Hypokalemia and Fatigue: Why Low Potassium Leaves You Exhausted
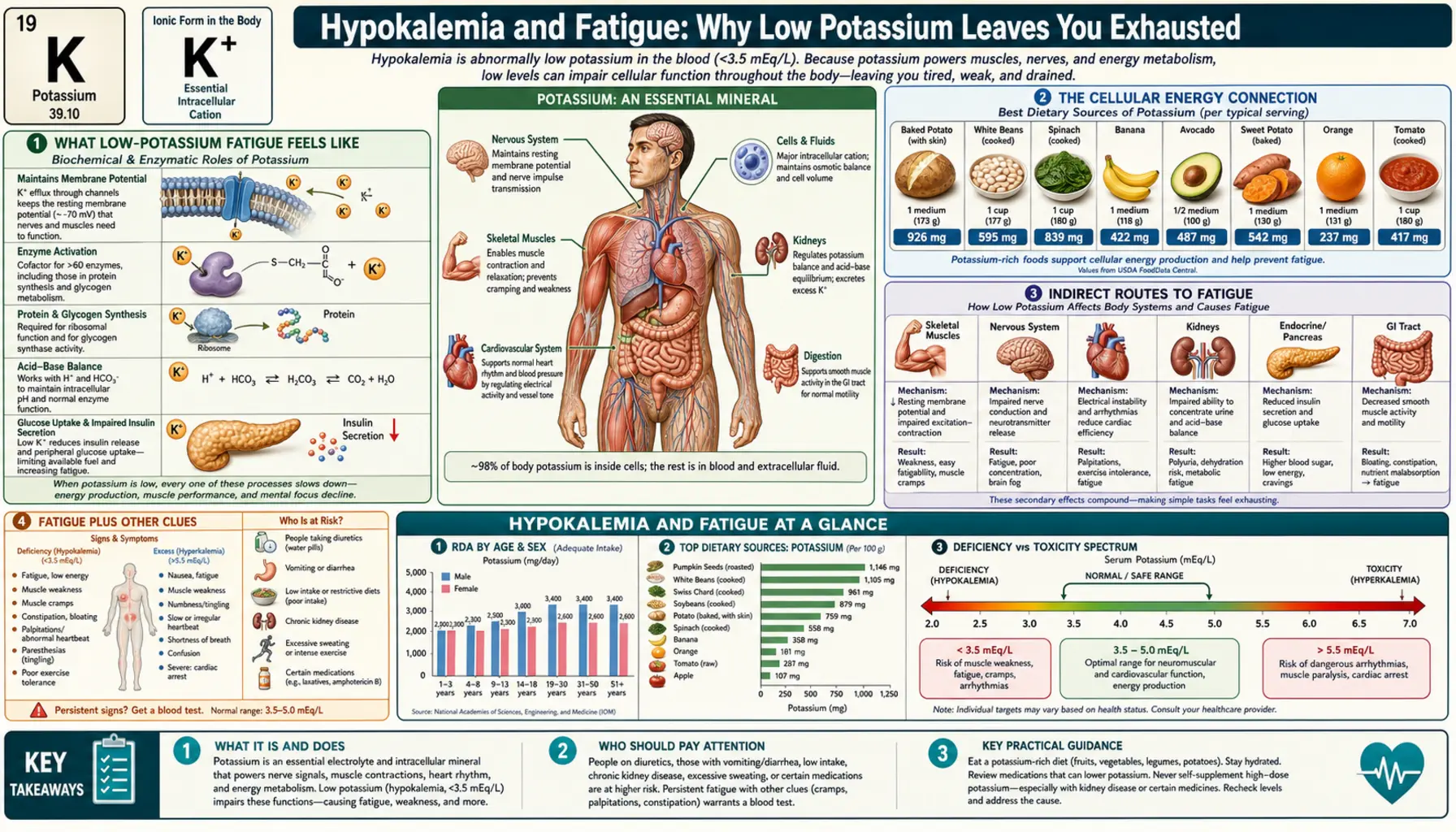
If you feel wrung out for no obvious reason — drained even after a full night's sleep, running on empty by mid-afternoon, foggy and low on stamina — low potassium is one possible piece of the puzzle. Potassium sits at the very center of how every cell makes and uses energy, so when blood levels drift low (hypokalemia, a potassium below about 3.5 mEq/L), a whole-body tiredness can set in long before anything dramatic happens. But here is the honest part: fatigue is the least specific symptom in all of medicine. Thyroid disease, low iron, anemia, low B12 or vitamin D, poor sleep, depression, and unsteady blood sugar cause exactly the same exhausted feeling — and they are far more common than hypokalemia. This page explains why low potassium can sap your energy, how it differs from the loss of muscle strength covered on the Muscle Weakness page, the other causes worth ruling out, and the simple blood test that sorts most of it out at once.
Interactive Visualization The Sodium–Potassium Pump — why you have a voltage Run the pump that gives every cell its charge — three sodium out, two potassium in, on Mg-ATP — then drop the magnesium and see exactly why low potassium refuses to correct. Launch →
Table of Contents
- What Low-Potassium Fatigue Feels Like
- The Cellular Energy Connection
- Indirect Routes to Fatigue
- Fatigue Plus Other Clues
- Other Causes of Fatigue to Consider
- Common Causes of the Low Potassium Itself
- The Magnesium Overlap
- Getting Tested
- Restoring Energy: Food First + Repletion
- When to Seek Care
- Key Research Papers
- Connections
- Featured Videos
What Low-Potassium Fatigue Feels Like
The fatigue of low potassium is a whole-body, “running on empty” tiredness rather than a problem with one muscle or one joint. People describe it in remarkably consistent ways:
- Deep tiredness that rest doesn't fix. You sleep a normal number of hours and still wake up feeling like you never recharged. The tank simply refuses to fill.
- Low stamina and early exhaustion. Ordinary activities — a flight of stairs, grocery shopping, a short walk — leave you needing to sit down sooner than they used to. It is less about “I can't lift this” and more about “I have nothing left in reserve.”
- Mental fog and flatness. Concentration slips, thoughts feel slow, and motivation drains away. Many people call it “brain fog” or feeling mentally heavy.
- A sense of being drained, not sore. This is the key distinction. The tiredness is general and pervasive, not the localized ache or weakness of a specific muscle.
It helps to separate two things that often get blurred together. Fatigue is the global feeling of low energy — the subject of this page. Muscle weakness is the measurable loss of force when you try to push, lift, or grip, and it is covered separately on the Muscle Weakness page. The two frequently travel together in hypokalemia, but they are not the same: you can feel exhausted with normal strength, or have genuinely weak muscles without feeling especially “tired” in the global sense. Naming which one dominates helps you and your clinician aim the workup correctly.
One more honest note up front: there is no “fatigue that proves it's potassium.” The feeling itself looks identical no matter what is driving it. What raises suspicion for hypokalemia is the company it keeps — diuretic use, ongoing vomiting or diarrhea, muscle cramps, palpitations, or constipation alongside the tiredness (see Fatigue Plus Other Clues).
The Cellular Energy Connection
To understand why low potassium can leave you exhausted, it helps to know that potassium isn't a bystander in your energy system — it is part of the machinery itself.
Every cell in your body runs a tiny molecular pump in its outer membrane called the sodium–potassium pump (Na+/K+-ATPase). For each cycle it pushes three sodium ions out of the cell and pulls two potassium ions in, burning one molecule of ATP — the cell's energy currency — to do it. This pump keeps potassium concentrated inside cells (roughly 140 mEq/L) and sodium concentrated outside, an arrangement that powers nerve signals, muscle contraction, and the basic electrical “charge” that living cells maintain.
Here is the striking part: this single pump consumes a large share of the body's resting energy — roughly 20–40% of a cell's energy use, and a substantial fraction of your whole-body basal metabolic rate. A big chunk of the food you eat is spent just keeping potassium where it belongs. Potassium is not optional fuel on the side; it is woven directly into how cells generate and spend energy, so when the system that depends on potassium gradients is disturbed, low energy is an intuitive result.
Low potassium can drain energy through a second route: blood-sugar handling. Insulin — the hormone that moves glucose out of the bloodstream into cells for fuel — leans on potassium to work, and potassium even helps trigger insulin's release from the pancreas. When potassium runs low, insulin secretion and effectiveness can both be blunted, nudging blood sugar up and making it harder for cells to take in the glucose they need. Chronic potassium depletion has been linked to impaired glucose tolerance for exactly this reason — one more way the body becomes less efficient at turning food into usable energy.
None of this means a mildly low potassium will flatten a healthy person. The body defends its potassium level tightly and small dips are often silent. But it does explain why, mechanistically, a meaningful drop can show up as vague, hard-to-shake tiredness rather than a single dramatic symptom.
Indirect Routes to Fatigue
Beyond the direct cellular-energy story, low potassium can wear you down through several indirect routes that compound one another:
- Disrupted sleep. Night-time muscle cramps, the urge to urinate from the conditions that drive potassium loss (or the diuretics that cause it), and an unsettled, restless feeling can all fragment sleep. Poor sleep then becomes its own engine of daytime fatigue — a loop where the original problem and the tiredness feed each other.
- Palpitations and an uneasy heart. Potassium is central to a steady heart rhythm. Low levels can produce skipped or fluttering beats (see Heart Palpitations). Even when harmless, palpitations are unnerving, interrupt rest, and add a layer of anxiety and exhaustion.
- Reduced appetite and less food eaten. Hypokalemia slows the gut, and a sluggish digestive tract brings nausea, bloating, and a poor appetite (see the Nausea page). Eating less means less energy and fewer of the other anti-fatigue nutrients — iron, B12, magnesium — deepening the deficiencies that cause tiredness.
- Deficiencies cluster together. The conditions that drain potassium — diuretics, vomiting, diarrhea, poor diet, alcohol overuse — rarely take only potassium. They tend to pull magnesium, and often B vitamins and others, down at the same time, producing a tiredness no single nutrient fully explains. That is why correcting potassium alone sometimes only partly helps.
So the fatigue may be only partly “the potassium.” More often it is potassium plus the poor sleep, poor appetite, and companion shortfalls that arrive in the same package — which is why the fix has to address the whole picture, not one number.
Fatigue Plus Other Clues
Because fatigue on its own points nowhere, the most useful thing you can do is notice what comes with it. Hypokalemia becomes a more plausible explanation when the tiredness arrives alongside one or more of these — each of which has its own page in this cluster:
- Muscle cramps — especially calf or leg cramps, often at night. See Muscle Cramps.
- Genuine muscle weakness — struggling to climb stairs or rise from a chair, distinct from feeling generally drained. See Muscle Weakness.
- Palpitations — a fluttering, pounding, or skipped-beat sensation. See Heart Palpitations.
- Constipation — a sluggish, backed-up gut from slowed intestinal muscle. See Constipation.
- Diuretic (“water pill”) use — the single most common driver of low potassium in everyday practice. If you take a thiazide or loop diuretic and feel newly exhausted, low potassium deserves a look.
One symptom alone is weak evidence. Fatigue with cramps, weakness, palpitations, or constipation — particularly on a diuretic — is a far stronger reason to check a potassium level. That pattern is the signal; isolated tiredness is mostly noise.
Other Causes of Fatigue to Consider
This is the most important section on the page, so it earns plain talk: do not assume your fatigue is potassium. Tiredness is non-specific, and the conditions below are all more common than hypokalemia. A good evaluation looks for these before pinning fatigue on a mineral — and the good news is that one or two blood tests catch most of them at once.
- Thyroid disease. An underactive thyroid (hypothyroidism) is a classic, very common cause of fatigue, often with weight gain, cold intolerance, dry skin, and constipation. A simple TSH blood test screens for it.
- Anemia and low iron. Too few healthy red blood cells — or depleted iron stores even before full anemia sets in — starves tissues of oxygen and is a leading cause of fatigue, especially in menstruating women. Checked with a complete blood count and a ferritin (iron-stores) level.
- Low vitamin B12. B12 deficiency causes fatigue, “pins and needles,” and brain fog; it is common in older adults, vegetarians/vegans, and people on long-term acid-reducing or metformin medications.
- Low vitamin D. Insufficiency is widespread and is associated with tiredness and low mood; easily measured and easily corrected.
- Poor sleep and sleep apnea. Untreated obstructive sleep apnea — snoring with daytime sleepiness — is a frequently missed cause of relentless fatigue. So is simple chronic sleep deprivation.
- Depression and anxiety. Low energy, poor concentration, and unrefreshing sleep are core features of depression. Fatigue is often the symptom people notice first.
- Blood-sugar problems. Both undiagnosed diabetes and reactive swings in blood sugar can produce afternoon crashes and persistent tiredness.
The honest framing: low potassium can contribute to fatigue, but it is rarely the whole story and is far from the most likely cause in someone who simply feels tired. The right move is not to self-diagnose a mineral deficiency — it is to get a basic evaluation that screens this whole list together (see Getting Tested).
Common Causes of the Low Potassium Itself
If a test does show low potassium, the next question is why. Potassium drops for a handful of well-understood reasons:
- Diuretics (“water pills”). Thiazide and loop diuretics — prescribed for high blood pressure, heart failure, and fluid retention — make the kidneys excrete potassium along with the extra fluid. This is the most common cause of hypokalemia in everyday medicine.
- Gastrointestinal losses. Vomiting, diarrhea, laxative overuse, or fluid drained through an ostomy or nasogastric tube all flush potassium out of the body. A bad stomach bug or chronic diarrhea can do it.
- Hyperaldosteronism. When the adrenal glands overproduce the hormone aldosterone, the kidneys dump potassium and retain sodium. This often shows up as low potassium together with high blood pressure that is hard to control, and is a cause clinicians specifically look for.
- Poor intake. On its own, a low-potassium diet rarely causes severe deficiency in healthy people because the kidneys conserve potassium well. But a genuinely poor diet — common with alcohol use disorder, eating disorders, or frailty — combined with any of the losses above can tip someone into hypokalemia.
Two of these — vomiting/diarrhea and alcohol or poor diet — also drag magnesium down at the same time, which matters more than it first appears (next section).
The Magnesium Overlap
You cannot tell the full story of potassium and fatigue without magnesium, because the two minerals are deeply intertwined.
First, magnesium is itself a cause of fatigue. Low magnesium produces tiredness, muscle cramps, twitching, and a generally run-down feeling — symptoms that overlap heavily with low potassium. The same circumstances that drain potassium (diuretics, diarrhea, poor diet, heavy alcohol use) drain magnesium too, so the two deficiencies very commonly coexist.
Second — and this is the clinically crucial bit — low magnesium actively perpetuates low potassium. Magnesium is needed to keep potassium inside cells and to stop the kidneys from wasting it. When magnesium is depleted, the kidneys leak potassium no matter how much potassium you take in. This is why potassium that simply “won't come up” despite supplements is a textbook clue to check magnesium: until the magnesium is replaced, the potassium keeps slipping away. Correcting both together is often the only thing that works.
For someone whose main complaint is fatigue, the takeaway is practical: checking and fixing magnesium is part of fixing potassium, and may relieve some of the tiredness in its own right. See Magnesium and Magnesium Replenishment for how to restore it sensibly.
Getting Tested
The reassuring thing about fatigue is that a single visit and a basic blood draw can sort through most of the possibilities at once. There is no need to guess.
The cornerstone is a Comprehensive Metabolic Panel (CMP) — a common, inexpensive blood test that measures potassium directly, along with sodium, kidney function, glucose, and other chemistries. If your potassium is low, the CMP also gives the context (kidney function, blood sugar, bicarbonate) that helps explain why.
Because fatigue has so many causes, clinicians typically pair the CMP with a few add-ons to cover the common culprits in one sitting:
- Complete blood count (CBC) — flags anemia.
- Ferritin — reveals low iron stores even before anemia appears.
- TSH — screens the thyroid.
- Vitamin B12 and vitamin D — two correctable deficiencies that cause tiredness.
- Magnesium — especially important if potassium is low or won't normalize (see The Magnesium Overlap). Note that a normal blood magnesium does not fully rule out depletion, since most magnesium lives inside cells.
If a low potassium is unexpected, a clinician may simply repeat it. The point of testing is not to chase a single number but to see the whole panel together — which is what turns vague fatigue into an answer.
Restoring Energy: Food First + Repletion
If low potassium is confirmed as part of the picture, the path back to feeling normal is usually straightforward — and for most people it starts in the kitchen, not the pharmacy.
Food first. Whole foods are the safest and most sustainable way to restore potassium, because they deliver it gradually alongside other nutrients (and, with little risk of overshooting in people with healthy kidneys). Excellent sources include:
- Fruits: bananas, oranges, cantaloupe, dried apricots, and avocado.
- Vegetables: sweet potatoes, regular potatoes (with skin), spinach, and other leafy greens.
- Legumes: lentils, white beans, and other pulses — some of the most potassium-dense foods there are.
- Other: plain yogurt, salmon, and tomato products.
For a fuller list with portions, see the Potassium-Rich Foods page.
Fix the magnesium too. As covered above, potassium often won't stay up until magnesium is replaced. Magnesium-rich foods (nuts, seeds, legumes, leafy greens, whole grains) and, when needed, sensible supplementation are part of the same repair job.
Treat the cause, not just the number. Restoring energy lasts only if the reason for the loss is addressed — reviewing a diuretic with your prescriber, recovering from the illness that caused vomiting or diarrhea, or working up resistant high blood pressure for hyperaldosteronism.
Don't forget the basics. Even when potassium is the trigger, the fatigue-fighting fundamentals still matter and often do the heaviest lifting: steady, sufficient sleep; adequate hydration; regular meals to keep blood sugar even; and gentle movement as energy returns.
Supplements only with guidance. Potassium supplements can raise blood levels too high — a genuinely dangerous condition (hyperkalemia) — especially in people with kidney disease or on certain blood-pressure medicines (ACE inhibitors, ARBs, potassium-sparing diuretics). Prescription potassium is appropriate for some people, but it belongs under medical supervision with follow-up testing, not as DIY self-treatment for tiredness.
When to Seek Care
Most fatigue is not an emergency, and the right pace is usually a scheduled visit and a blood panel. But seek prompt or urgent medical care if your tiredness comes with any of the following, which can signal dangerously low potassium or a serious heart problem:
- Fainting, near-fainting, or severe lightheadedness.
- Heart palpitations that are fast, irregular, or persistent — or any chest pain, pressure, or shortness of breath.
- Marked or rapidly worsening muscle weakness — trouble walking, climbing stairs, or lifting your arms — as opposed to ordinary tiredness.
- Inability to keep fluids down from ongoing vomiting or diarrhea, especially with signs of dehydration.
The combination of fatigue plus fainting, palpitations, chest symptoms, or significant weakness warrants being evaluated without delay — very low potassium can trigger dangerous heart rhythms (see Arrhythmia), and that is the scenario this section exists to catch.
Key Research Papers
- Gennari FJ (1998). Hypokalemia. New England Journal of Medicine;339(7):451-458. — DOI: 10.1056/NEJM199808133390707
- Kardalas E, Paschou SA, Anagnostis P, et al. (2018). Hypokalemia: a clinical update. Endocrine Connections;7(4):R135-R146. — DOI: 10.1530/EC-18-0109
- Palmer BF (2015). Regulation of Potassium Homeostasis. Clinical Journal of the American Society of Nephrology;10(6):1050-1060. — DOI: 10.2215/CJN.08580813
- Unwin RJ, Luft FC, Shirley DG (2011). Pathophysiology and management of hypokalemia: a clinical perspective. Nature Reviews Nephrology;7(2):75-84. — DOI: 10.1038/nrneph.2010.175
- Clausen T (2003). Na+-K+ Pump Regulation and Skeletal Muscle Contractility. Physiological Reviews;83(4):1269-1324. — DOI: 10.1152/physrev.00011.2003
- Tardy AL, Pouteau E, Marquez D, et al. (2020). Vitamins and Minerals for Energy, Fatigue and Cognition: A Narrative Review of the Biochemical and Clinical Evidence. Nutrients;12(1):228. — DOI: 10.3390/nu12010228
- Huang CL, Kuo E (2007). Mechanism of Hypokalemia in Magnesium Deficiency. Journal of the American Society of Nephrology;18(10):2649-2652. — DOI: 10.1681/ASN.2007070792
- Chaker L, Bianco AC, Jonklaas J, Peeters RP (2017). Hypothyroidism. The Lancet;390(10101):1550-1562. — DOI: 10.1016/S0140-6736(17)30703-1
- Stabler SP (2013). Vitamin B12 Deficiency. New England Journal of Medicine;368(2):149-160. — DOI: 10.1056/NEJMcp1113996
- Thacher TD, Clarke BL (2011). Vitamin D Insufficiency. Mayo Clinic Proceedings;86(1):50-60. — DOI: 10.4065/mcp.2010.0567
- Kennedy DO (2016). B Vitamins and the Brain: Mechanisms, Dose and Efficacy — A Review. Nutrients;8(2):68. — DOI: 10.3390/nu8020068
- Verdon F, Burnand B, Stubi CL, et al. (2003). Iron supplementation for unexplained fatigue in non-anaemic women: double blind randomised placebo controlled trial. BMJ;326(7399):1124. — DOI: 10.1136/bmj.326.7399.1124
PubMed Topic Searches
- PubMed — Hypokalemia, fatigue, and weakness
- PubMed — Potassium depletion, insulin, and glucose intolerance
- PubMed — Magnesium deficiency, fatigue, and potassium
- PubMed — Evaluation of fatigue in primary care
- PubMed — Diuretic-induced hypokalemia
Connections
- The Sodium–Potassium Pump — interactive animation
- Hypokalemia Hub
- Hypokalemia and Muscle Weakness
- Hypokalemia and Muscle Cramps
- Hypokalemia and Nausea
- Hypokalemia and Constipation
- Potassium Overview
- Potassium-Rich Foods
- Potassium and Heart Rhythm
- Magnesium
- Magnesium Replenishment
- Comprehensive Metabolic Panel
- Heart Palpitations
- Arrhythmia
- Kidney Disease
- Bananas
- Sweet Potatoes
- Spinach
- Lentils