Pregnancy and Hashimoto's Thyroiditis
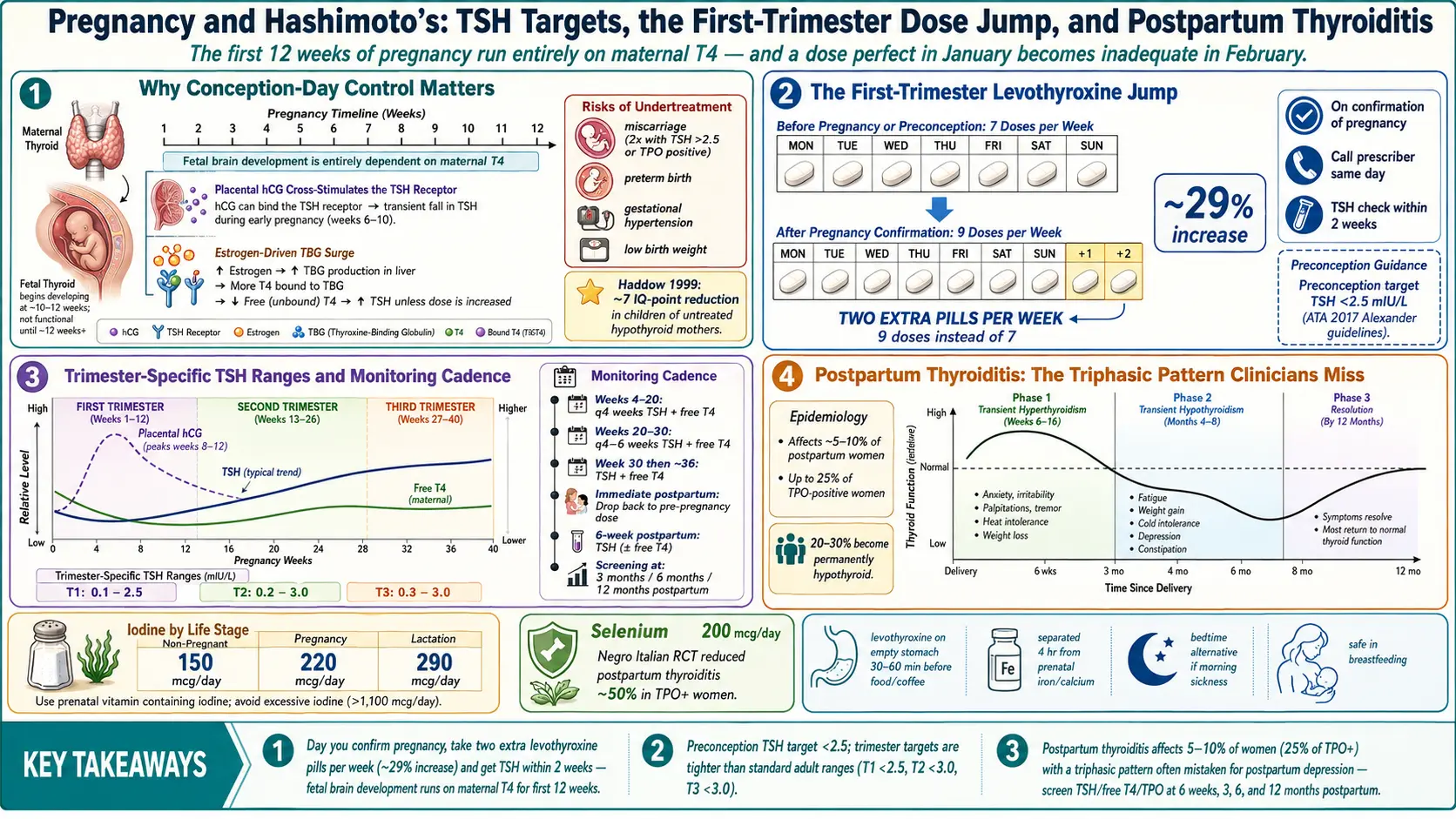
Table of Contents
- Why Hashimoto's Matters Before You Conceive
- The Preconception TSH Target: Under 2.5
- TPO Antibodies and Euthyroid Infertility
- The First-Trimester Levothyroxine Jump
- Trimester-Specific TSH Ranges
- Monitoring Cadence Through Pregnancy
- Postpartum Thyroiditis — The Missed Diagnosis
- Breastfeeding on Thyroid Medication
- Iodine and Selenium in Pregnancy
- Practical Tactics — Pills, Prenatals, Travel
- Advocating for Yourself at Appointments
- Key Research Papers
- Connections
- Featured Videos
Why Hashimoto's Matters Before You Conceive
If you have Hashimoto's thyroiditis and you are thinking about getting pregnant, the first thing to know is this: the single biggest variable that affects your pregnancy outcome is how well your thyroid is controlled at the moment of conception. Not in the second trimester. Not when you find out. At conception.
That is because the first ten to twelve weeks of pregnancy, the fetus cannot make any thyroid hormone of its own. Every molecule of T4 that builds the early fetal brain, skeleton, and placenta comes from you. If your thyroid is struggling — even in ways that feel mild or invisible — the fetus feels it too.
The risks of untreated or undertreated hypothyroidism in pregnancy are real and well documented:
- Miscarriage. Women with TSH above 2.5 mIU/L or positive TPO antibodies have roughly double the miscarriage rate of euthyroid, antibody-negative women.
- Preterm birth. Rates climb measurably when maternal TSH stays elevated, especially above 4.0 mIU/L.
- Gestational hypertension and preeclampsia. Undertreated hypothyroidism is an independent risk factor.
- Placental abruption and low birth weight. Both show up more often in inadequately treated pregnancies.
- Reduced child IQ. The 1999 Haddow study found children of untreated hypothyroid mothers scored roughly 7 IQ points lower at age seven than controls. That finding changed how obstetrics treats this disease.
None of this is said to frighten you. It is said because the fix is cheap, safe, and extraordinarily effective. A generic pill that costs pennies a day, titrated correctly, brings your risk profile back to that of a woman without thyroid disease. The catch is that "titrated correctly" requires more vigilance in pregnancy than at any other time in your life.
The Preconception TSH Target: Under 2.5
The American Thyroid Association's 2017 guidelines (Alexander et al.) recommend a preconception TSH of less than 2.5 mIU/L in women with known hypothyroidism who are trying to conceive. Some endocrinologists aim even lower — 1.0 to 2.0 — especially in women with a history of miscarriage or infertility.
Why this number matters: a "normal" lab range of roughly 0.5 to 4.5 mIU/L was never designed for pregnancy. It reflects the middle 95% of non-pregnant adults, including many with undiagnosed subclinical disease. In pregnancy, the normal range shifts downward because the placenta produces human chorionic gonadotropin (hCG), which cross-stimulates the TSH receptor and pushes your own TSH lower. A TSH of 3.8 before pregnancy may look reassuring on a generic report, but it signals a gland that will struggle to meet first-trimester demand.
If you are planning pregnancy and your TSH is between 2.5 and 4.5, ask your doctor about starting or increasing levothyroxine before conception rather than after. Waiting until a positive pregnancy test costs you four to six crucial weeks of fetal development.
TPO Antibodies and Euthyroid Infertility
A second, more subtle issue: you can have TPO or TgAb antibodies without being hypothyroid yet. Your TSH sits in the normal range, your free T4 looks fine, and a standard workup pronounces your thyroid healthy. But those antibodies are still associated with:
- Lower fertility rates, particularly in women over 35.
- Higher miscarriage rates, even when TSH stays below 2.5.
- Reduced response to IVF stimulation protocols.
- Higher risk of progressing to overt hypothyroidism during pregnancy, as the placenta's thyroid demands outstrip a weakened gland's reserve.
The Negro 2006 trial (JCEM) is the landmark study here. In euthyroid, TPO-positive pregnant women, a small dose of levothyroxine cut the miscarriage rate from 13.8% to 3.5% and the preterm-birth rate from 22.4% to 7.0%. Later trials (most notably TABLET in 2019) did not replicate this benefit in women with normal TSH at baseline, so the field is not unanimous. But if you have TPO antibodies, a history of recurrent miscarriage, or a TSH drifting upward quarter by quarter, it is entirely reasonable to ask your endocrinologist about preemptive treatment.
See the TPO and TgAb article for a deeper dive on what these antibodies mean and how they change over time.
The First-Trimester Levothyroxine Jump
Here is the single most important practical fact on this page: the moment you find out you are pregnant, your levothyroxine dose usually needs to go up by about 25–30%, and it needs to happen immediately.
The reason is a surge in thyroid-binding globulin (TBG) driven by rising estrogen. TBG is the taxi service that carries thyroid hormone through the bloodstream. When estrogen spikes, the liver makes more taxis, and more of your circulating T4 gets bound and becomes biologically unavailable. A gland that was comfortably meeting demand before pregnancy suddenly cannot keep up. Add the placenta's own hormonal appetite, and a dose that was perfect in January becomes inadequate in February.
The ATA-endorsed practical rule: on the day you confirm pregnancy, take two extra pills per week of your existing dose (that is, nine doses per week instead of seven). This is roughly a 29% increase and approximates what your endocrinologist would prescribe anyway. Then call your doctor's office the same day and ask for a TSH check within two weeks.
Do not wait for your first OB appointment at eight or ten weeks. Do not wait for a return call from a nurse triage line. The two-extra-pills-per-week move is safe, reversible, and supported by 2017 ATA guidelines — but call your prescribing doctor to confirm and document the change.
Trimester-Specific TSH Ranges
Pregnancy has its own reference intervals. The ATA recommends these upper limits:
- First trimester: 0.1 to 2.5 mIU/L (some labs use 0.1 to 4.0 if population-specific ranges are available).
- Second trimester: 0.2 to 3.0 mIU/L.
- Third trimester: 0.3 to 3.0 mIU/L (some guidelines extend to 3.5).
If your report comes back with a standard adult range noted (0.5 to 4.5 or similar) and your number is, say, 3.1 in the first trimester, the lab will flag it "normal" even though by pregnancy standards it is elevated. Read the actual number. Compare it to the trimester-specific target. Ask for a dose adjustment if you are above target — do not be talked out of a raise just because the lab printout shows no flag.
On the other end, a first-trimester TSH that drops to 0.05 or even becomes undetectable is usually not hyperthyroidism — it is the normal hCG-driven dip. Free T4 and clinical symptoms (rapid heart rate, tremor, heat intolerance) are better guides than TSH alone in early pregnancy.
Monitoring Cadence Through Pregnancy
For any pregnancy involving Hashimoto's or known hypothyroidism:
- Weeks 4–20 (first half): TSH and free T4 every four weeks. This is the window where requirements climb fastest and most dose adjustments happen.
- Weeks 20–30: TSH and free T4 every four to six weeks. Dose needs usually plateau.
- Weeks 30–delivery: at least once more around week 30. Some OBs check again near 36 weeks.
- Immediately postpartum: drop your dose back to your pre-pregnancy level the day after delivery. Check TSH at six weeks postpartum.
- 6 weeks, 3 months, 6 months, 12 months postpartum: screen for postpartum thyroiditis (see below). Many endocrinologists miss this.
If your OB or endocrinologist is checking less often than this, advocate. Four-weekly labs in the first half of pregnancy is the guideline standard, not overkill.
Postpartum Thyroiditis — The Missed Diagnosis
This is the chapter of the Hashimoto's story that most new mothers never hear about. Roughly 5 to 10% of all postpartum women — and up to 25% of those with pre-existing TPO antibodies — develop postpartum thyroiditis in the year after delivery.
The classic pattern is three phases:
- Transient hyperthyroidism (weeks 6 to 16 postpartum). The inflamed gland leaks stored hormone. You feel anxious, wired, heat-intolerant. Heart pounds. You lose weight you had not expected to lose. It is often blamed on new-parent stress or postpartum anxiety.
- Transient hypothyroidism (months 4 to 8 postpartum). Hormone stores deplete. Exhaustion, cold intolerance, constipation, weight gain, brain fog, hair falling out in the shower, low milk supply, mood flattening into what looks exactly like postpartum depression — because the symptoms are identical.
- Resolution (by 12 months postpartum in most women). Thyroid function returns to baseline.
Not every woman moves through all three phases. Some only get the hyper phase. Some only get the hypo phase. Some stay hypothyroid permanently — an estimated 20 to 30% of women who have postpartum thyroiditis remain hypothyroid long-term or relapse into overt Hashimoto's within five years.
The practical rule: any postpartum fatigue, mood change, hair loss, or milk-supply problem that does not resolve within a few weeks deserves a TSH, free T4, and TPO antibody check. "Probably just new-mom exhaustion" is not an acceptable answer without labs. If your provider resists, ask for the draw in writing.
Breastfeeding on Thyroid Medication
Levothyroxine is entirely safe in breastfeeding. The amount that crosses into breast milk is vanishingly small — smaller than the variation a nursing infant experiences from their own developing thyroid. You do not need to pump-and-dump, time feeds around doses, or worry about infant exposure.
The same is true for desiccated thyroid extracts (NDT) and liothyronine (T3), though these are less commonly used in pregnancy and postpartum and should be discussed with an endocrinologist familiar with them. See the levothyroxine versus NDT versus T3 article for the formulation comparison.
What can disrupt breastfeeding is undertreated thyroid disease. Low free T4 reduces prolactin response and milk supply. If your milk is not coming in, or supply drops around three months postpartum, check thyroid labs before blaming pumping schedule or latch.
Iodine and Selenium in Pregnancy
Iodine requirements rise sharply in pregnancy and lactation. The recommended daily intake goes from 150 mcg in non-pregnant adults to 220 mcg in pregnancy and 290 mcg during breastfeeding. Most U.S. prenatal vitamins now contain 150 mcg of iodine, which together with dietary iodine from dairy, eggs, and iodized salt usually covers the need.
Here is the trap: more is not better. In Hashimoto's specifically, excess iodine can accelerate autoimmune thyroid destruction and push a compensated gland into frank hypothyroidism. Kelp tablets, iodine-heavy seaweed, high-dose iodine supplements (10,000 mcg and up), and povidone-iodine exposures can all trigger flares. Studies from iodine-sufficient countries show a U-shaped relationship: too little is bad, too much is also bad.
Practical guidance for Hashimoto's pregnancy:
- Use a prenatal containing 150 mcg of iodine. Check the label; not all prenatals include it.
- Eat normally — a few eggs a week, some dairy, the occasional seaweed salad — without aiming for high-iodine foods.
- Avoid kelp supplements, iodine tablets, and megadose iodine products unless your endocrinologist specifically prescribes them.
- If you eat a vegan or dairy-free diet, work with a dietitian to confirm iodine intake.
Selenium is the second key micronutrient. Selenium supplementation (200 mcg per day as selenomethionine) lowers TPO antibody titers and, in one Italian trial, reduced the rate of postpartum thyroiditis in TPO-positive women by roughly 50%. Two Brazil nuts a day provide a reasonable food-based dose. See the selenium, zinc, iron, and iodine article for the full micronutrient map.
Practical Tactics — Pills, Prenatals, Travel
Levothyroxine absorption is fragile. A perfect dose badly timed may be no dose at all. Pregnancy adds complications: prenatal vitamins with iron and calcium, morning sickness, changing sleep schedules.
Pill timing. Take levothyroxine on an empty stomach, with plain water, at least 30 to 60 minutes before food, coffee, or any other supplement. The most reliable slot for most women is first thing on waking. If morning sickness makes that impossible, take it at bedtime — at least three hours after your last food. Pick one slot and stay consistent; switching back and forth between morning and night skews your labs.
Iron and calcium block absorption. Prenatal vitamins almost always contain both. Separate your levothyroxine and your prenatal by a minimum of four hours. A common working schedule: levothyroxine at 6 a.m. on waking, prenatal with breakfast at 7:30 or later, iron supplement (if separate) at lunch or dinner.
Morning sickness. If you vomit within an hour of taking levothyroxine, take another dose. The pill was probably not absorbed. Doing this occasionally will not over-medicate you — levothyroxine has a seven-day half-life and single-dose swings barely move steady-state levels.
Travel dose coverage. Levothyroxine tolerates a missed day without drama. If you miss one pill, take it as soon as you remember, or double up the next day. Missing three or more days in a row is where you start losing ground. When traveling, carry your pills in your carry-on, not checked luggage. Pack at least a week's extra. Get a written prescription from your doctor to carry through customs. Time zone changes do not require adjustment — just take your pill at your new local morning time.
Refills and supply. Do not wait until the bottle is empty to refill. Pharmacies sometimes switch between generic manufacturers, and different generics can have absorption differences of up to 12.5%. If you switch manufacturers mid-pregnancy, ask for a TSH check four weeks later to confirm the dose is still right.
Advocating for Yourself at Appointments
Obstetric care in the U.S. is often compressed, and thyroid management can fall between your OB and your endocrinologist — each assuming the other is handling it. You may need to stitch the care together yourself. A few phrases that work:
- "I have Hashimoto's. ATA guidelines say TSH should stay under 2.5 in the first trimester. Can we check labs every four weeks?"
- "My TSH was 3.4. The lab flagged it normal, but for pregnancy that is above target. Can we raise my dose?"
- "I'd like free T4 checked alongside TSH, not TSH alone."
- "Six weeks postpartum I'd like a TSH, free T4, and TPO antibody panel to screen for postpartum thyroiditis."
You are not being difficult. You are doing exactly what the guidelines ask. If your provider pushes back against monitoring that is clearly in the ATA document, bring a printed copy to the next appointment, or ask for a referral to a maternal-fetal medicine specialist or a pregnancy-experienced endocrinologist.
Key Research Papers
Foundational and recent peer-reviewed publications on thyroid disease in pregnancy and the postpartum period — preconception planning, dose adjustment in trimester one, postpartum thyroiditis, and the antibody-and-fertility literature. Each citation links to the full text via DOI.
- Alexander EK, Pearce EN, Brent GA, et al. 2017 Guidelines of the American Thyroid Association for the Diagnosis and Management of Thyroid Disease During Pregnancy and the Postpartum. Thyroid. 2017;27(3):315–389.
- Stagnaro-Green A, Abalovich M, Alexander E, et al. Guidelines of the American Thyroid Association for the Diagnosis and Management of Thyroid Disease During Pregnancy and Postpartum. Thyroid. 2011;21(10):1081–1125.
- Negro R, Formoso G, Mangieri T, Pezzarossa A, Dazzi D, Hassan H. Levothyroxine Treatment in Euthyroid Pregnant Women with Autoimmune Thyroid Disease: Effects on Obstetrical Complications. Journal of Clinical Endocrinology & Metabolism. 2006;91(7):2587–2591.
- Haddow JE, Palomaki GE, Allan WC, et al. Maternal Thyroid Deficiency During Pregnancy and Subsequent Neuropsychological Development of the Child. New England Journal of Medicine. 1999;341(8):549–555.
- Dhillon-Smith RK, Middleton LJ, Sunner KK, et al. Levothyroxine in Women with Thyroid Peroxidase Antibodies before Conception (TABLET Trial). New England Journal of Medicine. 2019;380(14):1316–1325.
- Negro R, Greco G, Mangieri T, Pezzarossa A, Dazzi D, Hassan H. The Influence of Selenium Supplementation on Postpartum Thyroid Status in Pregnant Women with Thyroid Peroxidase Autoantibodies. Journal of Clinical Endocrinology & Metabolism. 2007;92(4):1263–1268.
- Negro R, Schwartz A, Gismondi R, Tinelli A, Mangieri T, Stagnaro-Green A. Universal Screening Versus Case Finding for Detection and Treatment of Thyroid Hormonal Dysfunction During Pregnancy. Journal of Clinical Endocrinology & Metabolism. 2010;95(4):1699–1707.
- Mannisto T, Mendola P, Grewal J, Xie Y, Chen Z, Laughon SK. Thyroid Diseases and Adverse Pregnancy Outcomes in a Contemporary US Cohort. Journal of Clinical Endocrinology & Metabolism. 2013;98(7):2725–2733.
- Casey BM, Thom EA, Peaceman AM, et al. Treatment of Subclinical Hypothyroidism or Hypothyroxinemia in Pregnancy. New England Journal of Medicine. 2017;376(9):815–825.
- Alexander EK, Marqusee E, Lawrence J, Jarolim P, Fischer GA, Larsen PR. Timing and Magnitude of Increases in Levothyroxine Requirements During Pregnancy in Women with Hypothyroidism. New England Journal of Medicine. 2004;351(3):241–249.
- Hollowell JG, Staehling NW, Flanders WD, et al. Serum TSH, T4, and Thyroid Antibodies in the United States Population (NHANES III). Journal of Clinical Endocrinology & Metabolism. 2002;87(2):489–499.
- Zimmermann MB, Boelaert K. Iodine Deficiency and Thyroid Disorders. Lancet Diabetes & Endocrinology. 2015;3(4):286–295.
Live PubMed Searches
Live PubMed queries that update as new papers are indexed.
- PubMed: Hashimoto's in pregnancy
- PubMed: levothyroxine dose adjustment
- PubMed: subclinical hypothyroidism + miscarriage
- PubMed: TPO antibodies + infertility
- PubMed: postpartum thyroiditis
- PubMed: trimester-specific TSH
- PubMed: iodine + pregnancy + Hashimoto's
- PubMed: selenium + postpartum thyroiditis
- PubMed: levothyroxine + breastfeeding
Connections
- Endocrinology
- How Your Thyroid Is Controlled — interactive animation
- Hashimoto's Thyroiditis Overview
- Levothyroxine vs NDT vs T3
- Selenium, Zinc, Iron, and Iodine
- TPO and TgAb Antibodies
- TSH, T4, and T3 Optimal Ranges
- Reverse T3 and Low T3 Syndrome
- Hashimoto, POTS, and MCAS Overlap
- AIP and Gluten Elimination
- Gut-Thyroid Axis and Intestinal Permeability
- Infertility
- Preeclampsia
- Gestational Diabetes
- Perimenopause
- Thyroid Disorders
- Selenium
- Iodine
- Iron
- Polycystic Ovary Syndrome