Hypophosphatemia (Low Phosphate): Refeeding Syndrome
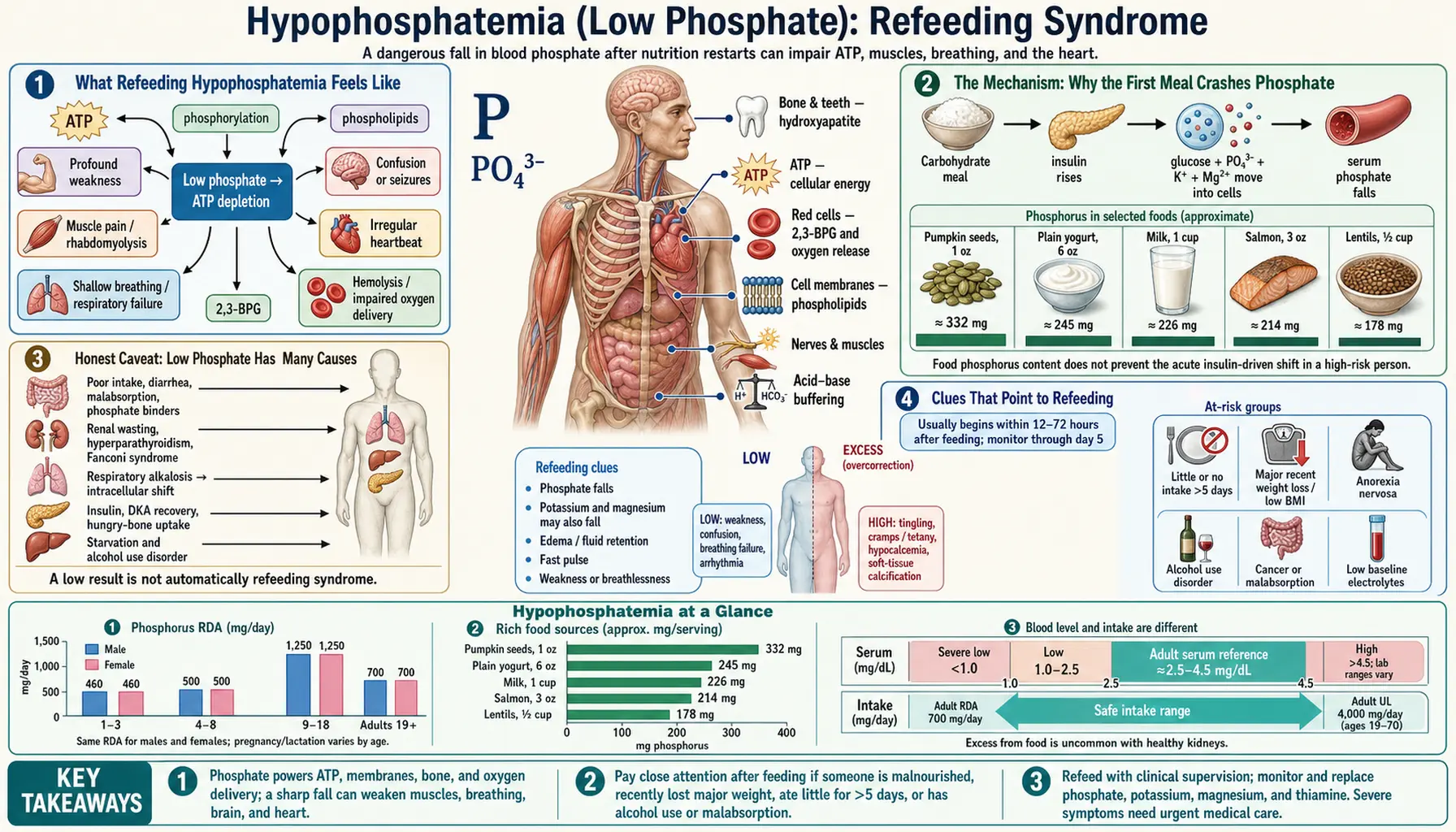
After days or weeks of eating very little, the most dangerous moment is not the starving — it is the first big meal. When a body that has been running on empty is suddenly fed carbohydrate, a surge of insulin sweeps phosphate out of the blood and into starved cells, and the level can crash within hours. That crash — refeeding hypophosphatemia — is the heart of refeeding syndrome, a state that can cause heart failure, breathing failure, seizures, and sudden death in someone who looked like they were finally getting better. This page explains why feeding a malnourished person can paradoxically harm them, why phosphate is the mineral that falls hardest and fastest, who is most at risk, and how the danger is prevented — by feeding slowly and replacing phosphate before it bottoms out.
Table of Contents
- What Refeeding Hypophosphatemia Feels Like
- The Mechanism: Why the First Meal Crashes Phosphate
- Honest Caveat: Low Phosphate Has Many Causes
- Clues That Point to Refeeding
- Who Is at Risk
- Getting Tested
- Preventing and Correcting It Safely
- When to Seek Care / Red Flags
- Key Research Papers
- Connections
- Featured Videos
What Refeeding Hypophosphatemia Feels Like
Refeeding syndrome is treacherous precisely because the early warning signs are quiet and easy to mistake for the malnutrition itself. The drop in phosphate usually begins within the first 72 hours of resuming feeding, and the person — or the family at the bedside — may notice a cluster of vague but escalating problems:
- New, deep weakness and exhaustion — far beyond the tiredness of being underfed. The muscles feel heavy and useless; getting out of bed or lifting the arms becomes hard. (Phosphate-starved muscle simply cannot generate force; see the sibling page on muscle weakness.)
- Breathlessness or shallow breathing — the diaphragm is a muscle too, and when it weakens, each breath moves less air. People describe feeling short of breath at rest or unable to take a full breath.
- A racing, pounding, or irregular heartbeat — palpitations, or a heart rate that climbs without exertion. This reflects strain on a heart muscle that is suddenly short of the fuel it needs.
- Swelling of the legs and ankles — fluid retention is common as the refed body holds on to salt and water.
- Confusion, irritability, numbness, or tingling — the brain and nerves are sensitive to falling phosphate; in severe cases seizures can occur.
The cruel feature of these symptoms is their timing. They appear when the person is supposed to be recovering — after the feeding tube goes in, after the first real meals, after admission to hospital for malnutrition. A patient who seemed stable can deteriorate sharply over a day or two. That is why anyone refeeding a severely undernourished person watches not for the slow return of strength but for the sudden appearance of weakness, breathlessness, swelling, or a fast heartbeat.
The Mechanism: Why the First Meal Crashes Phosphate
To understand refeeding syndrome you have to understand what starvation does first. When the body is deprived of food for days, it switches off the carbohydrate economy and burns fat and protein for fuel. Insulin — the hormone that handles incoming sugar — falls to almost nothing. Over time, the body's total stores of phosphate, potassium, and magnesium become quietly depleted, even though the blood levels can still look normal, because the body shifts these minerals out of cells to keep the blood concentration up. The tank is nearly empty, but the fuel gauge still reads full.
Then comes the meal — especially one rich in carbohydrate. Glucose floods in, and the pancreas answers with a surge of insulin. Insulin does several things at once: it drives glucose into cells, and it pulls phosphate, potassium, and magnesium in along with it. Inside the cell, that incoming glucose is immediately put to work building ATP — the molecule the body uses as energy currency — and ATP is built around phosphate. Cells also crank up production of a molecule called 2,3-DPG and rebuild their structures, all of which consume phosphate. So the body's cells, suddenly switched back on, gulp phosphate out of the bloodstream faster than the (already depleted) stores can supply it. Serum phosphate — normally about 2.5–4.5 mg/dL — can plummet within hours.
An analogy. Picture a town that has been under a power blackout for two weeks. The reservoir is nearly dry, but because nothing is running, the water tower at the top of the hill still looks full. Then the power comes back all at once: every factory, pump, and household turns on its taps simultaneously. The tower drains in minutes, and the whole town loses pressure. Refeeding is that moment the power comes back on. The "water" is phosphate; the simultaneous demand is every starved cell switching its machinery back on at once; and the sudden loss of pressure is the dangerous crash in blood phosphate that follows the first meal.
Phosphate matters here more than almost any other mineral because it is the literal backbone of cellular energy. Every cell that needs to do work — heart muscle pumping, the diaphragm breathing, nerves firing, red blood cells carrying oxygen — needs phosphate to make ATP. When phosphate bottoms out, ATP production stalls across the body at the exact moment demand is rising. (Phosphorus's central role in energy is covered on the Phosphorus and Energy Production page.) The heart can fail to pump, the diaphragm can fail to breathe, red cells release oxygen poorly, and nerves misfire — all traceable to a mineral that, days earlier, looked normal on a blood test. Potassium and magnesium fall by the same insulin-driven shift, and a deficiency of thiamine (vitamin B1), also depleted by starvation, can be unmasked by the carbohydrate load — which is why refeeding syndrome is a multi-mineral, multi-vitamin emergency, not phosphate alone.
Honest Caveat: Low Phosphate Has Many Causes
It is important to be straight about this: a low phosphate level is not proof of refeeding syndrome. Hypophosphatemia is fairly common in hospitalized patients and has a long list of causes that have nothing to do with feeding a starved person. Before assuming refeeding, clinicians weigh the alternatives:
- Other shifts of phosphate into cells. Anything that triggers an insulin surge or a metabolic shift can do it — recovery from diabetic ketoacidosis after insulin is started, treatment of severe high blood sugar, or a state called respiratory alkalosis (from rapid over-breathing) that drives phosphate into cells independently of food.
- Kidney losses. The kidneys normally reclaim most filtered phosphate; certain inherited tubular disorders, some medications (including some used for cancer and bone disease), excess parathyroid hormone, and rare tumors that secrete a phosphate-wasting hormone (FGF23) all make the kidney dump phosphate into the urine.
- Poor absorption or intake. Long-term heavy use of antacids that bind phosphate, chronic diarrhea or malabsorption, severe vitamin D deficiency, and chronic alcohol overuse all lower phosphate over time.
- Acute illness. Severe infection (sepsis) and major surgery commonly drop phosphate transiently.
So a low phosphate reading is a clue, not a verdict. What turns it into "refeeding hypophosphatemia" is the context: a person who was undernourished or barely eating and who has just started being fed. The mechanism is the same falling phosphate, but the trigger — and therefore the prevention — is specific to refeeding. The same caution applies in reverse: never wave away a sharp phosphate drop in a refed patient as "just their illness." In the right context it is the harbinger of a recognized, sometimes fatal syndrome.
Clues That Point to Refeeding
Several features help distinguish refeeding hypophosphatemia from the other causes above and raise the alarm early:
- The timing. The phosphate fall begins within hours to a few days of starting nutrition — oral, tube, or intravenous — in someone who had been eating little. A normal phosphate before feeding that drops afterward is the signature pattern.
- The set-up. A clear period of low intake or weight loss precedes it: prolonged fasting, an eating disorder, alcohol-use disorder, advanced cancer, or simply an older adult who stopped eating during an illness.
- The company it keeps. Phosphate rarely falls alone in refeeding — potassium and magnesium usually drop with it (because the same insulin surge drives all three into cells), and the person may retain fluid. A simultaneous fall in all three minerals after feeding is highly suggestive. By contrast, an isolated low phosphate with normal potassium and magnesium points more toward a kidney-wasting cause.
- The carbohydrate trigger. The crash is worst after carbohydrate-heavy feeding (sugary drinks, dextrose-containing IV fluids, high-carb tube feeds), because carbohydrate is what drives the insulin surge.
For a patient or family member, the practical clue is simply this: if weakness, breathlessness, swelling, or a racing heart appear in the first days after a malnourished person begins eating or is put on a feeding tube, refeeding syndrome should be on the list, and a phosphate level should be checked without delay. For the broader, slower forms of low phosphate — the kind that cause aching bones or chronic tiredness rather than an acute crash — see the sibling pages on bone pain and softening and fatigue.
Who Is at Risk
Refeeding syndrome only happens to people whose bodies have been depleted by inadequate nutrition — but that population is larger and more varied than many people expect. Widely used criteria (originally from the UK's National Institute for Health and Care Excellence) flag someone as at significant risk if they have one or more of the following:
- Very low body weight (a body-mass index below about 16), or unintentional loss of more than 15% of body weight over the previous three to six months.
- Little or no nutritional intake for more than 10 days.
- Low phosphate, potassium, or magnesium before feeding starts — a red flag that stores are already depleted.
The risk is even higher (a person needs only two of a slightly relaxed set of criteria) and includes a longer list of clinical situations:
- Anorexia nervosa and other eating disorders — the classic and most-studied setting, where well-meaning, too-rapid refeeding has caused deaths.
- Chronic alcohol-use disorder — poor intake plus the kidney and magnesium losses alcohol causes.
- Advanced cancer and chronic wasting illnesses, where appetite and intake have been poor for weeks.
- Prolonged fasting, hunger strikes, or post-surgical patients who have had little nutrition for many days.
- Older adults who have stopped eating during an acute illness, depression, or after a hospital admission — an under-recognized and growing group.
- Poorly controlled diabetes, malabsorption (such as after bariatric surgery or in inflammatory bowel disease), and long-term use of antacids or diuretics.
What unites all of these is a body running on depleted reserves that is about to be fed. Recognizing the risk before the first meal is the entire game, because refeeding syndrome is far easier to prevent than to treat.
Getting Tested
The test is simple, cheap, and decisive: a blood draw that measures serum phosphate, along with potassium and magnesium. Phosphate and potassium are reported on a standard Comprehensive Metabolic Panel in many labs (some basic panels omit phosphate and magnesium, so these are often ordered specifically). Magnesium is not on a standard CMP and must be requested separately. In anyone at risk of refeeding, these levels are checked before feeding starts and then repeated frequently — often daily, or even more than once a day in the highest-risk patients — during the first several days of nutrition.
The normal serum phosphate range is roughly 2.5–4.5 mg/dL (about 0.8–1.45 mmol/L) in adults. Severity is judged not only by the number but by how fast it falls and how the person looks:
- Mild–moderate hypophosphatemia (1.0–2.5 mg/dL) — may cause weakness and fatigue; handled with oral or careful intravenous replacement and slowing the feeding.
- Severe hypophosphatemia (below ~1.0 mg/dL) — the dangerous zone, where heart failure, respiratory failure, seizures, and serious muscle breakdown become real risks. This is treated urgently, usually with intravenous phosphate and close monitoring.
Because the phosphate before feeding can look reassuringly normal even when total-body stores are empty, a single baseline value is never enough in an at-risk person. The whole point of monitoring is to catch the drop after feeding begins, while it can still be corrected. An electrocardiogram (ECG) and continuous heart monitoring are often added in severe cases, because the same electrolyte shifts that endanger the muscles can destabilize the heart's rhythm.
Preventing and Correcting It Safely
The governing principle of refeeding is counterintuitive but lifesaving: in a severely starved person, feed slowly and cautiously, not generously. The instinct to "build them back up" with full meals is exactly what triggers the syndrome. Modern guidance from groups such as the American Society for Parenteral and Enteral Nutrition (ASPEN) follows a consistent shape:
- Start low and go slow. In high-risk patients, nutrition is begun at a small fraction of full calorie needs — often only about a quarter to half of the target on day one — and increased gradually over several days as the labs stay stable. Carbohydrate is held back deliberately, because it is the carbohydrate that drives the insulin surge.
- Replace minerals proactively, before they crash. Phosphate, potassium, and magnesium are checked and corrected at the start and replaced during feeding — not only after a low value appears. Phosphate may be given by mouth for milder deficits or intravenously for severe ones, at a controlled rate.
- Give thiamine (vitamin B1) first. Because starvation depletes thiamine and a carbohydrate load can trigger a severe neurological crisis (Wernicke encephalopathy) in a thiamine-deficient person, thiamine is given before or with the first carbohydrate — a cheap, simple, and essential step.
- Monitor relentlessly. Daily (or more frequent) electrolytes, fluid balance, and heart monitoring during the first days catch trouble while it is still fixable. Feeding is slowed or paused if phosphate falls sharply.
- Restrict fluid and salt as needed. Because the refed body tends to retain salt and water, careful fluid management helps prevent the swelling and heart strain that accompany the syndrome.
Crucially, recognizing the danger does not mean withholding food — a starving person must be fed, and refusing nutrition is its own harm. It means feeding correctly: starting cautiously, supplementing minerals and thiamine, and monitoring closely so the level can be supported before it collapses. Done this way, even very high-risk patients can be refed safely. This is medical care that belongs in a clinical setting; it is not something to manage at home with supplements. If you are caring for someone who has eaten very little for a long time, the safest thing you can do is get them assessed before a return to normal eating, so a refeeding plan can be put in place.
When to Seek Care / Red Flags
Refeeding syndrome is a medical emergency that develops fast. If a person who has been undernourished or barely eating has recently started eating again, been put on a feeding tube, or been given IV nutrition, treat any of the following as a reason to get emergency medical help immediately — not to wait for a routine appointment:
- Trouble breathing — new shortness of breath, shallow or labored breathing, or an inability to take a full breath.
- A racing, pounding, or irregular heartbeat, fainting, or near-fainting — signs the heart's rhythm may be destabilizing (see arrhythmia).
- Sudden severe weakness, especially if it is spreading or affecting breathing.
- Confusion, drowsiness, severe agitation, or a seizure.
- Rapid swelling of the legs, marked fluid retention, or sudden weight gain in the days after feeding begins.
- Numbness, tingling, or muscle spasms — which can reflect the falling magnesium and calcium that accompany the syndrome.
The single most protective action is preventive: anyone at risk — a person with an eating disorder, severe alcohol-use disorder, advanced illness, or a long stretch of barely eating — should have their electrolytes checked and a cautious refeeding plan made before they resume normal eating. When the danger is recognized in advance, refeeding syndrome is highly preventable; when it is missed, a phosphate crash can turn an apparent recovery into a crisis within a day. When in doubt, be seen — confirming or ruling it out takes one quick blood test.
Key Research Papers
- Mehanna HM, Moledina J, Travis J (2008). Refeeding syndrome: what it is, and how to prevent and treat it. BMJ;336(7659):1495-1498. — DOI: 10.1136/bmj.a301
- Crook MA, Hally V, Panteli JV (2001). The importance of the refeeding syndrome. Nutrition;17(7-8):632-637. — DOI: 10.1016/S0899-9007(01)00542-1
- da Silva JSV, Seres DS, Sabino K, et al. (2020). ASPEN Consensus Recommendations for Refeeding Syndrome. Nutrition in Clinical Practice;35(2):178-195. — DOI: 10.1002/ncp.10474
- Boateng AA, Sriram K, Meguid MM, Crook M (2010). Refeeding syndrome: treatment considerations based on collective analysis of literature case reports. Nutrition;26(2):156-167. — DOI: 10.1016/j.nut.2009.11.017
- Stanga Z, Brunner A, Leuenberger M, et al. (2008). Nutrition in clinical practice—the refeeding syndrome: illustrative cases and guidelines for prevention and treatment. European Journal of Clinical Nutrition;62(6):687-694. — DOI: 10.1038/sj.ejcn.1602854
- Marinella MA (2003). The refeeding syndrome and hypophosphatemia. Nutrition Reviews;61(9):320-323. — DOI: 10.1301/nr.2003.sept.320-323
- Amanzadeh J, Reilly RF (2006). Hypophosphatemia: an evidence-based approach to its clinical consequences and management. Nature Clinical Practice Nephrology;2(3):136-148. — DOI: 10.1038/ncpneph0124
- Gaasbeek A, Meinders AE (2005). Hypophosphatemia: an update on its etiology and treatment. The American Journal of Medicine;118(10):1094-1101. — DOI: 10.1016/j.amjmed.2005.02.014
- Geerse DA, Bindels AJ, Kuiper MA, et al. (2010). Treatment of hypophosphatemia in the intensive care unit: a review. Critical Care;14(4):R147. — DOI: 10.1186/cc9215
- Friedli N, Stanga Z, Sobotka L, et al. (2018). Revisiting the refeeding syndrome: results of a systematic review. Nutrition;47:13-20. — PubMed
- Kraft MD, Btaiche IF, Sacks GS (2005). Review of the refeeding syndrome. Nutrition in Clinical Practice;20(6):625-633. — PubMed
- National Institutes of Health, Office of Dietary Supplements. Phosphorus — Health Professional Fact Sheet. — NIH ODS
PubMed Topic Searches
- PubMed — Refeeding syndrome and hypophosphatemia
- PubMed — Refeeding syndrome in anorexia nervosa
- PubMed — Prevention and electrolyte monitoring in refeeding
- PubMed — Treatment of severe hypophosphatemia
- PubMed — Refeeding, thiamine, and Wernicke encephalopathy
Connections
- Hypophosphatemia Symptom Hub
- Hypophosphatemia and Muscle Weakness
- Hypophosphatemia and Bone Pain & Softening
- Hypophosphatemia and Fatigue
- Phosphorus Overview
- Phosphorus and Energy Production
- Phosphorus and Bone Mineralization
- Potassium
- Hypokalemia Symptom Hub
- Magnesium
- Calcium
- Comprehensive Metabolic Panel
- Eating Disorders
- Diabetes
- Arrhythmia
- Fasting