Acne
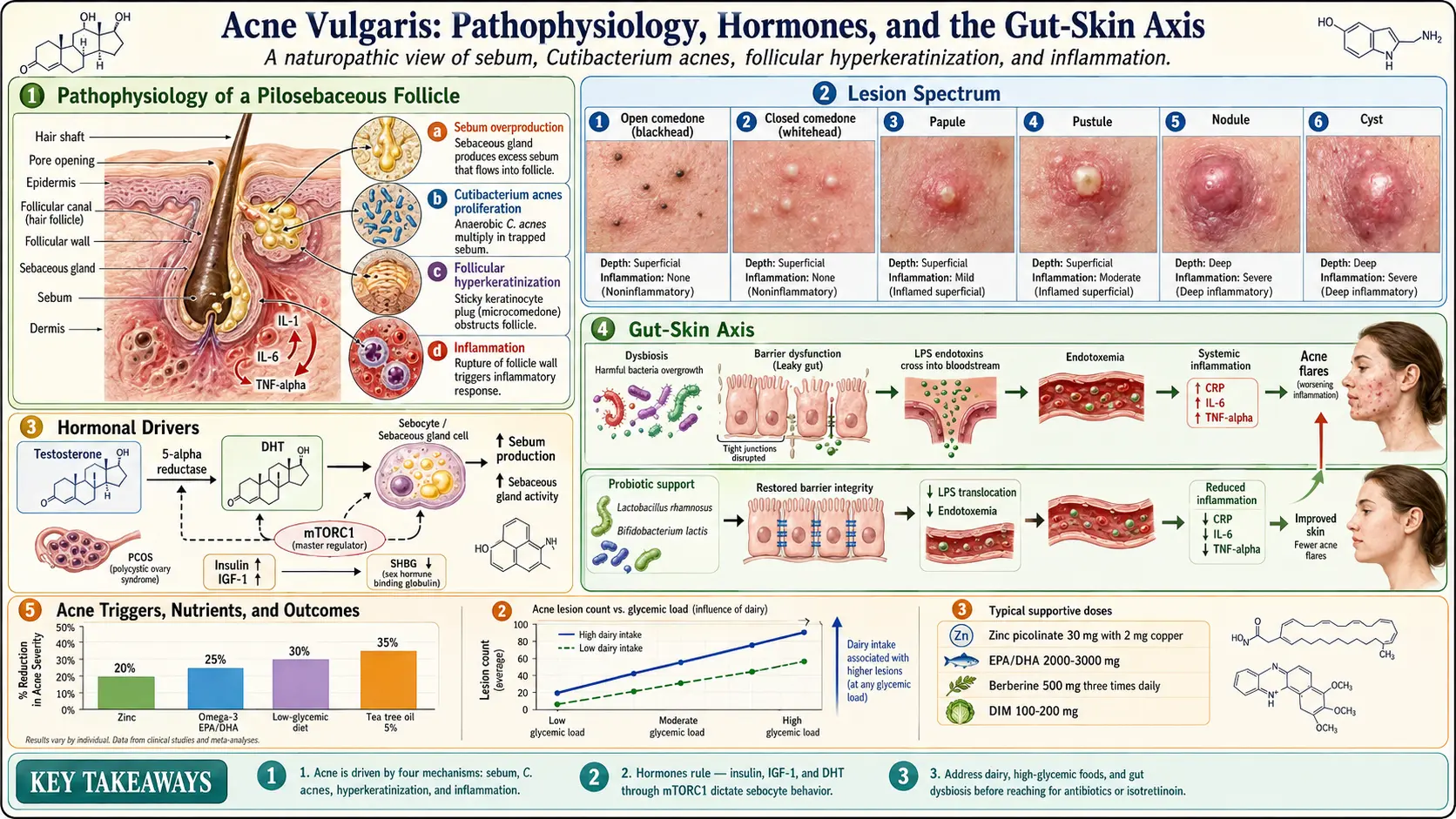
Table of Contents
- What Is Acne?
- Pathophysiology of Acne
- Types of Acne
- Hormonal Drivers
- The Gut-Skin Axis
- Conventional Treatments
- Natural and Naturopathic Approaches
- Dietary Triggers
- Blood Sugar and Insulin Connection
- Stress and Cortisol's Role
- Skincare Routine Recommendations
- Cautions and Considerations
- References & Research
- Featured Videos
What Is Acne?
Acne vulgaris is the most common skin condition worldwide, affecting an estimated 85% of people between the ages of 12 and 24. While often considered a teenage problem, acne can persist well into adulthood or appear for the first time in the 20s, 30s, or even 40s. From a naturopathic perspective, acne is not simply a skin problem but a visible manifestation of internal imbalances involving hormones, digestion, inflammation, and nutrient status.
Acne presents in several forms, ranging from mild to severe:
- Comedones — The most basic acne lesion. Open comedones (blackheads) occur when a pore is clogged but remains open at the surface, allowing the contents to oxidize and darken. Closed comedones (whiteheads) are pores sealed over by skin, trapping sebum and dead cells beneath the surface.
- Papules — Small, raised, red bumps caused by inflammation of clogged pores. They are tender to the touch and do not contain visible pus.
- Pustules — Similar to papules but topped with white or yellow pus. These are the classic "pimples" most people recognize.
- Nodules — Large, hard, painful lumps that form deep within the skin. They result from severe inflammation and can persist for weeks.
- Cysts — The most severe form of acne. Cysts are deep, pus-filled lesions that are painful and carry a high risk of scarring. They often require professional treatment.
Pathophysiology of Acne
Understanding how acne develops is essential for effective treatment. Four primary mechanisms work together to create acne lesions:
1. Sebum Overproduction
The sebaceous glands produce an oily substance called sebum, which normally lubricates the skin and hair. When these glands become overactive, often due to hormonal stimulation, excess sebum accumulates in the pore and creates an environment conducive to bacterial growth. Androgens, particularly dihydrotestosterone (DHT), are the primary hormonal drivers of increased sebum production.
2. Propionibacterium acnes (P. acnes) Bacteria
Cutibacterium acnes (formerly Propionibacterium acnes) is a commensal bacterium that lives on human skin. In normal amounts, it is harmless. However, when trapped inside a clogged pore with excess sebum, P. acnes proliferates rapidly. The bacterium produces enzymes and pro-inflammatory molecules that irritate the follicular wall and trigger an immune response, leading to the redness, swelling, and pus formation characteristic of inflammatory acne.
3. Follicular Hyperkeratinization
Normally, dead skin cells lining the hair follicle shed and are carried to the surface by sebum flow. In acne-prone skin, these cells become sticky and accumulate inside the follicle, forming a plug called a microcomedone. This process, known as follicular hyperkeratinization, is the initial event that leads to all visible acne lesions. Factors that promote hyperkeratinization include androgen activity, low levels of linoleic acid in sebum, and certain inflammatory cytokines.
4. Inflammation
Modern research has established that inflammation is present even in the earliest stages of acne, not just in visibly inflamed lesions. Pro-inflammatory cytokines such as IL-1, IL-6, and TNF-alpha are elevated in acne-affected skin. This chronic low-grade inflammation contributes to the progression from comedones to papules, pustules, and deeper lesions. Addressing systemic inflammation is a cornerstone of the naturopathic approach to acne.
Types of Acne
Hormonal Acne
Hormonal acne is driven by fluctuations in sex hormones, particularly androgens. It is most common in women and often appears along the jawline, chin, and lower cheeks. Hormonal acne frequently flares in the week before menstruation, during perimenopause, or in conditions such as polycystic ovary syndrome (PCOS). In men, hormonal acne may appear on the back and chest as well as the face.
- Tends to be deep, cystic, and painful
- Cyclical pattern related to menstrual cycle
- Often resistant to topical-only treatments
- May be accompanied by other signs of androgen excess such as hirsutism or hair thinning
Cystic Acne
Cystic acne is the most severe form of acne and involves large, inflamed, pus-filled cysts deep beneath the skin surface. These lesions are painful, slow to resolve, and frequently lead to scarring. Cystic acne often has a strong hormonal and genetic component. It may require a multi-pronged treatment approach addressing internal drivers rather than relying solely on topical products.
Fungal Acne (Malassezia Folliculitis)
Fungal acne is not true acne but is often mistaken for it. It is caused by an overgrowth of Malassezia yeast in the hair follicles, leading to small, uniform, itchy bumps typically found on the chest, back, and forehead. Unlike bacterial acne, fungal acne does not respond to antibiotics and may actually worsen with their use. Key distinguishing features include:
- Uniform size of bumps (unlike true acne, which has varied lesion types)
- Itchiness as a prominent symptom
- Worsens with sweat, humidity, and occlusive skincare products
- Requires antifungal treatment rather than antibacterial approaches
Hormonal Drivers
Hormones are the single most influential factor in acne development. Understanding the hormonal landscape is critical for effective treatment, especially in adult acne.
Androgens and DHT
Androgens — including testosterone, DHEA-S, and dihydrotestosterone (DHT) — stimulate the sebaceous glands to produce more sebum. The enzyme 5-alpha reductase converts testosterone to DHT, which is significantly more potent at stimulating sebum production. Some individuals have higher 5-alpha reductase activity in their skin, making them more acne-prone even with normal blood androgen levels.
Insulin as an Androgen Driver
Insulin and insulin-like growth factor 1 (IGF-1) play a major role in acne pathogenesis. Elevated insulin increases androgen production by the ovaries and adrenal glands, reduces sex hormone-binding globulin (SHBG), and directly stimulates sebocyte proliferation. This mechanism explains why high-glycemic diets and insulin resistance are strongly associated with acne.
The PCOS Connection
Polycystic ovary syndrome (PCOS) is one of the most common hormonal disorders in women of reproductive age and is frequently associated with persistent acne. Women with PCOS often exhibit elevated androgens, insulin resistance, and chronic low-grade inflammation — a triad that creates ideal conditions for acne. Addressing PCOS through blood sugar management, anti-inflammatory nutrition, and hormone-balancing strategies often leads to significant improvement in acne as well.
Estrogen and Progesterone
Estrogen generally has a protective effect against acne by opposing androgen activity and reducing sebum production. Progesterone, however, can be converted to androgens and may contribute to premenstrual acne flares. Low progesterone relative to estrogen (luteal phase deficiency) may also play a role in cyclical breakouts.
The Gut-Skin Axis
The connection between gut health and skin health is one of the most important and often overlooked aspects of acne treatment. Naturopathic medicine has long recognized this relationship, and modern research increasingly supports the existence of a gut-skin axis.
How the Gut Affects the Skin
- Intestinal permeability (leaky gut) — When the gut lining becomes compromised, bacterial endotoxins (lipopolysaccharides) can enter the bloodstream and trigger systemic inflammation that manifests in the skin.
- Dysbiosis — An imbalance in the gut microbiome can increase systemic inflammation, impair nutrient absorption, and alter hormone metabolism, all of which influence acne.
- Impaired detoxification — The gut is a primary route of elimination. When bowel function is sluggish or the microbiome is disrupted, the body may attempt to eliminate toxins through the skin.
- SIBO connection — Small intestinal bacterial overgrowth (SIBO) has been found to be significantly more prevalent in acne patients than in controls. SIBO contributes to nutrient malabsorption, inflammation, and intestinal permeability.
Probiotics for Acne
Both oral and topical probiotics have shown promise in acne treatment. Specific strains including Lactobacillus rhamnosus, Lactobacillus acidophilus, and Bifidobacterium lactis have demonstrated the ability to reduce inflammatory markers, improve gut barrier integrity, and decrease acne severity in clinical studies.
Conventional Treatments
Understanding conventional acne treatments helps patients make informed decisions. Each approach has benefits and limitations that should be carefully considered.
Benzoyl Peroxide
An antibacterial agent that kills P. acnes bacteria and helps prevent resistance. Available over the counter in strengths from 2.5% to 10%. Effective for mild to moderate acne but can cause dryness, peeling, and irritation. Lower concentrations (2.5%) are often equally effective with fewer side effects.
Retinoids (Topical)
Vitamin A derivatives such as tretinoin, adapalene, and tazarotene work by normalizing follicular keratinization and reducing comedone formation. They are considered a first-line treatment for comedonal acne. Side effects include dryness, peeling, sun sensitivity, and an initial "purging" period where acne may temporarily worsen.
Antibiotics
Both topical (clindamycin, erythromycin) and oral antibiotics (doxycycline, minocycline) are commonly prescribed for inflammatory acne. While effective short-term, significant concerns include:
- Antibiotic resistance (a growing global health concern)
- Disruption of the gut microbiome
- Rebound acne upon discontinuation
- Side effects including GI upset, photosensitivity, and yeast infections
Accutane (Isotretinoin)
Isotretinoin is a systemic retinoid reserved for severe, treatment-resistant acne. It works by dramatically reducing sebum production, shrinking sebaceous glands, and normalizing keratinization. While highly effective, it carries significant risks:
- Teratogenicity — Causes severe birth defects and is absolutely contraindicated in pregnancy
- Liver toxicity — Requires regular liver function monitoring
- Lipid changes — Can elevate triglycerides and cholesterol
- Dryness — Severe dryness of skin, lips, eyes, and mucous membranes
- Mood changes — Reports of depression, anxiety, and in rare cases suicidal ideation, though causation remains debated
- Musculoskeletal effects — Joint pain, muscle aches, and in rare cases impacts on bone growth in adolescents
- Gut effects — May alter the gut microbiome and has been associated with inflammatory bowel disease in some studies
Natural and Naturopathic Approaches
A naturopathic approach to acne focuses on identifying and addressing root causes rather than suppressing symptoms. The following nutrients and botanical medicines have evidence supporting their use in acne management.
Zinc
Zinc is one of the most well-studied nutrients for acne. It reduces inflammation, inhibits P. acnes growth, reduces 5-alpha reductase activity (lowering DHT), and supports wound healing. Studies have shown that oral zinc supplementation can reduce acne severity by up to 50%. Zinc picolinate or zinc bisglycinate at 30 mg daily are well-absorbed forms. Always take zinc with food and balance with copper (2 mg copper per 30 mg zinc) to prevent deficiency.
Vitamin A
Vitamin A (retinol, not beta-carotene) supports healthy skin cell turnover and immune function. Low vitamin A status is associated with increased acne severity. Moderate supplementation (5,000-10,000 IU daily) can support skin health. Higher therapeutic doses should be supervised by a healthcare provider, and vitamin A is contraindicated in pregnancy at doses above 10,000 IU.
Omega-3 Fatty Acids
EPA and DHA from fish oil or algal sources have potent anti-inflammatory effects. They reduce pro-inflammatory prostaglandins and leukotrienes that drive acne inflammation. Studies have shown improvement in acne severity with supplementation of 2,000-3,000 mg of combined EPA/DHA daily. Omega-3s also help balance the omega-6 to omega-3 ratio, which is typically skewed toward pro-inflammatory omega-6 in modern diets.
Probiotics
As discussed in the gut-skin axis section, probiotics support a healthy microbiome, reduce systemic inflammation, and improve gut barrier integrity. A multi-strain probiotic containing Lactobacillus and Bifidobacterium species at a dose of 10-50 billion CFU daily is a reasonable starting point.
DIM (Diindolylmethane)
DIM is a compound derived from cruciferous vegetables that supports healthy estrogen metabolism. It promotes the conversion of estrogen to less proliferative metabolites (2-hydroxyestrone) and may help reduce androgen activity. DIM at 100-200 mg daily is commonly used for hormonal acne, particularly in women with signs of estrogen dominance or PCOS.
Berberine
Berberine is a plant alkaloid found in goldenseal, Oregon grape, and barberry. It has antimicrobial, anti-inflammatory, and insulin-sensitizing properties. Berberine has been shown to be as effective as metformin in improving insulin sensitivity, making it particularly useful for acne associated with insulin resistance or PCOS. Typical dosing is 500 mg two to three times daily with meals.
Tea Tree Oil (Topical)
Tea tree oil (Melaleuca alternifolia) has well-documented antibacterial and anti-inflammatory properties. A 5% tea tree oil gel has been shown to be as effective as 5% benzoyl peroxide for mild to moderate acne, with fewer side effects. It should always be diluted before application and should never be ingested.
Green Tea
Green tea contains epigallocatechin gallate (EGCG), a polyphenol with anti-inflammatory, antioxidant, and anti-androgenic properties. Both oral consumption and topical application of green tea extract have shown benefit in reducing sebum production and acne lesion counts. Drinking 3-4 cups of green tea daily or applying a 2-3% green tea extract topically can be part of an integrative acne protocol.
Dietary Triggers
Diet plays a significant role in acne development and severity. The following dietary factors have the strongest evidence linking them to acne.
Dairy
Dairy products, particularly skim milk, have been consistently associated with increased acne risk in large epidemiological studies. The mechanisms likely involve:
- Naturally occurring hormones in milk (estrogen, progesterone, androgens, IGF-1)
- Insulinotropic properties — dairy raises insulin levels disproportionately to its glycemic index
- Casein and whey proteins stimulate IGF-1 production
- Bioactive peptides that may influence androgen pathways
A 2-3 month trial of complete dairy elimination is often recommended to assess individual sensitivity.
Sugar and High-Glycemic Foods
High-glycemic foods — white bread, white rice, sugary drinks, candy, processed cereals — cause rapid spikes in blood glucose and insulin. Elevated insulin increases androgen production, reduces SHBG, and directly stimulates sebocyte activity. Multiple studies have demonstrated that a low-glycemic diet significantly reduces acne lesion counts and severity.
Whey Protein
Whey protein supplements are a particularly potent acne trigger. Whey is highly insulinotropic and contains branched-chain amino acids (especially leucine) that activate the mTORC1 pathway, a master regulator of cell growth that drives sebum production and follicular keratinization. Bodybuilders and athletes frequently report acne outbreaks that correlate with whey protein use.
Other Potential Triggers
- Chocolate — Some studies suggest cocoa itself may increase inflammatory acne, independent of sugar content
- Processed and fried foods — High in omega-6 fatty acids and advanced glycation end products (AGEs) that promote inflammation
- Alcohol — Increases inflammation, disrupts gut health, and impairs liver detoxification
Blood Sugar and Insulin Connection
The relationship between blood sugar regulation and acne cannot be overstated. Insulin resistance is increasingly recognized as a central driver of acne, particularly in adults.
How Insulin Drives Acne
- Increases androgen production — Insulin stimulates the ovaries and adrenal glands to produce more testosterone and DHEA-S
- Reduces SHBG — Lower SHBG means more free (active) testosterone circulating in the body
- Elevates IGF-1 — IGF-1 stimulates sebocyte proliferation, sebum production, and follicular keratinization
- Activates mTORC1 — This nutrient-sensing pathway promotes cell growth and sebum synthesis and is now considered a central mediator of acne pathogenesis
- Promotes inflammation — Chronic hyperinsulinemia drives a pro-inflammatory state
Blood Sugar Management Strategies
- Eat a low-glycemic, whole-foods diet rich in vegetables, quality proteins, and healthy fats
- Include protein, fat, and fiber at every meal to slow glucose absorption
- Avoid refined carbohydrates, sugary drinks, and processed snacks
- Consider berberine (500 mg 2-3 times daily) or chromium (200-400 mcg daily) for additional insulin-sensitizing support
- Regular exercise improves insulin sensitivity significantly
- Adequate sleep (7-9 hours) is essential for blood sugar regulation
Stress and Cortisol's Role
Stress is a well-established acne trigger that operates through multiple mechanisms. The relationship between stress and acne is bidirectional — stress worsens acne, and acne itself is a significant source of psychological stress.
Mechanisms of Stress-Induced Acne
- Cortisol elevation — Chronic stress raises cortisol, which increases blood sugar, promotes insulin resistance, and stimulates sebum production. Sebocytes have cortisol receptors and respond directly to stress hormones.
- Adrenal androgen production — Stress activates the hypothalamic-pituitary-adrenal (HPA) axis, increasing adrenal androgen output (DHEA-S), which can drive acne.
- Immune dysregulation — Chronic stress suppresses some immune functions while amplifying inflammatory pathways, creating conditions favorable for acne.
- Gut disruption — Stress alters gut motility, microbiome composition, and intestinal permeability, all of which affect the gut-skin axis.
- Neuropeptides — Stress triggers the release of substance P and other neuropeptides in the skin that directly promote inflammation and sebum production.
Stress Management Approaches
- Regular mindfulness meditation or deep breathing exercises
- Adaptogenic herbs such as ashwagandha, rhodiola, and holy basil to support the stress response
- Consistent exercise (but avoid over-exercising, which can increase cortisol)
- Prioritizing sleep quality and consistency
- Reducing caffeine intake, which stimulates cortisol release
- Building social connection and seeking support when needed
Skincare Routine Recommendations
While addressing internal factors is paramount, a thoughtful skincare routine supports the skin's barrier function and can prevent further irritation.
Core Principles
- Gentle cleansing — Use a mild, pH-balanced cleanser (pH 4.5-5.5) twice daily. Avoid harsh scrubs, abrasive exfoliants, and strong sulfate-based cleansers that strip the skin barrier.
- Non-comedogenic products — Choose moisturizers, sunscreens, and makeup labeled non-comedogenic. Common pore-clogging ingredients to avoid include coconut oil, isopropyl myristate, and certain silicones.
- Moisturize appropriately — Even oily, acne-prone skin needs moisture. Lightweight, oil-free moisturizers with ingredients like hyaluronic acid, niacinamide, or aloe vera support skin barrier repair without clogging pores.
- Sun protection — Use mineral-based sunscreens (zinc oxide, titanium dioxide) rather than chemical sunscreens, which can be irritating. Many acne treatments increase photosensitivity.
- Avoid over-treatment — Using too many active products simultaneously (retinoids, acids, benzoyl peroxide) can compromise the skin barrier and worsen acne. Introduce one active at a time.
- Do not pick or squeeze — Manipulating acne lesions increases inflammation, spreads bacteria, and significantly increases scarring risk.
Helpful Topical Ingredients
- Niacinamide (vitamin B3) — Reduces inflammation, regulates sebum, and improves skin barrier function
- Tea tree oil (5%) — Antimicrobial and anti-inflammatory
- Green tea extract — Antioxidant and anti-androgenic
- Azelaic acid (10-20%) — Antibacterial, anti-inflammatory, and reduces hyperpigmentation
- Salicylic acid (0.5-2%) — A beta-hydroxy acid that penetrates pores and dissolves comedonal plugs
Cautions and Considerations
- Severe cystic acne may require co-management with a dermatologist. Natural approaches work best as part of an integrative plan.
- Acne scarring risk is highest with deep, inflamed lesions. Prompt treatment of severe acne is important to minimize permanent scarring.
- Supplement interactions — Berberine may interact with certain medications, including statins and diabetes drugs. Zinc can interfere with copper and iron absorption. Always consult a knowledgeable provider before starting new supplements.
- Hormonal testing — For suspected hormonal acne, comprehensive testing including testosterone, free testosterone, DHEA-S, SHBG, fasting insulin, and glucose is recommended to guide treatment.
- Purging vs. breakouts — Some treatments (retinoids, certain natural approaches) may cause an initial "purge" as existing microcomedones are brought to the surface. This typically resolves within 4-6 weeks. True worsening beyond this period suggests the treatment is not appropriate.
- Patience is essential — Skin cell turnover takes approximately 28 days. Most natural acne protocols require 8-12 weeks to show significant results. Consistency is key.
- Pregnancy considerations — Retinoids (both topical and oral), high-dose vitamin A, and certain herbs are contraindicated in pregnancy. Always verify supplement safety during pregnancy and breastfeeding.
13. References & Research
Historical Background
Acne vulgaris has been recognized since antiquity, with ancient Egyptian and Greek physicians documenting skin eruptions. The modern understanding of acne pathophysiology began with Robert Willan and Thomas Bateman's dermatological classifications in the early 19th century. In 1931, Felix Grutz established the link between lipid metabolism and acne, and the bacterium Propionibacterium acnes (now Cutibacterium acnes) was identified as a key contributor by Douglas Geraint James and colleagues in the mid-20th century.
Key Research Papers
- Zaenglein AL, Pathy AL, Schlosser BJ, et al. Guidelines of care for the management of acne vulgaris. J Am Acad Dermatol. 2016;74(5):945-973.e33.
- Williams HC, Dellavalle RP, Garner S. Acne vulgaris. Lancet. 2012;379(9813):361-372.
- Dréno B, Pécastaings S, Corvec S, et al. Cutibacterium acnes (Propionibacterium acnes) and acne vulgaris: a brief look at the latest updates. J Eur Acad Dermatol Venereol. 2018;32(S2):5-14.
- Melnik BC. Acne vulgaris: the metabolic syndrome of the pilosebaceous follicle. Dermatoendocrinol. 2018;10(1):e1232027.
- Adebamowo CA, Spiegelman D, Danby FW, et al. High school dietary dairy intake and teenage acne. J Am Acad Dermatol. 2005;52(2):207-214.
- Smith RN, Mann NJ, Braue A, et al. A low-glycemic-load diet improves symptoms in acne vulgaris patients: a randomized controlled trial. Am J Clin Nutr. 2007;86(1):107-115.
- Bowe WP, Logan AC. Acne vulgaris, probiotics and the gut-brain-skin axis: back to the future? Gut Pathog. 2011;3(1):1.
- Dreno B, Moyse D, Alirezai M, et al. Multicenter randomized comparative double-blind controlled clinical trial of the safety and efficacy of zinc gluconate versus minocycline hydrochloride in the treatment of inflammatory acne vulgaris. Dermatology. 2001;203(2):135-140.
- Melnik BC, Schmitz G. Role of insulin, insulin-like growth factor-1, hyperglycaemic food and milk consumption in the pathogenesis of acne vulgaris. Exp Dermatol. 2009;18(10):833-841.
- Leyden JJ. A review of the use of combination therapies for the treatment of acne vulgaris. J Am Acad Dermatol. 2003;49(3 Suppl):S200-S210.
- Bhate K, Williams HC. Epidemiology of acne vulgaris. Br J Dermatol. 2013;168(3):474-485.
- Keri J, Shiman M. An update on the management of acne vulgaris. Clin Cosmet Investig Dermatol. 2009;2:105-110.
Research Papers
Curated PubMed topic searches of peer-reviewed literature on Acne Vulgaris. Each link opens a live PubMed query so you always see the most current studies.
- PubMed: Acne pathogenesis
- PubMed: Acne treatment guidelines
- PubMed: Isotretinoin outcomes
- PubMed: Topical retinoids
- PubMed: Benzoyl peroxide
- PubMed: Antibiotic resistance in acne
- PubMed: Hormonal and spironolactone therapy
- PubMed: Diet and acne
- PubMed: Gut-skin axis in acne
- PubMed: Acne and PCOS
- PubMed: Light and laser therapy
- PubMed: Acne scarring treatment
Connections
- Dermatology
- Zinc
- Vitamin A
- Tea Tree
- Eczema
- Psoriasis
- Rosacea
- Gut Healing
- Elimination Diet
- Gut-Brain Axis
- Blood Sugar
- PCOS
- Testosterone
- Green Tea
- Insulin Resistance
- Probiotics
- Berberine
- DHEA-S
- Omega-3 Fatty Acids