Hypophosphatemia (Low Phosphate): Fatigue
When phosphate runs low, the tiredness it produces is unlike a bad night's sleep — it is a bone-deep, whole-body flatness, as if your batteries can no longer hold a charge. This makes biological sense, because phosphate sits at the very center of how your cells make energy: it is the P in ATP (adenosine triphosphate), the molecule that powers almost everything your body does. This page explains why low phosphate specifically drains energy, why it is easy to mistake the fatigue for a dozen more common things, when tiredness should prompt a phosphate check, and how the level is restored safely. It covers one symptom only — the fatigue of low phosphate — and links to its siblings (muscle weakness, bone pain) rather than repeating them.
Table of Contents
- What the Fatigue of Low Phosphate Feels Like
- The Mechanism: Phosphate Is the “P” in ATP
- A Second Hit: Phosphate, 2,3-DPG, and Oxygen Delivery
- Honesty: Fatigue Has Many Causes
- Clues That Point Toward Low Phosphate
- Common Situations That Cause It
- Getting Tested
- Correcting Low Phosphate Safely
- When to Seek Care / Red Flags
- Key Research Papers
- Connections
- Featured Videos
What the Fatigue of Low Phosphate Feels Like
The tiredness of low phosphate is usually described as energy that simply isn't there, rather than sleepiness. People say they wake unrefreshed, run out of steam early in the day, and find that ordinary tasks — making a meal, walking to the mailbox, getting through a workday — cost far more than they should. It is a fatigue that rest doesn't fix, because the problem is not a lack of sleep but a shortfall in the cellular fuel that converts effort into action.
Common everyday descriptions include:
- “Flat” or “drained” from the moment you wake — the sense that you started the day already depleted.
- Effort feels disproportionate — light activity leaves you needing to sit down, and you pace yourself through tasks you used to do without thinking.
- Mental fog alongside the physical tiredness — difficulty concentrating, slowed thinking, and irritability. The brain is one of the body's most energy-hungry organs, so it feels a fuel shortage too.
- A “heavy” whole-body feeling — though here it is important to separate genuine weakness (the muscle can't generate force) from fatigue (you have the strength but no stamina or drive). Severe low phosphate can cause both; the loss of strength is covered on the sibling muscle weakness page.
One reason this fatigue is under-recognized is that mild and even moderate hypophosphatemia is often vague and non-specific. There is rarely a single dramatic symptom; instead there is a creeping loss of vitality that people attribute to age, stress, overwork, or simply “getting older.” The fatigue tends to track how low and how fast the phosphate has fallen — a level that drops quickly (as in refeeding) can cause marked symptoms, while a chronically low-normal level may be quietly tolerated.
The Mechanism: Phosphate Is the “P” in ATP
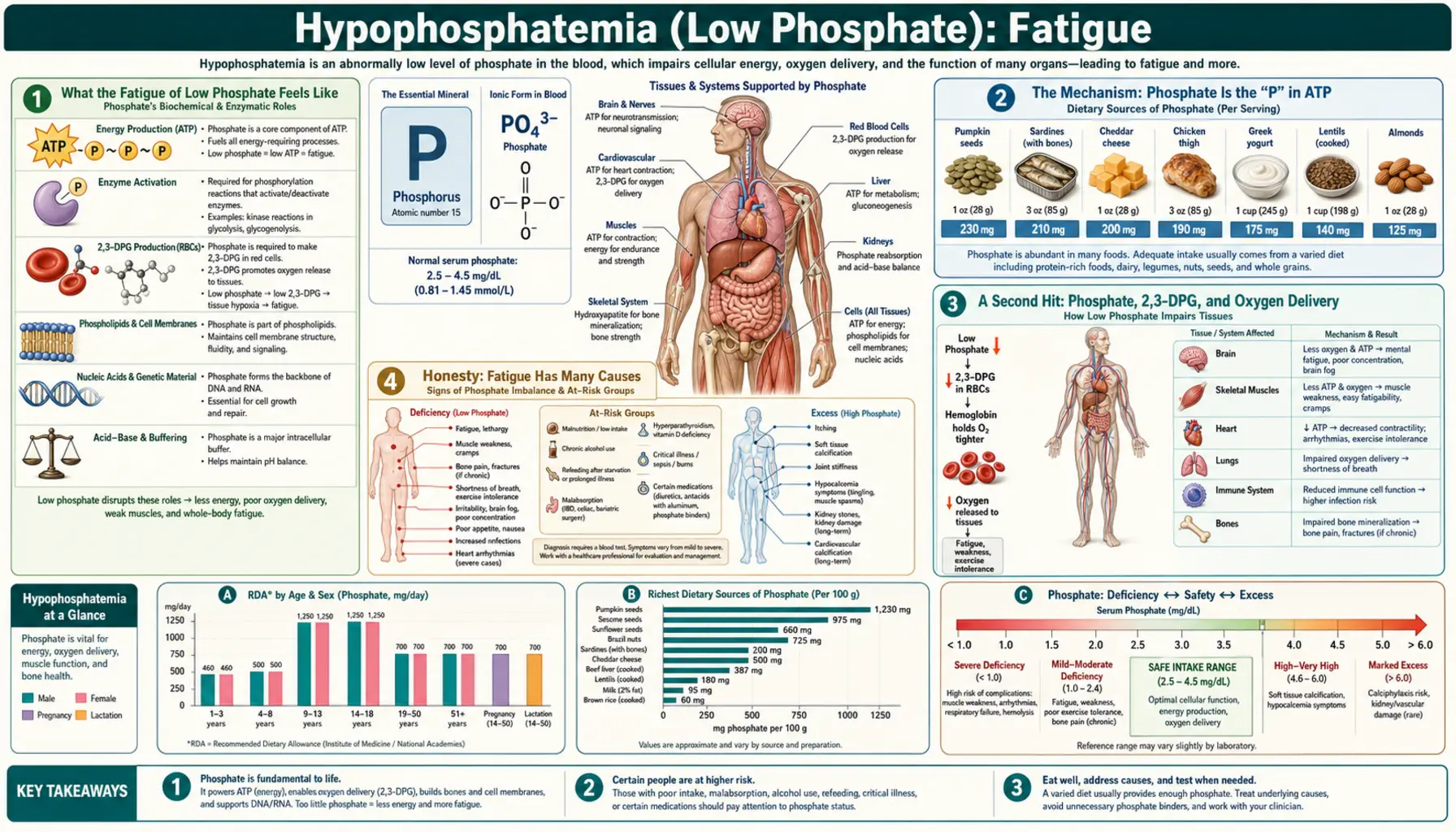
To understand why low phosphate drains energy, you have to meet the molecule your cells use as currency: adenosine triphosphate, or ATP. Nearly every energy-requiring process in the body — a muscle contracting, a nerve firing, a kidney pumping salt, a cell building protein — is paid for by splitting off one of ATP's phosphate groups, which releases usable energy and leaves behind ADP (adenosine diphosphate). The cell then spends fuel from food and oxygen to reattach a phosphate and recharge ADP back into ATP. That recharge step requires free phosphate. The clue is in the name: the three P's in ATP are phosphate groups. No phosphate, no recharge.
An analogy. Think of ATP as a rechargeable battery and phosphate as the charge it carries. Using energy “discharges” the battery (ATP → ADP); eating and breathing run the charger that “refills” it (ADP + phosphate → ATP). When phosphate is plentiful, batteries recharge as fast as you drain them and you feel energetic. When phosphate runs low, the charger has nothing to push back into the battery — so cells across the body are left running on half-charged batteries that never fully top up. That is the fatigue: not a broken engine, but a depleted, slow-to-recharge power supply feeding every organ at once. Because every cell depends on ATP, the tiredness is whole-body and global rather than confined to one muscle or one place.
Phosphate is so central to energy metabolism that the body normally guards its level tightly, keeping serum phosphate in roughly the 2.5–4.5 mg/dL range in adults (children run higher). When that level falls, intracellular ATP synthesis is impaired, and tissues with the highest energy demand — muscle, brain, heart, and the diaphragm — are the first to register the shortfall. This is why the classic clinical descriptions of severe hypophosphatemia, going back to Knochel's foundational work in the 1970s, center on weakness, lethargy, confusion, and impaired muscle (including respiratory muscle) function: all are downstream of cells that cannot keep their ATP topped up.
Phosphate also forms the backbone of other essential energy-handling molecules — creatine phosphate (the muscle's rapid-access energy reserve), NADPH, and the phosphorylated sugars of glycolysis — so a phosphate shortage throttles energy production at several points at once, not just at the final ATP step.
A Second Hit: Phosphate, 2,3-DPG, and Oxygen Delivery
There is a second, less obvious way low phosphate causes fatigue, and it involves your red blood cells. Inside red cells, phosphate is used to make a compound called 2,3-diphosphoglycerate (2,3-DPG). This molecule sits inside hemoglobin and acts like a release lever: it nudges hemoglobin to let go of its oxygen once the blood reaches the tissues that need it. Without enough 2,3-DPG, hemoglobin clings to its oxygen too tightly and delivers less of it to working muscle and brain.
When phosphate falls, red-cell 2,3-DPG falls with it. The result, demonstrated in classic studies by Travis and colleagues, is a leftward shift of the oxygen–hemoglobin dissociation curve — meaning your blood can be carrying a normal amount of oxygen yet hand off less of it where it is needed. So low phosphate delivers a double blow to energy: cells make ATP less efficiently and receive less of the oxygen required to make ATP in the first place. The practical experience of that double hit is exactly what people report — profound, out-of-proportion tiredness and a sense of being winded or depleted by ordinary effort.
In severe, sustained hypophosphatemia the same energy-and-oxygen squeeze on red cells can make them fragile (a rare complication called hemolysis), which is one more reason clinicians take a markedly low phosphate seriously rather than treating tiredness as a minor complaint.
Honesty: Fatigue Has Many Causes
It would be misleading to suggest that fatigue means low phosphate. Tiredness is one of the most common and least specific symptoms in all of medicine, and low phosphate is a relatively uncommon cause of it in people who are otherwise well and eating normally. Most fatigue has nothing to do with phosphate at all. Being honest about that is part of using this information well: the goal is to know when phosphate is worth checking, not to pin every tired day on a mineral.
Far more common explanations for persistent fatigue include:
- Iron-deficiency and other anemias — too few or under-fueled red cells, a leading cause of fatigue, especially in menstruating women. See anemia.
- Thyroid disease — an underactive thyroid slows the whole metabolism and is a classic, very treatable cause of tiredness. See thyroid disorders.
- Poor or disrupted sleep — including sleep apnea, insomnia, and shift work.
- Depression and chronic stress — among the most common reasons people seek help for low energy.
- Diabetes and blood-sugar problems — see diabetes.
- Chronic fatigue syndrome (ME/CFS), post-viral fatigue, medication side effects, and many chronic illnesses. See chronic fatigue syndrome.
- Other electrolyte and mineral shortfalls — including low magnesium and low potassium, which can travel with low phosphate and cause overlapping tiredness.
The fair summary is this: low phosphate is a real and sometimes overlooked cause of genuine fatigue, but it is rarely the first thing to suspect in a healthy person. It moves up the list sharply in the specific settings described next.
Clues That Point Toward Low Phosphate
Fatigue is worth investigating for low phosphate when the context fits. The following clues raise the suspicion enough that a phosphate level becomes a reasonable test:
- It comes with muscle weakness or bone aches. Fatigue plus genuine loss of strength (muscle weakness) or aching, tender bones (bone pain and softening) is a more phosphate-specific pattern than tiredness alone.
- It appears during refeeding. Tiredness, weakness, or confusion in the first days of being fed after starvation, severe weight loss, anorexia, or prolonged alcohol use is a hallmark of refeeding syndrome and is a phosphate emergency until proven otherwise.
- It tracks heavy alcohol use. Chronic heavy drinking depletes phosphate through poor intake, vomiting, and urinary loss, and a binge or withdrawal can drop it sharply.
- It accompanies recovery from a diabetic crisis. Profound fatigue during treatment of diabetic ketoacidosis is partly explained by phosphate shifting into cells with insulin.
- It comes with a known kidney, parathyroid, or vitamin D problem. Phosphate handling depends on the kidneys, on parathyroid hormone, and on vitamin D; disorders of any of these can lower it.
- It started after certain medications — some antacids that bind phosphate, intravenous iron formulations, and diuretics can lower phosphate.
Outside contexts like these, an isolated complaint of tiredness in a well-nourished person is far more likely to be one of the common causes listed above — which is exactly why a clinician evaluating fatigue usually screens broadly (blood count, thyroid, glucose) and checks phosphate when the story points to it.
Common Situations That Cause It
Phosphate is abundant in everyday food — it is found in dairy, meat, fish, eggs, beans, nuts, and whole grains — so low phosphate from diet alone is uncommon in people who eat normally. When it does occur, it almost always reflects one of three processes: phosphate shifting rapidly into cells, the kidneys wasting it into the urine, or the gut failing to absorb it. The main culprits:
- Refeeding. When someone who has been starved or severely malnourished is fed (especially carbohydrate) too quickly, the resulting insulin surge drives phosphate rapidly into cells to build new ATP, and serum phosphate can crash within hours. This is the single most important and most dangerous cause — covered in depth on the refeeding syndrome page.
- Chronic alcohol use. Heavy drinkers are prone to low phosphate from poor diet, vomiting, vitamin D problems, and increased urinary losses; levels can fall further during withdrawal and when eating resumes.
- Diabetic ketoacidosis (DKA) treatment. Insulin given to treat a diabetic crisis pushes phosphate into cells, sometimes unmasking a large total-body deficit as a low blood level during recovery.
- Critical illness and sepsis. Hypophosphatemia is common in intensive-care patients, driven by cellular shifts, kidney losses, and treatments; it is one of the most frequent electrolyte disturbances in the ICU.
- Kidney phosphate wasting. The kidney is the master regulator of phosphate. Overactive parathyroid hormone (hyperparathyroidism), certain inherited tubular disorders, and the hormone FGF23 can all make the kidney dump phosphate into the urine.
- Poor absorption. Vitamin D deficiency, malabsorption conditions, chronic diarrhea, and the long-term use of phosphate-binding antacids reduce how much phosphate the gut takes up.
- Certain medications. Some intravenous iron preparations, diuretics, and high-dose corticosteroids can lower phosphate.
Pinning down which mechanism is at work matters, because the fix differs: slowing a refeed, replacing vitamin D, adjusting a medication, or treating an overactive parathyroid gland are very different responses.
Getting Tested
Confirming low phosphate as a contributor to fatigue is straightforward and inexpensive. Phosphate is measured directly on a simple blood draw — it is reported as serum phosphate (sometimes labeled “phosphorus,” PO4, or P), with a normal adult range of roughly 2.5–4.5 mg/dL. Phosphate appears on most kidney function and metabolic test bundles; note that it is not always on the most basic Comprehensive Metabolic Panel, so a clinician evaluating possible low phosphate will request it specifically.
Because fatigue has so many causes, a sensible work-up rarely stops at phosphate. A clinician investigating tiredness typically checks a broad panel first — a complete blood count for anemia, thyroid function for thyroid disease, glucose for diabetes — and adds phosphate when the context fits. If phosphate is low, the next step is to find out why:
- A 25-hydroxy vitamin D level — deficiency reduces phosphate absorption and is common and easily corrected.
- Calcium and parathyroid hormone (PTH) — to screen for hyperparathyroidism, which drives phosphate into the urine.
- A urine phosphate measurement — this distinguishes whether phosphate is being wasted by the kidney (high urine phosphate) or lost/shifted elsewhere (low urine phosphate), which directs the search for a cause.
- Magnesium and potassium — these frequently fall alongside phosphate (a magnesium test is usually ordered separately), and overlapping deficits add to the fatigue.
The takeaway for patients: a single inexpensive blood test can confirm or exclude low phosphate, and a handful of follow-up tests usually reveals the reason — which is what makes the fatigue fixable.
Correcting Low Phosphate Safely
How phosphate is replaced depends on how low it is, how fast it dropped, and how the person feels. The guiding principle is to match the urgency to the danger — food and oral repletion for mild deficits, and careful intravenous correction for severe or symptomatic ones — while always treating the underlying cause.
- Food first, for mild cases. When phosphate is only modestly low and the person is otherwise well, phosphate-rich whole foods are the foundation. Good sources include dairy (milk, yogurt, cheese), eggs, fish and lean meats, lentils and beans, nuts, seeds, and whole grains. Whole-food phosphate comes packaged with protein and other nutrients and rarely causes overshoot.
- Oral phosphate supplements — prescribed when diet isn't enough or when phosphate keeps draining. They are dosed and monitored by a clinician; a common side effect is diarrhea, and they are not something to self-prescribe at high doses.
- Intravenous (IV) phosphate — reserved for severe hypophosphatemia or dangerous symptoms (marked weakness, breathing trouble, confusion) or when someone can't take it by mouth. IV phosphate is given at a controlled rate with blood monitoring, because replacing it too quickly can drop calcium dangerously and deposit calcium-phosphate in tissues.
- Replace vitamin D, magnesium, and potassium too. Correcting a vitamin D deficiency restores phosphate absorption, and low magnesium or potassium often travels alongside and needs its own correction.
- Fix the cause. Slowing a too-fast refeed, treating alcohol-use disorder, adjusting a phosphate-lowering medication, or managing an overactive parathyroid gland is what makes the correction last.
A note of caution that matters in kidney disease: because the kidneys regulate phosphate, people with reduced kidney function can swing the other way into high phosphate if they supplement without guidance — which is harmful in its own right. This is why phosphate replacement is individualized and clinician-guided rather than one-size-fits-all.
When to Seek Care / Red Flags
Most mild low-phosphate fatigue is corrected calmly with diet, a vitamin D check, and a clinician's guidance. But certain features mean seek medical help promptly, and some mean call for emergency help, because they signal that phosphate may have fallen to a dangerous level:
- Fatigue with new muscle weakness that is worsening, spreading, or affecting your ability to stand, walk, or hold things up (see muscle weakness).
- Trouble breathing — shortness of breath or the sense you can't take a full breath. Severe hypophosphatemia can weaken the diaphragm; treat this as an emergency.
- New confusion, disorientation, irritability, or seizures — the brain is highly energy-dependent, and these can reflect a profoundly low level.
- Palpitations, fainting, or chest discomfort — very low phosphate can affect the heart muscle and rhythm.
- Any of the above appearing during refeeding — in the first days of eating after starvation, severe weight loss, anorexia, or heavy alcohol use. This is a classic refeeding syndrome emergency.
- Persistent unexplained fatigue that doesn't improve with rest — not an emergency, but a clear reason to see a clinician and have it investigated rather than dismissed.
The dangerous pattern is fatigue that is joined by breathing trouble, confusion, or rapidly worsening weakness, because at that point the same low phosphate starving your muscles of energy can also be affecting the heart, brain, and diaphragm. When in doubt, err toward being seen — confirming or ruling out severe hypophosphatemia takes one quick blood test.
Key Research Papers
- Amanzadeh J, Reilly RF Jr (2006). Hypophosphatemia: an evidence-based approach to its clinical consequences and management. Nature Clinical Practice Nephrology;2(3):136-148. — DOI: 10.1038/ncpneph0124
- Knochel JP (1977). The Pathophysiology and Clinical Characteristics of Severe Hypophosphatemia. Archives of Internal Medicine;137(2):203-220. — DOI: 10.1001/archinte.1977.03630140051013
- Knochel JP (1985). The Clinical Status of Hypophosphatemia. New England Journal of Medicine;313(7):447-449. — DOI: 10.1056/NEJM198508153130711
- Travis SF, Sugerman HJ, Ruberg RL, et al. (1971). Alterations of Red-Cell Glycolytic Intermediates and Oxygen Transport as a Consequence of Hypophosphatemia in Patients Receiving Intravenous Hyperalimentation. New England Journal of Medicine;285(14):763-768. — DOI: 10.1056/NEJM197109302851402
- Aubier M, Murciano D, Lecocguic Y, et al. (1985). Effect of Hypophosphatemia on Diaphragmatic Contractility in Patients with Acute Respiratory Failure. New England Journal of Medicine;313(7):420-424. — DOI: 10.1056/NEJM198508153130705
- Felsenfeld AJ, Levine BS (2012). Approach to Treatment of Hypophosphatemia. American Journal of Kidney Diseases;60(4):655-661. — DOI: 10.1053/j.ajkd.2012.03.024
- Mehanna HM, Moledina J, Travis J (2008). Refeeding syndrome: what it is, and how to prevent and treat it. BMJ;336(7659):1495-1498. — DOI: 10.1136/bmj.a301
- Penido MGMG, Alon US (2012). Phosphate homeostasis and its role in bone health. Pediatric Nephrology;27(11):2039-2048. — DOI: 10.1007/s00467-012-2175-z
- Geerse DA, Bindels AJ, Kuiper MA, et al. (2010). Treatment of hypophosphatemia in the intensive care unit: a review. Critical Care;14(4):R147. — DOI: 10.1186/cc9215
- Bech A, Blans M, Telting D, de Boer H (2013). Incidence and aetiology of renal phosphate loss in patients with hypophosphatemia in the intensive care unit. Intensive Care Medicine;39(10):1785-1791. — DOI: 10.1007/s00134-013-2970-4
- Imel EA, Econs MJ (2012). Approach to the Hypophosphatemic Patient. The Journal of Clinical Endocrinology & Metabolism;97(3):696-706. — DOI: 10.1210/jc.2011-1319
PubMed Topic Searches
- PubMed — Hypophosphatemia, ATP depletion, and muscle energy
- PubMed — Hypophosphatemia, 2,3-DPG, and oxygen delivery
- PubMed — Refeeding syndrome and hypophosphatemia
- PubMed — Hypophosphatemia, fatigue, and weakness
- PubMed — Hypophosphatemia in critical illness
Connections
- Hypophosphatemia Symptom Hub
- Hypophosphatemia and Muscle Weakness
- Hypophosphatemia and Bone Pain
- Refeeding Syndrome
- Phosphorus Overview
- Phosphorus and Energy Production
- Calcium
- Magnesium
- Potassium and Fatigue
- Vitamin D
- Comprehensive Metabolic Panel
- Kidney Function Test
- Hyperparathyroidism
- Kidney Disease
- Anemia
- Chronic Fatigue Syndrome