Tocotrienols — The Other Vitamin E Family (Palm, Annatto, Rice Bran)
"Vitamin E" is not one molecule but a family of eight. Most Vitamin E supplements and almost all clinical trials have studied just one of them — alpha-tocopherol — while the other seven, especially the four tocotrienols, have very different biological properties. Tocotrienols are 40-60× more potent than tocopherols for some antioxidant indications, uniquely inhibit cholesterol synthesis at the HMG-CoA reductase step (the same enzyme statins target), and produce neuroprotective and anti-cancer effects at concentrations where alpha-tocopherol does nothing. This page covers why the tocotrienol forms matter, the best sources (palm, annatto, rice bran), the major clinical trials (Magosso 2013 NAFLD trial, gamma-tocotrienol breast cancer trials, alpha-tocotrienol stroke protection), and why a tocopherol-only Vitamin E supplement may actually deplete the more potent tocotrienol forms.
Table of Contents
- The Eight Vitamin E Isomers
- Why Tocotrienols Are 40-60× More Potent
- Sources: Palm, Annatto, and Rice Bran
- Cardiovascular: HMG-CoA Reductase and Delta-Tocotrienol
- Liver Health: The Magosso 2013 NAFLD Trial
- Neuroprotection: Alpha-Tocotrienol's Unique Brain Effects
- Anti-Cancer: Gamma-Tocotrienol in Breast and Pancreatic Cancer
- Bone, Skin, and Anti-Aging
- The Alpha-Tocopherol Displacement Problem
- Practical Supplementation Protocol
- Cautions & Drug Interactions
- Key Research Papers
- Connections
- Featured Videos
1. The Eight Vitamin E Isomers
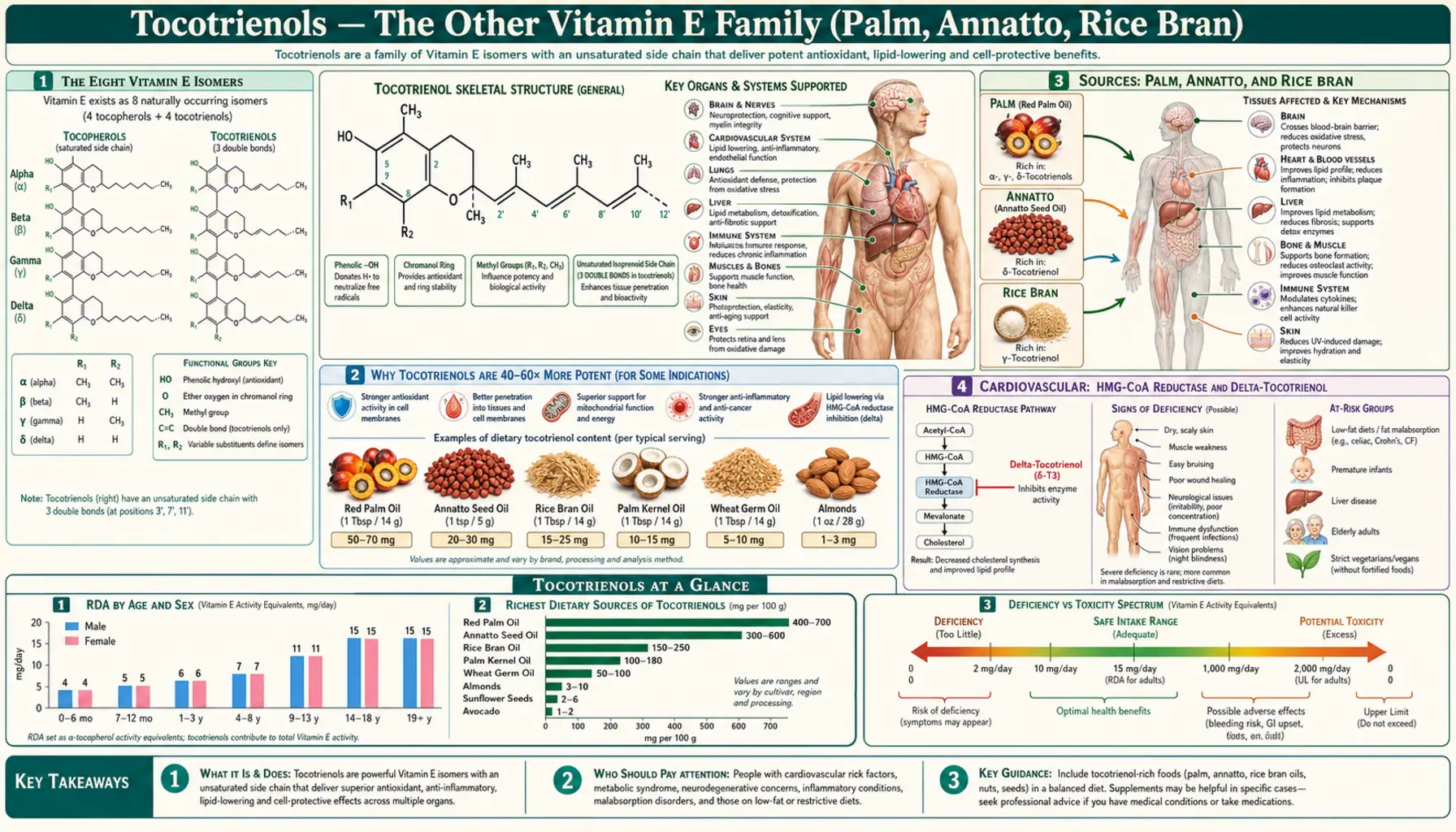
"Vitamin E" is a family name for eight naturally occurring molecules that share a chromanol ring (the antioxidant business end) attached to a 16-carbon side chain. The eight split into two sub-families based on the side chain:
- Tocopherols (4 forms) — saturated phytyl side chain (no double bonds). Alpha, beta, gamma, and delta forms differ by the position and number of methyl groups on the chromanol ring.
- Tocotrienols (4 forms) — unsaturated farnesyl side chain (three double bonds in the tail). Same four methylation patterns: alpha, beta, gamma, delta tocotrienol.
The three double bonds in the tocotrienol tail are the key structural difference. The unsaturated tail is more flexible, lets the molecule penetrate more deeply into the fatty interior of cell membranes, and exposes the active chromanol ring to a wider area — which is why tocotrienols are recycled faster and intercept lipid radicals more efficiently than tocopherols at the same concentration.
The methylation pattern on the chromanol ring matters too. Alpha forms have three methyls (one each at positions 5, 7, and 8). Beta forms have methyls at 5 and 8. Gamma forms have methyls at 7 and 8. Delta forms have only one methyl, at position 8. The fewer the methyls, the more open the position 5 on the ring is for trapping reactive nitrogen species like peroxynitrite — which is why gamma-tocopherol/tocotrienol traps reactive nitrogen species that alpha-forms cannot.
Of the eight, alpha-tocopherol is the one preferentially retained by the liver's alpha-tocopherol transfer protein (α-TTP), incorporated into VLDL, and distributed throughout the body. The other seven are largely metabolized to water-soluble CEHCs (carboxyethyl hydroxychromans) by CYP4F2 and excreted in urine and bile. This is why plasma Vitamin E is mostly alpha-tocopherol — the body actively retains it — but it does NOT mean the other seven forms are unimportant. They simply act locally during their passage through tissues before catabolism.
2. Why Tocotrienols Are 40-60× More Potent (For Some Indications)
"More potent" is widely repeated about tocotrienols but the headline number depends entirely on the indication. Here is what the literature actually supports:
- Lipid peroxidation in membranes — tocotrienols are approximately 40-60× more efficient than alpha-tocopherol at preventing lipid peroxidation in cell membrane models (Serbinova 1991, Free Radical Biology and Medicine). The three reasons: (1) deeper membrane penetration via the unsaturated tail, (2) more uniform distribution across the membrane bilayer, (3) faster recycling by ascorbate at the membrane-water interface.
- Neuroprotection against glutamate excitotoxicity — alpha-tocotrienol protects neurons from glutamate-induced death at nanomolar concentrations (10-50 nM), while alpha-tocopherol requires micromolar concentrations (10-50 μM) for the same effect — a 1000× potency difference in this specific assay (Sen 2000, Journal of Biological Chemistry). The mechanism is inhibition of 12-lipoxygenase, not simple antioxidant activity.
- Cholesterol synthesis inhibition — delta-tocotrienol and gamma-tocotrienol post-transcriptionally suppress HMG-CoA reductase (the rate-limiting enzyme of cholesterol synthesis — the same enzyme inhibited by statin drugs). Alpha-tocopherol does NOT do this; it actually antagonizes the tocotrienol cholesterol-lowering effect.
- Apoptosis induction in cancer cells — gamma- and delta-tocotrienol induce apoptosis in breast cancer, pancreatic cancer, and prostate cancer cell lines at micromolar concentrations where alpha-tocopherol is inactive.
- Standard linoleate-radical scavenging — for the basic chemistry of intercepting a peroxyl radical in solution, alpha-tocopherol and alpha-tocotrienol are similar. The "40-60×" advantage shows up only in membrane and cellular contexts where geometry matters.
The honest summary: tocotrienols are NOT a universal "stronger Vitamin E." They are differently potent for specific indications — dramatically better than alpha-tocopherol for neuroprotection, cholesterol modulation, and cancer-cell apoptosis; comparable for ordinary antioxidant chemistry. For these specific indications, gamma-tocotrienol or delta-tocotrienol from annatto is the rational supplement choice; for general dietary adequacy, mixed tocopherols from nuts and seeds remain the foundation.
3. Sources: Palm, Annatto, and Rice Bran
Tocotrienols are uncommon in the typical Western diet. Sunflower oil, soybean oil, corn oil, almonds — all the standard "Vitamin E" foods — provide almost exclusively tocopherols, not tocotrienols. The three concentrated dietary sources are:
- Palm oil (red palm fruit) — contains a mixed tocotrienol fraction (TRF) of approximately 70% tocotrienols and 30% tocopherols. The four tocotrienols (alpha, beta, gamma, delta) are all present, with alpha and gamma typically the most abundant. Palm tocotrienol-rich fraction (Palm TRF) is the source for most cardiovascular and liver clinical trials. Sustainable, RSPO-certified palm oil is the preferred sourcing.
- Annatto seeds (Bixa orellana) — produces a tocotrienol extract that is approximately 90% delta-tocotrienol and 10% gamma-tocotrienol, with virtually NO tocopherols. This near-pure tocotrienol profile is preferred for indications where the alpha-tocopherol displacement effect matters (cancer-prevention research, cholesterol indications). Brand examples include EVNol SupraBio (an emulsified delivery system) and DeltaGold annatto tocotrienol.
- Rice bran oil — contains modest amounts of all four tocotrienols along with gamma-oryzanol (a separate cholesterol-modulating compound). The total tocotrienol content per gram is lower than palm or annatto, but the dietary use of rice bran oil in Asian cuisines provides meaningful cumulative intake.
Other minor sources include barley, oats, and certain wheat varieties (containing primarily alpha-tocotrienol), and some emerging interest in coconut oil byproducts. None of these reach the concentrations of palm or annatto.
The U.S. dietary intake of total tocotrienols is estimated at <5 mg/day for most adults — effectively zero for the targeted clinical effects discussed below, which typically require 100-300 mg/day of mixed tocotrienols from supplementation.
4. Cardiovascular: HMG-CoA Reductase and Delta-Tocotrienol
The single most distinctive cardiovascular mechanism of tocotrienols is post-transcriptional inhibition of HMG-CoA reductase — the rate-limiting enzyme in cholesterol synthesis. Statin drugs (atorvastatin, rosuvastatin, simvastatin) competitively inhibit the active site of this enzyme. Tocotrienols work upstream: they accelerate the degradation of the enzyme protein itself, reducing the total amount of HMG-CoA reductase in the cell.
- Delta-tocotrienol is the most potent for this effect, followed by gamma-tocotrienol. Alpha-tocotrienol is weaker. Alpha-tocopherol does NOT inhibit HMG-CoA reductase — and at concentrations above ~1 μM, alpha-tocopherol actually antagonizes the cholesterol-lowering effect of tocotrienols (Qureshi 1996 work at USDA).
- Clinical effects — Palm and annatto tocotrienol supplementation at 100-300 mg/day produces modest total-cholesterol reductions (typically 10-15%) and LDL reductions in the 15-20% range across multiple controlled trials. This is less than statin-grade reduction (30-50%) but is meaningful for patients who cannot tolerate statins or who prefer a food-derived approach.
- Anti-platelet effects — tocotrienols reduce platelet aggregation through similar mechanisms as tocopherols (PKC inhibition, thromboxane reduction).
- Endothelial function — tocotrienols improve nitric oxide bioavailability and reduce inflammatory adhesion molecule expression on vascular endothelium.
- Carotid atherosclerosis regression — the Tomeo 1995 trial (small, 50 patients, palm tocotrienols + standard care for 18 months) reported stabilization or modest regression of carotid plaques by duplex ultrasound in the tocotrienol group versus progression in controls. The trial was small and has not been definitively replicated, but suggests tocotrienols may go beyond statin-like LDL lowering to affect plaque biology directly.
For patients on statins, adding tocotrienols can produce additive LDL reduction but the combination needs medical supervision. For patients avoiding statins, mixed tocotrienols are a defensible adjunct to dietary cholesterol management — with the understanding that the absolute LDL effect is smaller than statin therapy.
5. Liver Health: The Magosso 2013 NAFLD Trial
Non-alcoholic fatty liver disease (NAFLD) is now the most common chronic liver disease worldwide, driven primarily by metabolic syndrome, insulin resistance, and dietary fructose. There is no FDA-approved drug for NAFLD; treatment is lifestyle-based. Both alpha-tocopherol (the PIVENS trial, 800 IU/day) and tocotrienols (multiple smaller trials) have evidence for benefit.
The pivotal tocotrienol trial is Magosso et al. 2013 (Nutrition Journal): 87 patients with ultrasound-diagnosed fatty liver, randomized to mixed palm tocotrienols 200 mg twice daily (400 mg/day total) or placebo for 12 months. Primary outcome: ultrasound remission of hepatic steatosis.
- 50% of tocotrienol group achieved normalization of ultrasound steatosis grade versus 23% for placebo (p < 0.05)
- ALT and AST liver enzymes improved significantly in the tocotrienol group
- Treatment was well tolerated; no significant adverse events
- The required duration was long (12 months) — consistent with how slowly steatosis resolves on any intervention
Mechanism: tocotrienols address NAFLD through multiple pathways simultaneously — reduced lipid peroxidation in hepatocyte membranes, inhibition of HMG-CoA reductase (reducing intrahepatic cholesterol burden), Nrf2 pathway activation (upregulating endogenous antioxidant enzymes), reduction of TNF-alpha and inflammatory cytokine signaling, and modest improvement of insulin sensitivity. This multimodal action is well-suited to a multifactorial disease like NAFLD.
For patients with biopsy-proven NASH (the inflammatory advanced form of NAFLD), the conventional recommendation remains alpha-tocopherol 800 IU/day based on the PIVENS trial (men and post-menopausal women; not for diabetics due to mortality signal in some analyses). Mixed tocotrienols can be considered as an alternative or adjunct, particularly for patients where the alpha-tocopherol concerns are relevant.
6. Neuroprotection: Alpha-Tocotrienol's Unique Brain Effects
Alpha-tocotrienol is the most-studied neuroprotective tocotrienol, with effects mediated through mechanisms independent of and additive to its antioxidant activity. Chandan Sen and colleagues at Ohio State (and later at Indiana) have published most of the foundational work.
- 12-Lipoxygenase inhibition — alpha-tocotrienol inhibits 12-lipoxygenase, the enzyme that produces 12-HPETE (a lipid signaling molecule that drives glutamate-induced neuron death in stroke). Alpha-tocopherol does NOT inhibit 12-LOX. This is why alpha-tocotrienol protects neurons against glutamate excitotoxicity at nanomolar concentrations while alpha-tocopherol fails at micromolar concentrations.
- c-Src kinase suppression — alpha-tocotrienol blocks c-Src activation in neurons, another non-antioxidant signaling effect relevant to stroke and traumatic brain injury.
- Stroke models — in canine and primate stroke models, alpha-tocotrienol supplementation before middle cerebral artery occlusion significantly reduces infarct volume and improves functional outcomes. The effect persists when supplementation begins before the stroke; post-stroke initiation has been less consistently studied.
- White matter preservation — supplementation studies in healthy adults using diffusion tensor imaging have shown that tocotrienol supplementation may slow the age-related decline in cerebral white matter integrity.
- Cognitive effects in older adults — small trials of mixed tocotrienol supplementation in cognitively healthy older adults have suggested modest improvements in some cognitive domains, though larger and longer trials are needed.
For neuroprotection, the rational supplement choice is mixed tocotrienols from palm sources (containing alpha-tocotrienol along with the other isomers) at doses around 100-200 mg/day. Annatto delta-tocotrienol alone is less appropriate for neurological indications because alpha-tocotrienol is the most neuroprotective form.
7. Anti-Cancer: Gamma-Tocotrienol in Breast and Pancreatic Cancer
The anti-cancer literature on tocotrienols is large in preclinical (cell culture and animal) work but limited in human trial data. The most-developed indications:
- Breast cancer — gamma-tocotrienol and delta-tocotrienol induce apoptosis in estrogen-receptor positive and triple-negative breast cancer cell lines through multiple mechanisms (caspase activation, NF-kB inhibition, downregulation of survival proteins like Bcl-2). The Nesaretnam group (Malaysian Palm Oil Board) has published most of this work. A small Phase I-II breast cancer trial of palm tocotrienol-rich fraction as adjunct to tamoxifen suggested a modestly improved disease-free survival signal but was not adequately powered.
- Pancreatic cancer — delta-tocotrienol has been investigated as an adjunct to gemcitabine in pancreatic cancer. The mechanism is sensitization of resistant pancreatic cancer cells to chemotherapy through NF-kB pathway inhibition. A Phase I trial established safety; Phase II efficacy data are emerging.
- Prostate cancer — given the SELECT trial's signal that alpha-tocopherol monotherapy may increase prostate cancer risk, there is interest in whether the other Vitamin E forms (especially gamma-tocopherol and tocotrienols) might do the opposite. Preclinical data are encouraging; large human trials are not yet available.
- Radiation protection — gamma-tocotrienol has been investigated by the U.S. military as a potential radiation countermeasure (for nuclear accident scenarios). Animal studies show it protects hematopoietic stem cells from radiation injury when given before radiation exposure.
For cancer prevention or adjunct use, tocotrienol supplementation should be discussed with the treating oncologist — particularly because some chemotherapy agents (cisplatin, doxorubicin) rely partly on oxidative stress for their cytotoxic effect, and antioxidants might theoretically interfere. The interaction in practice is unclear and likely depends on the specific chemotherapy and tumor type.
8. Bone, Skin, and Anti-Aging
- Bone health — tocotrienols (particularly gamma and delta) have shown bone-preserving effects in ovariectomized rat models of postmenopausal osteoporosis. They appear to upregulate osteoblast (bone-forming cell) activity and downregulate osteoclast (bone-resorbing cell) activity. Human trial data are emerging from Malaysia.
- Skin photoaging — tocotrienols penetrate the stratum corneum more effectively than tocopherols when applied topically, and reach deeper skin layers. Topical tocotrienol formulations are part of a small but growing dermatological literature on alternative Vitamin E sources for photoaging.
- Hair growth — a small placebo-controlled trial (Beoy 2010, Penang) suggested that 8 months of mixed tocotrienol supplementation (100 mg/day) increased hair count modestly in subjects with androgenic alopecia. Replication is needed.
- Anti-aging mechanism — the overall picture is that tocotrienols favorably affect multiple aging-related pathways: Nrf2-driven antioxidant gene expression, mitochondrial function, inflammatory cytokine reduction, and lipid peroxidation in cell membranes. Whether this translates to a measurable longevity effect in humans is not established.
9. The Alpha-Tocopherol Displacement Problem
A critical point that explains why much of the historical "Vitamin E" trial literature is misleading: high-dose alpha-tocopherol supplementation actively reduces the body's gamma-tocopherol and tocotrienol levels.
Three mechanisms drive this:
- Liver alpha-TTP saturation — the alpha-tocopherol transfer protein in the liver preferentially binds and recirculates alpha-tocopherol. Flooding the system with supplemental alpha-tocopherol saturates alpha-TTP and accelerates the catabolism of all the non-alpha forms (gamma-tocopherol, delta-tocopherol, all four tocotrienols) by CYP4F2.
- Plasma displacement — alpha-tocopherol supplementation at 400-1000 IU/day reduces plasma gamma-tocopherol by 30-50% within weeks.
- Direct antagonism at HMG-CoA reductase — for the cholesterol-lowering mechanism specifically, alpha-tocopherol at high concentrations interferes with the tocotrienol effect on enzyme degradation.
This is why the HOPE, SELECT, and similar large alpha-tocopherol-only trials produced flat or negative results despite the strong biological plausibility of "antioxidants prevent cardiovascular disease." The supplementation regimen actively depleted the very forms (gamma-tocopherol, tocotrienols) that probably do most of the protective work in a normal mixed-tocopherol diet.
The practical implication: if you supplement Vitamin E, prefer mixed-tocopherol + tocotrienol formulations over alpha-tocopherol monotherapy. Reasonable products include:
- Mixed tocopherols (alpha + beta + gamma + delta) without tocotrienols — e.g. Now Foods Gamma E Plus
- Annatto tocotrienols (90% delta + 10% gamma, no tocopherols) — e.g. DeltaGold-based products, taken separately from any tocopherol supplement to avoid the displacement effect
- Palm tocotrienol-rich fraction (TRF) — mixed tocotrienols + some tocopherols — the form used in most cardiovascular and NAFLD trials
10. Practical Supplementation Protocol
If you have decided to add tocotrienols, here is a practical, evidence-based protocol:
Selection
- Cardiovascular / cholesterol focus: annatto delta-tocotrienol 125-250 mg/day OR mixed palm tocotrienol (TRF) 200-400 mg/day. Take separately from alpha-tocopherol supplements (12+ hours apart) to avoid the displacement effect.
- Liver / NAFLD focus: mixed palm tocotrienol 200 mg twice daily (400 mg/day total), per the Magosso 2013 trial protocol. Expect to commit for 6-12 months before reassessment.
- Neuroprotection focus: mixed palm tocotrienol (containing alpha-tocotrienol) 100-200 mg/day. Annatto alone is less appropriate because it provides almost no alpha-tocotrienol.
- General antioxidant / mixed indications: mixed tocopherols + tocotrienols (whole Vitamin E complex) 100-200 mg total mixed isomers daily.
Timing & absorption
- Take with a meal containing fat (15+ grams) for adequate absorption. Tocotrienols are fat-soluble and bioavailability from an empty stomach is poor.
- Avoid co-administration with iron supplements (separate by 8+ hours).
- Avoid co-administration with high-dose alpha-tocopherol (separate by 12+ hours or skip alpha-tocopherol entirely).
Monitoring
- For cholesterol indications: baseline and 12-week lipid panel.
- For NAFLD: baseline AST, ALT, GGT, and abdominal ultrasound; repeat at 6 months.
- For all indications: notify physician if on warfarin, antiplatelet drugs, or before any planned surgery.
11. Cautions & Drug Interactions
- Warfarin and antiplatelet drugs — tocotrienols, like tocopherols, have mild anti-platelet effects. Notify the prescribing physician; INR monitoring may need to be more frequent for the first 4 weeks.
- Statins — combination produces additive LDL lowering. Acceptable with monitoring; some patients can reduce statin dose under medical supervision.
- Chemotherapy — discuss with oncologist. Tocotrienols may sensitize some tumors to chemotherapy but could theoretically interfere with the oxidative-stress component of others.
- Pre-surgical discontinuation — stop 2 weeks before elective surgery.
- Pregnancy and breastfeeding — safety data are limited. Conservative recommendation is to avoid high-dose tocotrienol supplementation during pregnancy and breastfeeding unless directed by a clinician.
- Annatto allergy — annatto-derived tocotrienols are theoretically a concern for the rare individuals with annatto/bixin food coloring allergy.
- GI side effects — nausea, bloating, or loose stools occur in a small minority. Taking with a larger meal usually resolves this.
- Drug interaction monitoring — the literature is much smaller for tocotrienols than for alpha-tocopherol. Conservative approach: assume the same interaction profile as Vitamin E in general (anticoagulants, antiplatelets, fish oil, vitamin K).
Key Research Papers
- Serbinova E, Kagan V, Han D, Packer L (1991). Free radical recycling and intramembrane mobility in the antioxidant properties of alpha-tocopherol and alpha-tocotrienol. Free Radical Biology and Medicine. — PubMed
- Sen CK et al. (2000). Molecular basis of vitamin E action: tocotrienol potently inhibits glutamate-induced pp60(c-Src) kinase activation and death of HT4 neuronal cells. Journal of Biological Chemistry. — PubMed
- Qureshi AA et al. (1996). Lowering of serum cholesterol in hypercholesterolemic humans by tocotrienols (palmvitee). American Journal of Clinical Nutrition. — PubMed
- Qureshi AA et al. (2002). Synergistic effect of tocotrienol-rich fraction (TRF25) of rice bran and lovastatin on lipid parameters in hypercholesterolemic humans. Journal of Nutritional Biochemistry. — PubMed
- Magosso E et al. (2013). Tocotrienols for normalisation of hepatic echogenic response in nonalcoholic fatty liver: a randomised placebo-controlled clinical trial. Nutrition Journal. — PubMed
- Tomeo AC et al. (1995). Antioxidant effects of tocotrienols in patients with hyperlipidemia and carotid stenosis. Lipids. — PubMed
- Khanna S et al. (2005). Molecular basis of vitamin E action: tocotrienol modulates 12-lipoxygenase, a key mediator of glutamate-induced neurodegeneration. Journal of Biological Chemistry. — PubMed
- Nesaretnam K et al. (2010). Tocotrienol-rich fraction from palm oil and gene expression in human breast cancer cells. Annals of the New York Academy of Sciences. — PubMed
- Springett GM et al. (2015). A Phase I safety, pharmacokinetic, and pharmacodynamic presurgical trial of vitamin E delta-tocotrienol in patients with pancreatic ductal neoplasia. EBioMedicine. — PubMed
- Sen CK et al. (2007). Tocotrienols: the natural vitamin E to defend the nervous system? Annals of the New York Academy of Sciences. — PubMed
- Beoy LA, Woei WJ, Hay YK (2010). Effects of tocotrienol supplementation on hair growth in human volunteers. Tropical Life Sciences Research. — PubMed
- Aggarwal BB et al. (2010). Tocotrienols, the vitamin E of the 21st century: its potential against cancer and other chronic diseases. Biochemical Pharmacology. — PubMed
- Patel V et al. (2012). Oral tocotrienols are transported to human tissues and delay the progression of the model for end-stage liver disease score in patients. Journal of Nutrition. — PubMed
- Yam ML et al. (2009). Tocotrienols suppress proatherogenic chemokines and adhesion molecules in TNF-alpha-stimulated human plasma cells. Inflammation Research. — PubMed
PubMed Topic Searches
- Tocotrienols and HMG-CoA reductase
- Delta-tocotrienol (annatto)
- Alpha-tocotrienol and neuroprotection
- Palm tocotrienol-rich fraction (TRF)
- Tocotrienols and NAFLD
- Gamma-tocotrienol and breast cancer
- Tocotrienols and pancreatic cancer
- Tocotrienols and bone health
- Tocotrienols and radiation protection
- Alpha-tocopherol displacement of tocotrienols
- Mixed tocopherol + tocotrienol supplementation
- Rice bran oil and tocotrienols
Connections
- Vitamin E (Main Page)
- Vitamin E Benefits Hub
- Vitamin E and Heart Health
- Vitamin E and Immune Function
- Vitamin E and Skin Health
- Cardiovascular Disease
- Atherosclerosis
- Stroke
- NAFLD / NASH
- Cancer
- Stroke
- Vitamin C
- Vitamin A
- Selenium
- Oxidative Stress
- Olive Oil
- Almonds
- Tocotrienols — the dedicated antioxidant page for this half of the Vitamin E family.