Vitamin C and Collagen Synthesis
Collagen is the most abundant protein in the human body, accounting for roughly 30% of total protein mass and providing the structural scaffold for skin, tendons, ligaments, cartilage, bone, blood vessels, and virtually every organ system. Vitamin C (ascorbic acid) is the non-negotiable cofactor for the iron-dependent dioxygenases (prolyl hydroxylase and lysyl hydroxylase) that hydroxylate proline and lysine residues in nascent procollagen — the single biochemical step that allows the collagen triple helix to fold and stabilize at body temperature. When ascorbate runs out, connective tissue fails catastrophically, producing the hemorrhages, tooth loss, and wound breakdown that define scurvy. This article walks through the biochemistry, the clinical implications for skin, wounds, bone, cartilage, and vessels, and the landmark papers that underpin modern practice.
Interactive Visualization Vitamin C, Collagen & Why Sailors Fell Apart Zip three protein chains into the strongest rope in biology — then take the vitamin C away and watch the helix unravel, and old healed scars split back open. Launch →Table of Contents
- Key Health Benefits at a Glance
- Prolyl Hydroxylase and Lysyl Hydroxylase Biochemistry
- Collagen Triple Helix Formation
- Scurvy: Collagen Failure in Action
- Skin Health and Anti-Aging
- Wound Healing Phases
- Joint and Cartilage Support
- Blood Vessel Integrity
- Bone Collagen Matrix
- Periodontal Health
- Surgical Recovery
- Topical Vitamin C for Skin
- Clinical Applications and Recommendations
- Research Papers and References
- Connections
- Featured Videos
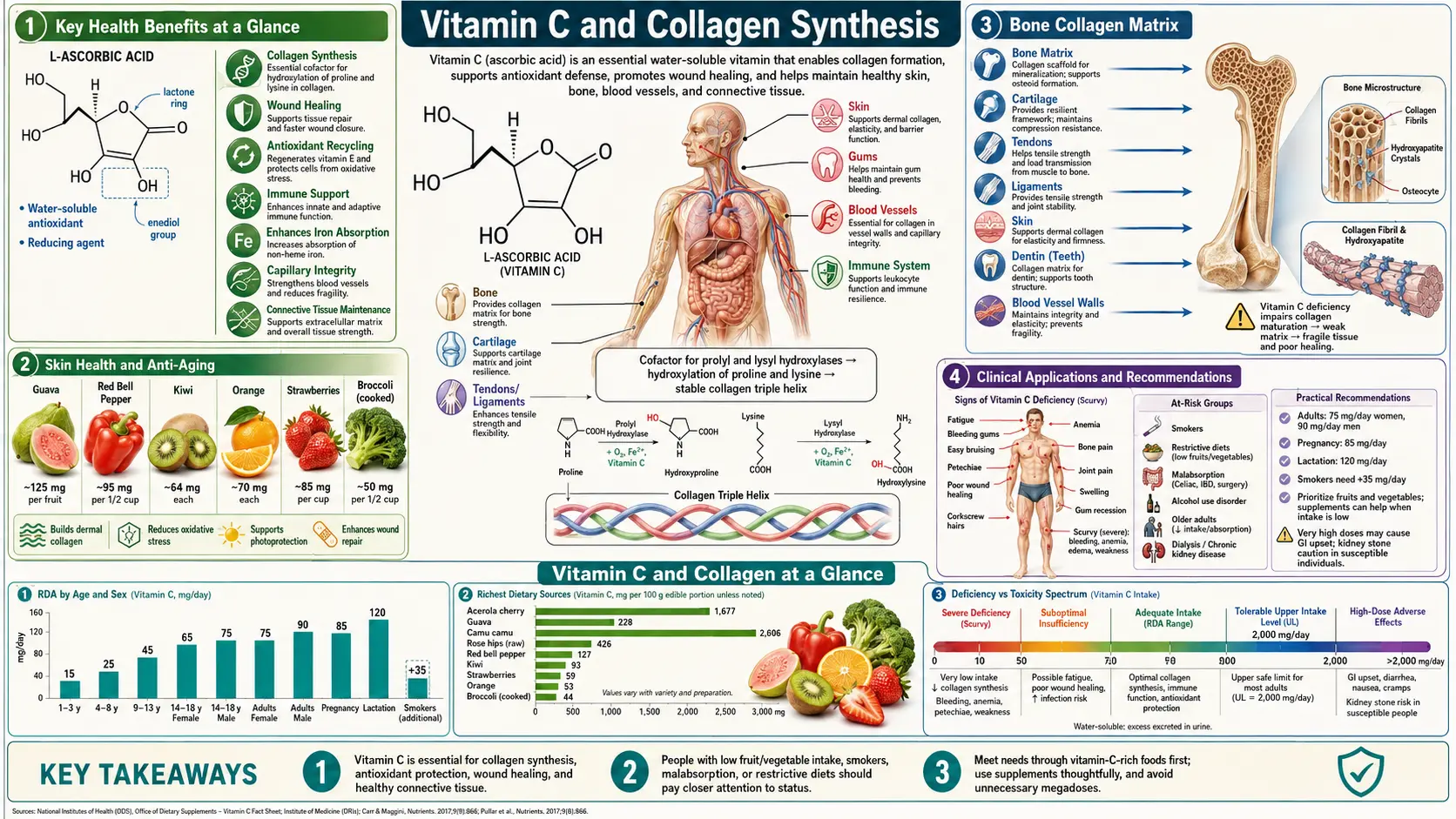
Key Health Benefits at a Glance
Before the mechanism-level detail, the following is a high-level summary of the evidence-backed benefits of adequate vitamin C status for collagen-dependent tissues. Each bullet is explored in more depth below, with supporting studies in the Research Papers section.
- Enables collagen triple-helix formation – Ascorbate regenerates the Fe2+ active site of prolyl and lysyl hydroxylases, allowing procollagen proline and lysine residues to be hydroxylated and the helix to become stable at body temperature.
- Prevents scurvy – Even modest daily intakes (10–40 mg) prevent overt scurvy; the Levine pharmacokinetic studies established the dose-response for plasma and tissue saturation.
- Supports wound healing – Vitamin C drives fibroblast collagen deposition, angiogenesis, and the proliferative phase of tissue repair; deficiency impairs wound strength and dehiscence rates climb.
- Reduces post-fracture complex regional pain syndrome (CRPS) – Meta-analyses of perioperative 500 mg/day vitamin C following distal radius fracture suggest a ~50% reduction in CRPS incidence.
- Slows dermal collagen loss – Higher dietary vitamin C intake correlates with fewer wrinkles, better hydration, and less photoaging in large cross-sectional skin-aging studies.
- Protects bone matrix – Type I collagen makes up ~90% of the organic matrix of bone; ascorbate supports osteoblast collagen deposition and is linked with higher bone mineral density in older adults.
- Maintains articular cartilage – Type II collagen and proteoglycan synthesis by chondrocytes requires ascorbate; higher intakes are associated with slower osteoarthritis progression in the Framingham cohort.
- Supports vascular integrity – Type I, III, and IV collagens in vessel walls and basement membranes depend on ascorbate for synthesis and maintenance.
- Protects periodontal ligament – Collagen-rich gingival tissue and periodontal ligament are vitamin C-sensitive, as the historical progression of scurvy makes clear.
- Enhances topical skin rejuvenation – L-ascorbic acid at 10–20% (pH < 3.5) increases dermal collagen synthesis and photoprotection, with synergy when combined with vitamin E and ferulic acid.
Prolyl Hydroxylase and Lysyl Hydroxylase Biochemistry
The synthesis of mature, functional collagen depends on two classes of iron-dependent dioxygenase enzymes for which vitamin C is an essential cofactor.
- Prolyl 4-Hydroxylase (P4H) – This enzyme catalyzes the hydroxylation of proline residues at the 4-position in nascent procollagen chains. The reaction requires molecular oxygen, ferrous iron (Fe2+), 2-oxoglutarate (alpha-ketoglutarate), and ascorbate. During each catalytic cycle, the iron center is oxidized from Fe2+ to Fe3+; ascorbate serves as the reducing agent that regenerates the active Fe2+ form, preventing irreversible enzyme inactivation. Without vitamin C, prolyl hydroxylase rapidly becomes inactive, and collagen synthesis halts.
- Prolyl 3-Hydroxylase – A related enzyme that hydroxylates specific proline residues at the 3-position, also requiring ascorbate as a cofactor. This modification is less common but critical for certain collagen types, particularly type IV collagen found in basement membranes.
- Lysyl Hydroxylase (PLOD) – This enzyme hydroxylates lysine residues in collagen, producing hydroxylysine. These hydroxylysine residues serve as attachment sites for galactose and glucosylgalactose carbohydrate units, and are essential for the formation of stable intermolecular cross-links that give collagen fibers their tensile strength. Three isoforms (PLOD1, PLOD2, PLOD3) exist with distinct tissue distributions and substrate specificities.
- Stoichiometry – In a typical collagen molecule, approximately 50% of proline residues are hydroxylated to hydroxyproline. Each hydroxylation reaction consumes one molecule of ascorbate. Given the enormous rate of collagen turnover in the body (estimated at 2 to 5 grams daily), the demand for vitamin C in collagen synthesis alone is substantial.
Collagen Triple Helix Formation
- Hydroxyproline and Helix Stability – The triple helical structure of collagen depends critically on 4-hydroxyproline residues. Hydroxyproline forms hydrogen bonds via its hydroxyl group with water molecules that bridge adjacent chains, stabilizing the triple helix. The melting temperature of fully hydroxylated collagen is approximately 42 degrees Celsius, safely above body temperature. Under-hydroxylated collagen has a melting temperature below 37 degrees Celsius and cannot maintain its helical structure at physiological temperature.
- Procollagen Processing – Properly hydroxylated and folded procollagen molecules are secreted from fibroblasts into the extracellular space, where N-terminal and C-terminal propeptides are cleaved by specific proteinases. The resulting tropocollagen molecules self-assemble into collagen fibrils in a quarter-staggered array.
- Cross-Linking – Lysyl oxidase then catalyzes the oxidative deamination of lysine and hydroxylysine residues to form allysine, which participates in covalent cross-link formation between adjacent tropocollagen molecules. These cross-links provide the extraordinary tensile strength of mature collagen fibers.
Scurvy: Collagen Failure in Action
Scurvy represents the clinical manifestation of vitamin C deficiency and serves as a dramatic demonstration of the importance of ascorbate in collagen maintenance.
- Timeline – Body stores of vitamin C are typically 1,500 to 2,000 mg in well-nourished individuals. Clinical symptoms of scurvy appear after 1 to 3 months of dietary intake below 10 mg daily, when body stores fall below 300 mg.
- Early Symptoms – Fatigue, malaise, and inflammation of the gums (gingivitis) are among the earliest signs. Perifollicular hemorrhages (bleeding around hair follicles) and corkscrew hairs reflect weakened connective tissue around hair shafts.
- Progressive Disease – Advanced scurvy features widespread hemorrhage (ecchymoses, petechiae), poor wound healing, loosening and loss of teeth due to weakened periodontal ligaments, joint pain and swelling from subperiosteal hemorrhage, and anemia. Existing wounds may reopen as previously deposited collagen degrades without vitamin C-dependent maintenance.
- Fatal Outcomes – If untreated, scurvy progresses to hemopericardium, cerebral hemorrhage, and death. Historically, scurvy killed more sailors than combat, storms, and all other diseases combined during the age of exploration.
Skin Health and Anti-Aging
The dermis contains predominantly type I and type III collagen, which provide skin with its strength, structure, and resilience.
- Dermal Collagen Decline – Skin collagen content decreases by approximately 1% per year after age 20. This decline accelerates after menopause due to estrogen loss. UV radiation (photoaging) further degrades collagen through matrix metalloproteinase (MMP) activation and direct ROS-mediated damage.
- Vitamin C and Collagen Preservation – Adequate vitamin C status supports ongoing dermal collagen synthesis by fibroblasts. Additionally, ascorbate inhibits MMP expression, reducing collagen degradation, and scavenges UV-generated free radicals, protecting existing collagen from oxidative damage.
- Clinical Skin Studies – Higher dietary vitamin C intake correlates with fewer wrinkles, better skin hydration, and reduced signs of aging in epidemiological studies. A cross-sectional study of over 4,000 women aged 40 to 74 found that higher vitamin C intake was associated with significantly lower odds of a wrinkled appearance and age-related skin dryness.
- Elastin Synthesis – Beyond collagen, vitamin C also supports the synthesis of elastin, the protein responsible for skin elasticity and the ability to return to its original shape after stretching.
Wound Healing Phases
Vitamin C participates in all phases of wound repair, reflecting the central role of collagen in tissue reconstruction.
- Inflammatory Phase (Days 1-5) – Vitamin C supports neutrophil and macrophage function at the wound site, facilitating debris clearance and pathogen defense. Ascorbate modulates inflammatory cytokine production to prevent excessive tissue damage.
- Proliferative Phase (Days 5-21) – This phase demands massive collagen synthesis by fibroblasts to form granulation tissue. Vitamin C is consumed at high rates as prolyl and lysyl hydroxylases work to produce mature collagen. Ascorbate also supports angiogenesis (new blood vessel formation) by promoting endothelial cell proliferation and stabilizing newly formed capillaries through basement membrane collagen (type IV) synthesis.
- Remodeling Phase (3 weeks to 1 year) – Type III collagen deposited during the proliferative phase is gradually replaced by stronger type I collagen. This remodeling requires continued vitamin C-dependent hydroxylation and cross-linking. Healed wounds ultimately achieve 70 to 80% of the tensile strength of uninjured tissue.
Joint and Cartilage Support
- Articular Cartilage – Articular cartilage relies on type II collagen for its structural framework. Chondrocytes embedded within the cartilage matrix require vitamin C to synthesize and maintain this collagen network. The Framingham Osteoarthritis Cohort Study found that higher vitamin C intake (middle and highest tertiles) reduced the risk of osteoarthritis progression threefold and decreased the risk of knee pain.
- Proteoglycan Synthesis – In addition to collagen, vitamin C supports the synthesis of proteoglycans (aggrecan), which provide cartilage with its compressive resilience and water-retaining properties.
- Meniscus and Ligament Repair – Tendons and ligaments are composed primarily of type I collagen. Adequate vitamin C status is important for the repair of sports injuries and the recovery of joint stability after ligament damage.
Blood Vessel Integrity
- Vascular Collagen – Blood vessel walls contain abundant collagen (types I, III, and IV) that provides structural strength and prevents rupture under arterial pressure. Vitamin C deficiency weakens vessel walls, leading to the spontaneous hemorrhages characteristic of scurvy.
- Endothelial Basement Membrane – The endothelium rests on a basement membrane rich in type IV collagen. Vitamin C supports the integrity of this barrier, which controls the passage of molecules and cells between the blood and surrounding tissue.
- Atherosclerosis Connection – Some researchers have proposed that suboptimal vitamin C status contributes to vascular weakening that the body attempts to repair with lipoprotein(a) deposition, potentially contributing to atherosclerotic plaque formation. While this hypothesis remains debated, adequate vitamin C clearly supports vascular collagen maintenance.
Bone Collagen Matrix
- Organic Matrix – Approximately 90% of the organic matrix of bone is type I collagen. This collagen scaffold provides the template upon which hydroxyapatite crystals are deposited during mineralization. Without proper collagen formation, bone mineralization cannot proceed normally.
- Osteoblast Function – Osteoblasts, the bone-forming cells, are prolific collagen producers. Vitamin C stimulates osteoblast differentiation, proliferation, and collagen synthesis. In cell culture, ascorbate is an essential component of osteogenic differentiation media.
- Fracture Risk – Epidemiological studies link higher vitamin C intake with greater bone mineral density and reduced fracture risk, particularly in postmenopausal women and elderly men.
Periodontal Health
- Periodontal Ligament – The periodontal ligament anchoring teeth to the alveolar bone is composed primarily of collagen fibers. Vitamin C deficiency leads to weakening of this ligament, resulting in tooth loosening and eventual loss, one of the hallmark symptoms of scurvy.
- Gingival Health – Gingival tissue has a high collagen turnover rate and is particularly sensitive to vitamin C status. Supplementation in individuals with marginal vitamin C status has been shown to reduce gingival bleeding and improve periodontal probe depths.
- Epidemiological Evidence – The third National Health and Nutrition Examination Survey (NHANES III) found a significant association between low vitamin C intake and periodontal disease prevalence, even after controlling for smoking status.
Surgical Recovery
- Preoperative Optimization – Surgeons increasingly recognize the importance of vitamin C status for postoperative wound healing. Plasma vitamin C levels drop significantly after major surgery due to increased metabolic demand and the acute-phase response. Preoperative supplementation (500 mg to 1 g daily for 1 to 2 weeks) has been recommended by some surgical nutrition guidelines.
- Postoperative Supplementation – Several studies have demonstrated faster wound healing, reduced wound dehiscence, and lower infection rates with postoperative vitamin C supplementation, particularly in patients undergoing orthopedic, colorectal, or plastic surgery.
- Complex Regional Pain Syndrome (CRPS) – A meta-analysis of randomized trials found that vitamin C supplementation (500 mg daily for 50 days) following wrist fracture surgery reduced the incidence of CRPS by approximately 50%.
Topical Vitamin C for Skin
- L-Ascorbic Acid – The most studied topical form, L-ascorbic acid at concentrations of 10 to 20% and pH below 3.5 has been shown to penetrate the stratum corneum and increase dermal collagen synthesis. Clinical trials demonstrate improvements in fine lines, skin texture, and photoaged skin with consistent use over 12 weeks or more.
- Stable Derivatives – Because L-ascorbic acid is unstable and rapidly oxidizes, numerous derivatives have been developed, including ascorbyl palmitate, magnesium ascorbyl phosphate, and ascorbic acid 2-glucoside (AA2G). These offer improved stability but variable bioconversion to active ascorbic acid within the skin.
- Combination Formulations – The combination of topical vitamin C with vitamin E and ferulic acid (the “CEF” formulation) has been shown to provide enhanced photoprotection and collagen-stimulating effects, with synergistic antioxidant activity exceeding the sum of individual components.
- Melanin Inhibition – Topical vitamin C also inhibits tyrosinase, the rate-limiting enzyme in melanin production, making it useful for hyperpigmentation and uneven skin tone in addition to its collagen-promoting effects.
Clinical Applications and Recommendations
- Dietary Intake – The RDA of 75 to 90 mg daily prevents scurvy but may not optimize collagen synthesis. Many researchers recommend 200 to 500 mg daily for maximal connective tissue support, achievable through a diet rich in fruits and vegetables supplemented as needed.
- Collagen Supplements – The growing market for oral collagen supplements (hydrolyzed collagen peptides) should be considered alongside vitamin C status. Taking collagen peptides without adequate vitamin C is unlikely to maximize benefit, as the body requires ascorbate to incorporate the amino acids into new collagen molecules.
- Special Populations – Athletes, surgical patients, individuals with chronic wounds, smokers, and those with connective tissue disorders may benefit from higher vitamin C intakes to support increased collagen demands.
This content is provided for informational purposes only and does not constitute medical advice. Consult a qualified healthcare provider before beginning any supplementation regimen, particularly in the perioperative setting or if you have a connective tissue disorder.
Research Papers and References
The following are landmark and frequently cited research papers underpinning the claims on this page. Links resolve to the publisher DOI or PubMed record.
Pharmacokinetics and Foundational Biochemistry
- Levine M, Conry-Cantilena C, Wang Y, et al. Vitamin C pharmacokinetics in healthy volunteers: evidence for a recommended dietary allowance. PNAS. 1996;93(8):3704-3709.
- Padayatty SJ, Sun H, Wang Y, et al. Vitamin C pharmacokinetics: implications for oral and intravenous use. Annals of Internal Medicine. 2004;140(7):533-537.
Skin, Collagen, and Wound Healing
- Pullar JM, Carr AC, Vissers MCM. The roles of vitamin C in skin health. Nutrients. 2017;9(8):866.
- DePhillipo NN, Aman ZS, Kennedy MI, et al. Efficacy of vitamin C supplementation on collagen synthesis and oxidative stress after musculoskeletal injuries: a systematic review. Orthopaedic Journal of Sports Medicine. 2018;6(10):2325967118804544.
- PubMed — Vitamin C, wound healing, and fibroblast collagen synthesis (topic search)
Bone, Cartilage, and Connective Tissue
- PubMed — Vitamin C and bone mineral density (topic search)
- PubMed — Vitamin C and osteoarthritis progression in the Framingham cohort (topic search)
- PubMed — Ascorbate and cartilage proteoglycan synthesis (topic search)
Perioperative and CRPS Evidence
- PubMed — Vitamin C and CRPS after distal radius fracture: meta-analyses (topic search)
- PubMed — Perioperative vitamin C and wound healing RCTs (topic search)
Skin Aging — Epidemiology and Topical
- PubMed — Dietary vitamin C and skin-aging appearance (topic search)
- PubMed — Topical L-ascorbic acid, vitamin E, and ferulic acid (topic search)
External Authoritative Resources
- NIH Office of Dietary Supplements — Vitamin C Fact Sheet for Health Professionals
- Linus Pauling Institute — Micronutrient Information Center: Vitamin C
- Harvard T.H. Chan School of Public Health — The Nutrition Source: Vitamin C
- PubMed — Vitamin C and collagen synthesis reviews (topic search)
Connections
- All Vitamins
- Vitamin C, Collagen & Why Sailors Fell Apart — interactive animation
- Vitamin C
- Collagen
- Iron
- Vitamin C and Iron Absorption
- Vitamin C and Immune Defense
- Vitamin E
- Vitamin A
- Vitamin D3
- Zinc
- Copper
- Vitamin K
- Osteoporosis
- Proline
- Lysine
- Vitamin E and Skin Health