Vitamin E and Skin Health
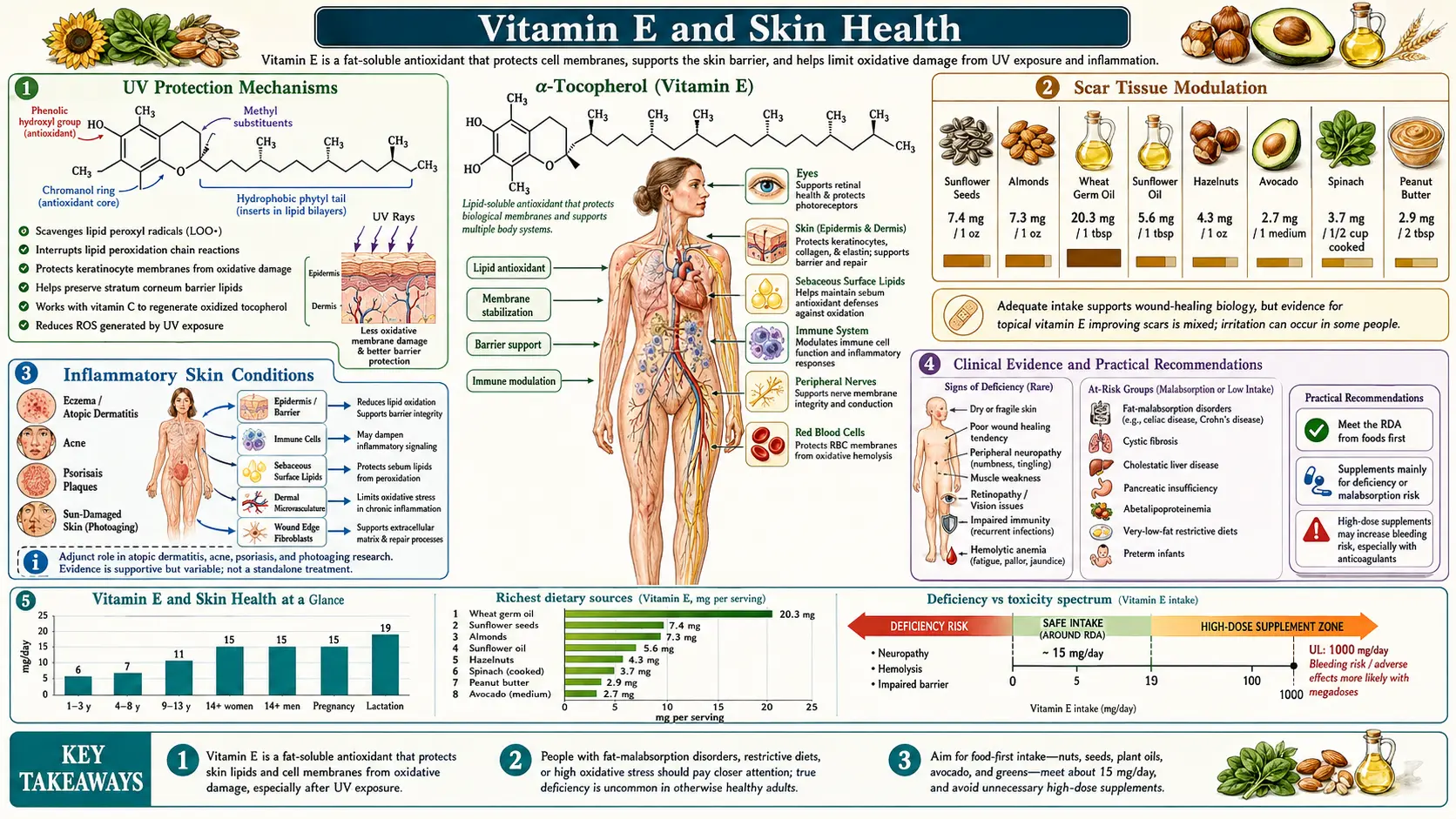
Vitamin E is one of the most important nutrients for skin health, functioning as the skin's primary fat-soluble antioxidant and playing critical roles in UV protection, wound healing, scar modulation, moisture retention, and management of inflammatory skin conditions. The skin is the body's largest organ and its primary interface with the external environment, constantly exposed to ultraviolet radiation, air pollution, chemical irritants, and microbial pathogens — all of which generate reactive oxygen species that damage skin cells, degrade collagen, and accelerate aging. Vitamin E, embedded within the lipid bilayers of skin cell membranes and present in the sebum of the stratum corneum, provides an essential line of defense against these oxidative insults. Both oral supplementation and topical application of Vitamin E have been extensively studied and employed for dermatological benefit, and the synergistic relationship between Vitamin E and Vitamin C in the skin represents one of the best-characterized antioxidant partnerships in dermatology.
Table of Contents
- UV Protection Mechanisms
- Photoaging Prevention
- Wound Healing Acceleration
- Scar Tissue Modulation
- Moisturizing Effects and Skin Barrier Function
- Inflammatory Skin Conditions
- Topical vs. Oral Vitamin E for Skin
- Synergy with Vitamin C for Skin Protection
- Clinical Evidence and Practical Recommendations
- Cautions & Topical Safety
- Key Research Papers
- Connections
- Featured Videos
1. UV Protection Mechanisms
Ultraviolet radiation is the most significant environmental threat to skin health, and Vitamin E provides multiple layers of protection against UV-induced damage.
- Free Radical Scavenging After UV Exposure: UV radiation (both UVA and UVB) generates reactive oxygen species in the skin, including superoxide, singlet oxygen, hydroxyl radicals, and lipid peroxyl radicals. Vitamin E, positioned within skin cell membranes, directly neutralizes these radicals by donating hydrogen atoms from its chromanol ring, preventing the initiation and propagation of lipid peroxidation chain reactions in the skin's lipid-rich structures.
- Sunburn Cell Reduction: UV exposure causes keratinocyte apoptosis, producing characteristic "sunburn cells." Topical and oral Vitamin E have been shown to reduce the formation of sunburn cells following UV exposure, indicating reduced UV-induced cellular damage and apoptosis.
- DNA Damage Protection: UV radiation causes direct DNA damage (thymine dimers) and indirect oxidative DNA damage. Vitamin E's antioxidant activity reduces oxidative DNA damage in skin cells, potentially lowering the risk of UV-induced mutations that can lead to skin cancer.
- Immunosuppression Prevention: UV radiation suppresses local and systemic immune responses, which is believed to contribute to skin cancer development by allowing transformed cells to escape immune surveillance. Vitamin E partially prevents UV-induced immunosuppression by reducing the oxidative signals that trigger immune suppression.
- Erythema Reduction: Both topical and oral Vitamin E supplementation have been shown to reduce the intensity of UV-induced erythema (sunburn redness), indicating reduced inflammatory response to UV exposure.
- Not a Sunscreen Replacement: While Vitamin E provides meaningful photoprotection, it is not a substitute for sunscreen. Vitamin E does not absorb UV radiation as efficiently as sunscreen filters but rather mitigates the downstream oxidative damage caused by UV photons that penetrate the skin.
2. Photoaging Prevention
Photoaging — the premature aging of skin caused by chronic UV exposure — is distinct from chronological aging and is the primary cause of wrinkles, age spots, and loss of skin elasticity in sun-exposed areas.
- Matrix Metalloproteinase (MMP) Inhibition: UV-generated reactive oxygen species activate signaling pathways (AP-1 and NF-kB) that upregulate matrix metalloproteinases — enzymes that degrade collagen, elastin, and other extracellular matrix proteins. Vitamin E reduces ROS levels in UV-exposed skin, thereby reducing MMP activation and collagen degradation.
- Collagen Preservation: By preventing lipid peroxidation and reducing MMP expression, Vitamin E helps preserve the dermal collagen network that provides skin firmness and structural support. Collagen loss is the primary molecular basis of wrinkling and skin sagging.
- Elastin Fiber Protection: Elastin fibers, which provide skin with its elastic recoil properties, are damaged by UV-induced oxidative stress. The resulting "solar elastosis" — characterized by thickened, disorganized, dysfunctional elastin — is a hallmark of photoaged skin. Vitamin E helps protect elastin from oxidative degradation.
- Hyperpigmentation Prevention: UV-induced oxidative stress stimulates melanogenesis (melanin production) through activation of tyrosinase and other melanin synthesis enzymes. Vitamin E's antioxidant effects may help reduce UV-stimulated hyperpigmentation and age spot formation.
- Lipid Peroxidation Product Reduction: Lipid peroxidation products, including malondialdehyde (MDA) and 4-hydroxynonenal (4-HNE), accumulate in photoaged skin and can form cross-links with proteins, contributing to the stiff, leathery quality of severely photoaged skin. Vitamin E reduces the formation of these damaging lipid peroxidation end-products.
3. Wound Healing Acceleration
Vitamin E supports wound healing through mechanisms that operate across all phases of the wound repair process.
- Inflammatory Phase Support: Vitamin E modulates the inflammatory response in wounds by reducing excessive oxidative stress while preserving the oxidative burst needed for antimicrobial defense. It protects immune cells (neutrophils and macrophages) from self-inflicted oxidative damage during the inflammatory phase.
- Fibroblast Protection and Proliferation: Vitamin E protects fibroblast cell membranes from oxidative damage, supporting their survival and proliferation during the proliferative phase of wound healing. Fibroblasts are responsible for synthesizing collagen, elastin, and the extracellular matrix components that form the structural foundation of healing tissue.
- Collagen Synthesis Modulation: While Vitamin C is the primary cofactor for collagen synthesis, Vitamin E supports collagen formation indirectly by protecting fibroblasts and the newly synthesized collagen from oxidative damage. In the remodeling phase, Vitamin E may modulate the balance between collagen synthesis and degradation.
- Angiogenesis Support: Adequate Vitamin E status supports the formation of new blood vessels (angiogenesis) in healing wounds, ensuring adequate oxygen and nutrient delivery to the repair tissue.
- Epithelialization: Vitamin E supports keratinocyte migration and proliferation, promoting the re-epithelialization that closes the wound surface. Topical Vitamin E may provide a moist, antioxidant-rich environment that facilitates this process.
- Post-Surgical Recovery: Some clinical protocols recommend optimizing Vitamin E status before and after surgery to support wound healing, though high-dose supplementation should be balanced against Vitamin E's anti-platelet effects and discussed with the surgical team.
4. Scar Tissue Modulation
Topical Vitamin E is one of the most commonly used home remedies for scar treatment, though the clinical evidence is nuanced.
- Hypertrophic Scar Reduction: Some studies suggest that topical Vitamin E, particularly in combination with silicone-based treatments, can reduce the development of hypertrophic scars by modulating fibroblast activity and collagen cross-linking in healing wounds.
- Keloid Prevention: Limited evidence suggests that Vitamin E may help prevent keloid formation in susceptible individuals, potentially through anti-inflammatory effects and modulation of transforming growth factor beta (TGF-beta) signaling.
- Moisturizing Effect: A significant portion of the scar-improving effect attributed to Vitamin E may be due to the occlusive and moisturizing properties of Vitamin E oil itself, which maintains a hydrated wound environment that supports optimal healing and reduces scar rigidity.
- Mixed Clinical Evidence: A widely cited study by Baumann and Spencer (1999) found that topical Vitamin E did not improve scar appearance and caused contact dermatitis in 33% of subjects. However, other studies have reported benefit, and the discrepancy may relate to the form of Vitamin E used, the timing of application, and individual variation. The evidence base is not strong enough to make definitive recommendations.
- Contact Dermatitis Risk: Topical Vitamin E can cause allergic contact dermatitis in some individuals, characterized by redness, itching, and swelling at the application site. Patch testing before widespread application on healing wounds is advisable.
5. Moisturizing Effects and Skin Barrier Function
Vitamin E contributes to skin hydration and barrier integrity through multiple mechanisms.
- Stratum Corneum Lipid Component: Vitamin E is a natural component of the stratum corneum lipid barrier and the sebum produced by sebaceous glands. It contributes to the lipid matrix that prevents transepidermal water loss (TEWL) and maintains skin hydration.
- Membrane Fluidity Maintenance: By preventing lipid peroxidation in skin cell membranes, Vitamin E maintains membrane fluidity and structural integrity, supporting the barrier function of the epidermis.
- Sebum Delivery: Vitamin E is delivered to the skin surface through sebum secretion. Sebaceous gland activity is a major route by which the body supplies Vitamin E to the skin's surface, where it provides antioxidant protection at the outermost layer.
- Emollient Properties: Vitamin E oil (tocopherol acetate or pure tocopherol) acts as an emollient, softening the skin surface and filling in micro-cracks in the stratum corneum, improving the skin's feel and appearance.
6. Inflammatory Skin Conditions
Vitamin E's anti-inflammatory and antioxidant properties make it relevant to the management of several inflammatory dermatological conditions.
- Eczema (Atopic Dermatitis): Oxidative stress is elevated in atopic dermatitis, and some studies suggest that oral Vitamin E supplementation may reduce disease severity by decreasing oxidative damage and modulating the inflammatory response. Vitamin E's moisturizing properties also benefit the dry, compromised skin barrier characteristic of eczema.
- Psoriasis: Psoriasis involves oxidative stress, chronic inflammation, and hyperproliferation of keratinocytes. Some research suggests that Vitamin E supplementation may provide modest benefit as an adjunct therapy, though it is not a primary treatment for psoriasis.
- Acne: Vitamin E's antioxidant and anti-inflammatory effects may benefit acne by reducing inflammatory mediators and oxidative stress in the pilosebaceous unit. However, heavy topical Vitamin E oils may be comedogenic and could potentially exacerbate acne in some individuals.
- Dermatitis: Vitamin E may help manage contact dermatitis and irritant dermatitis through its anti-inflammatory effects, though paradoxically, topical Vitamin E itself can cause allergic contact dermatitis in susceptible individuals.
7. Topical vs. Oral Vitamin E for Skin
Both topical and oral routes of Vitamin E administration have been studied for skin benefits, each with distinct advantages and limitations.
- Topical Application: Topical Vitamin E delivers the nutrient directly to the skin surface and upper epidermis, achieving high local concentrations at the site where it is needed for UV protection and antioxidant defense. Topical formulations commonly use alpha-tocopherol, alpha-tocopheryl acetate, or alpha-tocopheryl succinate. The free form (alpha-tocopherol) has immediate antioxidant activity, while the ester forms (acetate, succinate) require enzymatic cleavage by skin esterases before becoming active — a process that may be incomplete in the skin.
- Oral Supplementation: Oral Vitamin E is absorbed in the gut, transported via lipoproteins, and delivered to the skin through the bloodstream and sebaceous gland secretion. Oral supplementation provides Vitamin E to all layers of the skin (including the dermis) and protects skin cells from within, but requires 7-14 days of supplementation to meaningfully increase skin Vitamin E levels.
- Combined Approach: The most comprehensive skin protection may come from combining oral and topical Vitamin E, providing both immediate surface protection (topical) and sustained, systemic protection from within (oral).
- Formulation Considerations: The stability of Vitamin E in topical formulations is a significant concern. Alpha-tocopherol is readily oxidized by light and air exposure, losing its antioxidant efficacy. Well-formulated products use airtight, opaque packaging and may include stabilizing agents. Vitamin E serum formulations in combination with Vitamin C and ferulic acid (such as the patented CE Ferulic formulation) have demonstrated superior stability and efficacy.
8. Synergy with Vitamin C for Skin Protection
The combination of Vitamins C and E represents the gold standard for antioxidant skin protection in dermatology.
- Complementary Compartment Coverage: Vitamin E protects the lipid-soluble compartments of the skin (cell membranes, sebum, intercellular lipids) while Vitamin C protects the aqueous compartments (cytoplasm, intercellular fluid). Together, they provide comprehensive antioxidant protection across all compartments of the skin.
- Vitamin E Recycling: Vitamin C regenerates oxidized Vitamin E at the water-lipid interface of skin cell membranes, restoring Vitamin E to its active antioxidant form and extending its protective capacity. This recycling mechanism means that the combination is significantly more effective than either vitamin alone.
- Enhanced Photoprotection: Studies by Sheldon Pinnell and colleagues demonstrated that the combination of topical 15% Vitamin C and 1% Vitamin E provides approximately four-fold greater protection against UV-induced erythema and sunburn cell formation compared to Vitamin C alone. The addition of 0.5% ferulic acid further doubles this protection (CE Ferulic formulation).
- Collagen Synthesis Support: While Vitamin C is the direct cofactor for collagen-synthesizing enzymes (prolyl and lysyl hydroxylases), Vitamin E supports collagen preservation by preventing oxidative degradation of newly synthesized collagen. The combination supports both collagen production and collagen protection.
- Anti-Inflammatory Synergy: Both vitamins independently reduce inflammatory mediators in UV-exposed skin, and their combination provides synergistic anti-inflammatory effects that reduce UV-induced erythema, edema, and immune suppression.
9. Clinical Evidence and Practical Recommendations
The clinical evidence for Vitamin E in skin health spans decades of research, with some applications better supported than others.
- Well-Supported Applications: UV photoprotection (especially in combination with Vitamin C), prevention of lipid peroxidation in skin, maintenance of skin barrier function, and support of wound healing are well-supported by both mechanistic and clinical evidence.
- Moderately Supported Applications: Photoaging prevention, improvement of inflammatory skin conditions (as adjunct therapy), and skin moisturization have moderate clinical support with generally positive but not uniformly consistent results across studies.
- Weakly Supported Applications: Scar reduction with topical Vitamin E has weak and inconsistent clinical evidence, and some studies suggest no benefit or even adverse effects (contact dermatitis). Individual variation in response is substantial.
- Recommended Oral Intake: For general skin health, meeting the RDA of 15 mg/day of alpha-tocopherol through diet or supplementation provides baseline antioxidant protection. Some dermatologists recommend 200-400 IU/day for enhanced skin protection, particularly in individuals with high UV exposure.
- Topical Formulation Selection: Choose stable formulations in airtight, opaque packaging. Combination formulations with Vitamin C and ferulic acid have the strongest evidence base. Apply in the morning under sunscreen for photoprotection, or in the evening for overnight repair support.
- Dietary Sources for Skin Health: Almonds, sunflower seeds, avocados, olive oil, and leafy greens provide dietary Vitamin E along with other skin-supporting nutrients. A diet rich in these foods, combined with adequate Vitamin C intake from fruits and vegetables, provides a strong nutritional foundation for skin health.
Cautions & Topical Safety
While both oral and topical Vitamin E have well-established benefits for skin, several safety and practical considerations apply:
- Contact dermatitis from topical Vitamin E — the Baumann & Spencer 1999 study found that 33% of subjects developed contact dermatitis from topical Vitamin E applied to scars. The reaction presents as redness, itching, and small bumps at the application site. Patch test on a small area of inner forearm for 7 days before applying widely on the face or healing wounds.
- Comedogenic potential in acne-prone skin — pure Vitamin E oil is heavy and occlusive. Applied to acne-prone facial skin, it can clog pores and worsen comedonal acne. People with acne should prefer lighter Vitamin E formulations (typically combined with Vitamin C in a serum) or apply Vitamin E only to non-acne-prone body areas.
- Formulation stability matters — alpha-tocopherol is rapidly oxidized by light and air, losing antioxidant efficacy. Choose products in airtight, opaque packaging. The CE Ferulic combination (15% Vitamin C + 1% Vitamin E + 0.5% ferulic acid, pH 2.5-3.5) is the most-studied stable topical formulation.
- Ester forms are inactive on the skin surface — tocopheryl acetate and tocopheryl succinate (the cheap, stable ester forms in most cosmetic products) require enzymatic cleavage by skin esterases before becoming active antioxidants. This cleavage is incomplete and slow in the stratum corneum, so ester forms provide less surface antioxidant protection than free alpha-tocopherol. For active photoprotection, free tocopherol is preferred — even though it is less stable.
- Not a sunscreen replacement — Vitamin E absorbs UV light only weakly. It reduces downstream oxidative damage but does NOT prevent UV photons from reaching DNA. Always use a broad-spectrum SPF 30+ sunscreen for primary UV protection; Vitamin E (oral and/or topical) is an adjunct, not a substitute.
- Oral high-dose for skin — high-dose oral alpha-tocopherol (>400 IU/day) for skin photoprotection carries the same systemic risks as any other high-dose use (bleeding, hemorrhagic stroke, possible prostate cancer signal). For skin-only goals, lower doses (200 IU) plus topical application are safer than oral megadoses.
- Pre-procedure use — before laser resurfacing, microneedling, or chemical peel, stop high-dose oral Vitamin E 2 weeks before due to bleeding/bruising risk. Some dermatologists allow topical Vitamin E up until the day before; check with your provider.
- Pregnancy — topical Vitamin E is considered safe in pregnancy. High-dose oral supplementation during pregnancy is not recommended without OB guidance because some studies have raised concerns about pregnancy outcomes.
- Scar treatment realistic expectations — the evidence does NOT support routine topical Vitamin E for surgical scars, hypertrophic scars, or keloids. Silicone gel sheeting has better-quality evidence. If you try Vitamin E for a scar, do so AFTER initial wound healing is complete (3+ weeks post-injury), patch test first, and discontinue if any irritation develops.
- Recommended skin protocol — for daily skin health: morning topical Vitamin C + Vitamin E + ferulic acid serum under broad-spectrum SPF 30+ sunscreen; evening retinoid (separate from Vitamin E to avoid product interaction); oral 200 IU mixed-tocopherol Vitamin E if dietary intake is low; whole-food sources (almonds, sunflower seeds, avocado, olive oil).
Key Research Papers
- Lin JY et al. (2003). UV photoprotection by combination topical antioxidants vitamin C and vitamin E. Journal of the American Academy of Dermatology. — PubMed
- Lin FH et al. (2005). Ferulic acid stabilizes a solution of vitamins C and E and doubles its photoprotection of skin (CE Ferulic formulation). Journal of Investigative Dermatology. — PubMed
- Burke KE et al. (2000). Effects of topical and oral vitamin E on pigmentation and skin cancer induced by ultraviolet irradiation in Skh:2 hairless mice. Nutrition and Cancer. — PubMed
- Baumann LS & Spencer J (1999). The effects of topical vitamin E on the cosmetic appearance of scars. Dermatologic Surgery. — PubMed
- Thiele JJ et al. (2005). Vitamin E in human skin: organ-specific physiology and considerations for its use in dermatology. Molecular Aspects of Medicine. — PubMed
- Eberlein-König B et al. (1998). Protective effect against sunburn of combined systemic ascorbic acid (vitamin C) and d-alpha-tocopherol (vitamin E). Journal of the American Academy of Dermatology. — PubMed
- Trevithick JR et al. (1992). Topical tocopherol acetate reduces post-UVB, sunburn-associated erythema, edema, and skin sensitivity in hairless mice. Archives of Biochemistry and Biophysics. — PubMed
- Tsoureli-Nikita E et al. (2002). Evaluation of dietary intake of vitamin E in the treatment of atopic dermatitis: a study of the clinical course and evaluation of the immunoglobulin E serum levels. International Journal of Dermatology. — PubMed
- Keen MA & Hassan I (2016). Vitamin E in dermatology. Indian Dermatology Online Journal. — PubMed
- Yamamoto Y & Niki E (1988). Action of antioxidants in the membrane: vitamin E and ascorbic acid. BioFactors. — PubMed
- Packer L et al. (2001). Molecular aspects of alpha-tocotrienol antioxidant action and cell signalling. Journal of Nutrition. — PubMed
- Nachbar F & Korting HC (1995). The role of vitamin E in normal and damaged skin. Journal of Molecular Medicine. — PubMed
PubMed Topic Searches
- Vitamin E and skin photoprotection
- Alpha-tocopherol and UV damage in skin
- Vitamin C, Vitamin E, and ferulic acid (topical skin)
- Vitamin E and wound healing
- Topical Vitamin E and scar appearance
- Vitamin E and photoaging
- Vitamin E and atopic dermatitis
- Tocotrienols and skin
- Vitamin E and stratum corneum/skin barrier
- Vitamin E and skin lipid peroxidation
- Topical tocopherol and contact dermatitis
- Vitamin E and psoriasis
Connections
- Vitamin E (Main Page)
- Vitamin E Benefits Hub
- Vitamin E and Heart Health
- Vitamin E and Immune Function
- Tocotrienols — The Other Vitamin E Family
- Vitamin C
- Vitamin C and Collagen
- Vitamin A
- Vitamin D3
- Zinc
- Selenium
- Collagen
- Oxidative Stress
- Immune Boosting
- Psoriasis
- Acne
- Eczema
- Olive Oil
- Almonds