled circulation and drains it further.
- Impaired vascular tone. Thyroid hormone supports endothelial function and vasoconstriction in the legs. When it drops, blood pools harder when you stand.
- Bradycardia at rest, exaggerated tachycardia on standing. A hypothyroid heart beats slowly when you are horizontal but overshoots when adrenaline takes over in the upright position. This is why patients with untreated Hashimoto's often have a resting pulse of 58 and a standing pulse of 130.
- Cold extremities and Raynaud-like symptoms. Peripheral vasoconstriction conserves heat in hypothyroidism, but it also worsens the hands-and-feet-freezing complaint typical of POTS.
This is why the first move in any suspected POTS patient is to nail down the thyroid. Not with a single TSH — which can be in range while free T3 is in the basement — but with a full panel (TSH, free T4, free T3, TPO antibodies, thyroglobulin antibodies, and often reverse T3). See TSH/T4/T3 optimal ranges and Reverse T3 and low-T3 syndrome for the interpretation details.
Mast Cells, Histamine, and Thyroid Autoimmunity
Mast cells are tissue-resident immune cells stationed in skin, gut, airways, and — importantly — the thyroid gland. When they degranulate, they release histamine, tryptase, prostaglandin D2, leukotrienes, heparin, and dozens of cytokines.
Why this matters for Hashimoto's:
- Mast cells infiltrate autoimmune thyroid tissue. Histological studies of Hashimoto's glands consistently show increased mast cell density around the lymphocytic infiltrate.
- Histamine and thyroid function. Histamine affects TRH and TSH release at the hypothalamic-pituitary level. A chronically activated mast cell system feeds into the loop that controls thyroid output.
- MCAS flares mimic thyroid storm. A severe mast cell flare can produce tachycardia, flushing, hypertension, anxiety, tremor, diarrhea, and a sense of impending doom — the same symptoms as a thyrotoxic crisis. ER workups often find normal thyroid labs and send the patient home with no explanation.
- Treatment for MCAS lowers autoimmune noise. Patients on H1/H2 blockers and cromolyn frequently report their Hashimoto's antibodies trend down over six to twelve months. This is anecdotal but consistent enough in clinical cohorts to be taken seriously.
The reverse is also true. Poorly controlled Hashimoto's — particularly during a Hashitoxic flare — can destabilize mast cells. The thyroid and the mast cell compartment talk to each other constantly. Treating only one of them leaves the other to stir the pot.
Workup Sequence — What to Ask For and In What Order
If you suspect this triad, here is the order of operations. You can often get most of it through a supportive primary care doctor; the harder pieces may need a rheumatologist, cardiologist, or allergist.
Step 1. Thyroid panel (done first)
- TSH, free T4, free T3
- TPO antibodies and thyroglobulin antibodies — see TPO and TgAb explained
- Reverse T3 if fatigue dominates and free T3 looks borderline
- Thyroid ultrasound if antibodies are positive — confirms the characteristic heterogeneous, hypoechoic pattern
Step 2. Orthostatic vitals (in-office, ten minutes)
- Lie flat for 10 minutes. Measure HR and BP.
- Stand up. Measure HR and BP at 1, 3, 5, and 10 minutes.
- POTS criterion: sustained HR rise of ≥30 bpm (≥40 bpm in teens) within 10 minutes of standing, without a drop in BP >20/10.
- If the in-office test is negative but symptoms persist, push for a tilt-table test with autonomic reflex screen.
Step 3. Mast cell workup
- Serum tryptase (baseline, when not flaring). Normal does not rule out MCAS; elevated points strongly toward it.
- 24-hour urine N-methylhistamine, prostaglandin D2 (or 11-beta-PGF2-alpha), and leukotriene E4. Collect chilled.
- Chromogranin A (off PPIs for 5 days before the test, which falsely elevates it).
- A clinical trial of H1 + H2 antihistamines for 4–6 weeks can be diagnostic if symptoms respond.
Step 4. Hypermobility screen
- Beighton score (0–9). Score ≥5 in adults suggests hypermobility.
- Family history of "double-jointedness," easy bruising, stretchy skin, or early joint problems.
- Full hEDS criteria (2017 international) require more than just Beighton — skin findings and musculoskeletal complications count.
Step 5. Co-travelers worth checking
- Ferritin (aim >50 ng/mL, ideally 70–100 for POTS)
- Vitamin B12, vitamin D, magnesium
- Celiac panel (tTG-IgA + total IgA) — celiac coexists with Hashimoto's at roughly 5–10%
- Cortisol (AM serum, or 4-point salivary) — HPA-axis dysregulation is common in the triad
Treatment Ordering — Thyroid First, Then POTS, Then MCAS
You cannot treat this triad in parallel without going in circles. The order matters, and the order is thyroid → POTS → MCAS.
1. Optimize the thyroid first
Get free T3 into the upper third of the reference range and free T4 into the mid-to-upper third. TSH in this population often needs to be below 2.0 for patients to feel well, though individual response varies. Some patients do fine on levothyroxine alone; others need a T4/T3 combination or natural desiccated thyroid (see levothyroxine vs NDT vs T3). Give it at least 8–12 weeks at a stable dose before judging.
Why first? Because a significant fraction of POTS-like symptoms resolve on their own once tissue thyroid levels come up. You do not want to be stacking three more drugs on a patient whose core problem is actually undertreated hypothyroidism.
2. Then address POTS with non-pharmacologic baseline
- Salt. 8–10 grams of sodium per day unless you have a reason not to. That is roughly 2–3 teaspoons.
- Fluids. 2–3 liters per day. Electrolyte drinks (LMNT, Liquid IV, or homemade) help.
- Compression. Waist-high 20–30 mmHg stockings or an abdominal binder. Knee-highs are mostly cosmetic.
- Recumbent exercise (Levine or CHOP protocol). Rowing, recumbent bike, swimming — start horizontal and graduate to upright over months.
- Sleep with the head of the bed elevated 4–6 inches to train renin-angiotensin regulation.
If the baseline is not enough, medications come next: beta-blockers (propranolol, metoprolol) for hyperadrenergic POTS, midodrine for vasoconstriction, fludrocortisone for volume, ivabradine if beta-blockade is not tolerated, pyridostigmine for some autoimmune phenotypes.
3. Then layer MCAS therapy
Start with the cheap, safe pieces and escalate:
- H1 antihistamines (daytime: cetirizine, fexofenadine, loratadine; night: hydroxyzine or diphenhydramine)
- H2 antihistamines (famotidine 20–40 mg twice daily)
- Mast cell stabilizers: cromolyn sodium 200 mg four times daily before meals, ketotifen 1–2 mg twice daily
- Quercetin 500–1000 mg twice daily, often paired with bromelain or luteolin
- Leukotriene blockers (montelukast) for respiratory-predominant flares
- Low-dose naltrexone (LDN) 1.5–4.5 mg at night — modulates both mast cells and autoimmune activity; increasingly used across the triad
Avoid any drug or supplement that is a known mast cell trigger — opioids (morphine, codeine), vancomycin, radiocontrast without premedication, NSAIDs in some patients, alcohol.
Gluten, Histamine, and Iodine — Dietary Landmines
Diet is not a cure for any of these three conditions, but it is a lever, and the triad makes the lever tricky because the rules for one disease sometimes clash with the rules for another.
Gluten
Hashimoto's and celiac share genetic background (HLA-DQ2/DQ8). Even in non-celiac patients, a strict gluten-free trial of 3–6 months lowers TPO antibodies in a sizable minority. The autoimmune protocol (AIP) is a more aggressive version. See AIP and gluten elimination. Gluten is not known to directly trigger mast cells or POTS, but the inflammation it drives in susceptible people makes both worse.
Histamine
This is the real landmine for MCAS patients. High-histamine foods: aged cheeses, cured meats, fermented foods (sauerkraut, kimchi, kombucha), wine and beer, leftovers stored more than 24 hours, tomatoes, spinach, eggplant, avocado, banana, strawberries, chocolate, vinegar. The problem is that several of these — fermented foods especially — are darlings of the "gut health for Hashimoto's" crowd. A patient with both conditions should try a low-histamine diet for 4–8 weeks and reintroduce systematically. See the dedicated low-histamine diet guide.
Iodine
This is where well-meaning advice goes wrong most often. High-dose iodine (kelp tablets, Lugol's solution, 12.5 mg daily protocols) can accelerate Hashimoto's autoimmune activity. Studies from iodine-replete populations show that excess iodine increases TPO antibodies and hastens the transition to overt hypothyroidism. Patients with Hashimoto's should aim for roughly the RDA (150 mcg/day from food and a standard multivitamin) — not megadose supplementation. See selenium, zinc, iron, and iodine for the full nuance.
Salt
POTS wants 8–10 grams daily. MCAS usually tolerates this fine. Hashimoto's does not care. This is one of the easier wins.
Practical Self-Monitoring
You will be your own most reliable data source between appointments. A cheap wrist BP cuff and a smartphone are enough.
- Daily orthostatic vitals (first 4–6 weeks, then weekly). Supine HR/BP after 5 minutes flat in the morning. Stand, then measure at 1, 3, 5, and 10 minutes. Log it in a spreadsheet or an app like Welltory or Visible.
- Resting heart rate trend. A smartwatch that logs overnight HR shows the thyroid and autonomic picture more reliably than a single clinic reading. A trend from 75 down to 58 often means thyroid is undertreated. A trend up from 65 to 88 often means you are flaring or thyroid is swinging.
- Symptom-and-trigger diary. Date, food, environment, menstrual cycle day, symptoms, severity 1–10. Three weeks of this usually reveals a pattern no doctor can extract in a 15-minute visit.
- Basal body temperature first thing in the morning. Chronically below 97.4°F (36.3°C) suggests under-treated hypothyroidism.
- Flare journal. When you have a bad day, write down what you ate, did, wore, and took in the preceding 24 hours. Patterns emerge: a specific detergent, a skipped dose, a high-histamine dinner, a hot shower, a missed salt load.
When to Push Back on Your Doctor
This triad has a diagnostic delay averaging 5–10 years in women. The reason is almost always that individual specialists look only at their own organ. You may need to advocate hard. Red flags for a workup that is not thorough enough:
- TSH alone ordered with no antibodies or free T3/T4.
- "Your labs are normal, it's just anxiety" without orthostatic vitals ever being measured.
- Being told MCAS is not real. It is real; it is in the ICD-10 as D89.42.
- A refusal to trial H1/H2 antihistamines for 4 weeks. These are cheap, over-the-counter, and virtually risk-free.
- No recognition that hypermobility is clinically significant.
If your current provider is not engaged, look for a dysautonomia specialist, an allergist/immunologist who sees MCAS, or an integrative/functional medicine physician who understands the triad. Dysautonomia International maintains a physician directory. You are not a difficult patient — you have a complex illness, and it takes the right team.
Key Research Papers
Foundational and recent peer-reviewed publications on the Hashimoto's / POTS / MCAS triad — autoimmune thyroid disease, postural tachycardia, mast-cell activation, and the connective-tissue overlap. Each citation links to the full text via DOI.
- Caturegli P, De Remigis A, Rose NR. Hashimoto Thyroiditis: Clinical and Diagnostic Criteria. Autoimmunity Reviews. 2014;13(4-5):391–397.
- Blitshteyn S. Autoimmune Markers and Autoimmune Disorders in Patients with Postural Tachycardia Syndrome (POTS). Lupus. 2015;24(13):1364–1369.
- Shaw BH, Stiles LE, Bourne K, et al. The Face of Postural Tachycardia Syndrome — Insights from a Large Cross-Sectional Online Community-Based Survey. Journal of Internal Medicine. 2019;286(4):438–448.
- Kohno R, Cannom DS, Olshansky B, et al. Mast Cell Activation Disorder and Postural Orthostatic Tachycardia Syndrome: A Clinical Association. Journal of the American Heart Association. 2021;10(17):e021002.
- Seneviratne SL, Maitland A, Afrin L. Mast Cell Disorders in Ehlers-Danlos Syndrome. American Journal of Medical Genetics Part C: Seminars in Medical Genetics. 2017;175(1):226–236.
- Afrin LB, Self S, Menk J, Lazarchick J. Characterization of Mast Cell Activation Syndrome. American Journal of the Medical Sciences. 2017;354(2):207–215.
- Theoharides TC, Tsilioni I, Ren H. Recent Advances in Our Understanding of Mast Cell Activation — or Should It Be Mast Cell Mediator Disorders? Expert Review of Clinical Immunology. 2019;15(6):639–656.
- Vernino S, Stiles LE. Autoimmunity in Postural Orthostatic Tachycardia Syndrome: Current Understanding. Autonomic Neuroscience. 2018;215:78–82.
- Watari M, Nakane S, Mukaino A, et al. Autoimmune Postural Orthostatic Tachycardia Syndrome. Annals of Clinical and Translational Neurology. 2018;5(4):486–492.
- Hollowell JG, Staehling NW, Flanders WD, et al. Serum TSH, T4, and Thyroid Antibodies in the United States Population (NHANES III). Journal of Clinical Endocrinology & Metabolism. 2002;87(2):489–499.
- Jonklaas J, Bianco AC, Bauer AJ, et al. Guidelines for the Treatment of Hypothyroidism (American Thyroid Association). Thyroid. 2014;24(12):1670–1751.
- Knezevic J, Starchl C, Tmava Berisha A, Amrein K. Thyroid–Gut-Axis: How Does the Microbiota Influence Thyroid Function? Nutrients. 2020;12(6):1769.
Live PubMed Searches
Live PubMed queries that update as new papers are indexed.
- PubMed: Hashimoto's + POTS
- PubMed: POTS + mast cell activation
- PubMed: EDS + POTS + MCAS triad
- PubMed: autoimmune thyroid + dysautonomia
- PubMed: mast cells + thyroid autoimmunity
- PubMed: hypothyroidism + orthostatic intolerance
- PubMed: histamine intolerance + autoimmune
- PubMed: iodine + Hashimoto's antibody
Connections
- How Your Thyroid Is Controlled — interactive animation
- Hashimoto's Thyroiditis Overview
- AIP and Gluten Elimination
- Levothyroxine vs NDT vs T3
- TSH, T4, and T3 Optimal Ranges
- Selenium, Zinc, Iron, and Iodine
- TPO and TgAb Antibodies
- Reverse T3 and Low T3 Syndrome
- Pregnancy and Hashimoto's
- Gut-Thyroid Axis and Intestinal Permeability
- POTS
- MCAS
- Thyroid Disorders
- Low-Histamine Diet
- Brain Fog
- Iodine