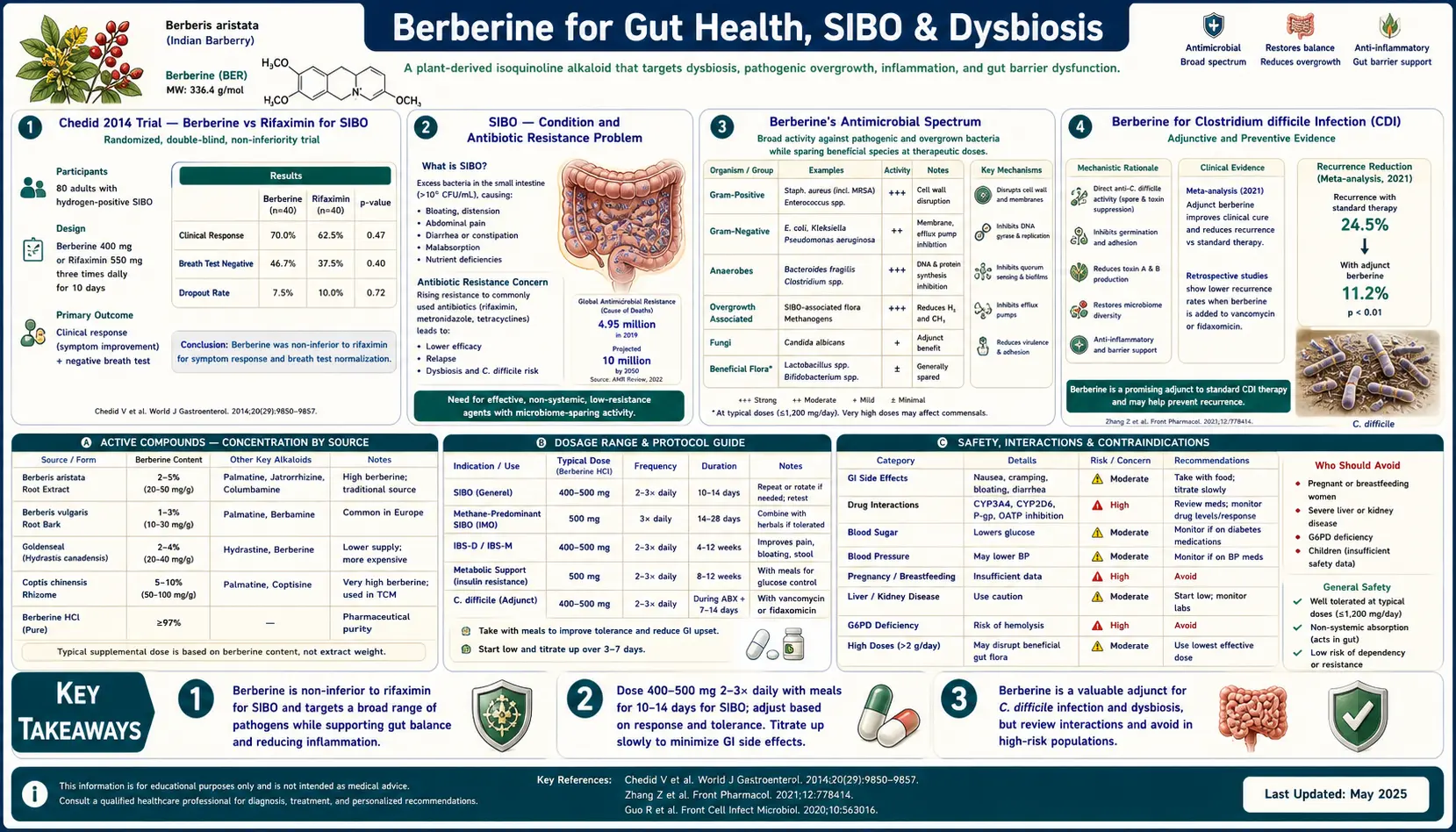
Berberine for Gut Health, SIBO & Dysbiosis
Long before berberine was a metformin alternative or a cholesterol-lowering herb, it was the antimicrobial of Traditional Chinese Medicine and Ayurveda — the yellow alkaloid in Coptis chinensis and Berberis bark used for two millennia to treat bacterial diarrhea, dysentery, and gastrointestinal infection. The modern evidence has caught up with the traditional use. The 2014 Chedid trial published in Global Advances in Health and Medicine showed that herbal antimicrobials (a blend including berberine, oregano oil, and others) were non-inferior to the prescription antibiotic rifaximin for eradicating small intestinal bacterial overgrowth (SIBO) on lactulose breath testing. The pilot data for berberine in recurrent Clostridium difficile infection are similarly promising. The mechanism is broad-spectrum: berberine has direct antimicrobial activity against Gram-positive bacteria, Gram-negative bacteria, yeasts (particularly Candida), and protozoa (Giardia, Entamoeba). It also serves as a sustainable third option in dysbiosis-rotation protocols that aim to avoid the resistance and microbiome disruption of repeated antibiotic courses. This deep-dive walks through the SIBO evidence, the C. diff data, the dysbiosis-rotation framework, and the practical protocols for using berberine as gut antimicrobial.
Table of Contents
- The Chedid 2014 Trial — Berberine vs Rifaximin for SIBO
- SIBO — The Condition and Why Antibiotic Resistance Is a Problem
- Berberine's Antimicrobial Spectrum
- Berberine for Clostridium difficile Infection
- Berberine for Helicobacter pylori
- Berberine for Giardia and Other Protozoa
- Berberine for Candida and Yeast Overgrowth
- The Dysbiosis Rotation Protocol
- Berberine's Effect on the Beneficial Microbiome
- Practical Protocol for SIBO Eradication
- Aftercare — Preventing Relapse
- Key Research Papers
- Connections
- Featured Videos
The Chedid 2014 Trial — Berberine vs Rifaximin for SIBO
The 2014 Chedid, Dhalla, Clarke, Roland, et al. trial at Johns Hopkins is the foundational modern evidence for using herbal antimicrobials including berberine in SIBO. The investigators conducted a retrospective chart review of 104 patients with newly diagnosed SIBO (positive lactulose breath test) who were treated with either:
- Rifaximin 1,200 mg/day (400 mg three times daily) for 4 weeks — the standard prescription antibiotic for SIBO
- Herbal antimicrobials — two commercial blends were used: Dysbiocide + FC Cidal (Biotics Research) or Candibactin-AR + Candibactin-BR (Metagenics), both containing berberine plus oregano, thyme, sage, and lemon balm essential oil components. Two tablets of each blend, twice daily, for 4 weeks.
The post-treatment results were striking:
- Normalization of lactulose breath test: rifaximin 34%, herbal antimicrobials 46%
- Clinical symptom response: approximately equivalent between the two arms
- Adverse events: 14% in the rifaximin group, 8% in the herbal group
- Cost: herbal regimen approximately $100 for a 4-week course; rifaximin approximately $1,500 for a 14-day course without insurance coverage
The herbal antimicrobials were therefore non-inferior to (and numerically superior to) rifaximin for breath-test normalization, with a better tolerability profile and dramatically lower cost. The trial limitations are real — retrospective design (not RCT), modest sample size, two different herbal blends (not pure berberine), single center — but the signal is strong enough to have changed clinical practice in integrative gastroenterology. Herbal antimicrobials, with berberine as the most-validated component, are now a standard first-line or second-line option for SIBO treatment in many integrative GI clinics.
For the broader SIBO clinical picture and a deeper treatment discussion, see the SIBO main page and the SIBO Treatment Protocols deep-dive.
SIBO — The Condition and Why Antibiotic Resistance Is a Problem
Small intestinal bacterial overgrowth (SIBO) is a condition in which excessive numbers of bacteria colonize the small intestine, where bacterial density should normally be low (the small bowel is designed to be relatively sterile compared to the colon). Diagnostic threshold has historically been >10^5 CFU/mL in jejunal aspirate, although the lactulose breath test (LBT) and glucose breath test (GBT) are the practical clinical tools.
Symptoms are nonspecific but consistent: bloating, postprandial abdominal distension, alternating diarrhea and constipation, excessive gas, food intolerances (particularly to high-FODMAP foods that are fermented by the overgrown bacteria), nutritional deficiencies (B12 from bacterial competition, fat-soluble vitamins from bile acid deconjugation, iron from intestinal inflammation), and weight loss in severe cases. The mechanisms linking small-bowel bacterial overgrowth to symptoms are reasonably well-understood: bacterial fermentation of carbohydrates produces hydrogen and methane gas distending the bowel, bacterial deconjugation of bile acids impairs fat digestion and produces diarrhea, bacterial metabolites including LPS contribute to systemic inflammation.
The standard pharmacologic treatment is the non-absorbable antibiotic rifaximin (Xifaxan) 550 mg three times daily for 14 days. The advantage of rifaximin is that it stays in the gut lumen, achieving high local concentrations without systemic absorption. The disadvantages are:
- Cost — approximately $1,500 per 14-day course without insurance; even with insurance often $200+ copay
- Insurance prior-authorization burden — rifaximin is FDA-approved for IBS with diarrhea and hepatic encephalopathy but not formally for SIBO, so insurance coverage is variable
- Relapse rate — approximately 40-50% of patients relapse within 6-9 months after a single course, requiring repeated treatment
- Emerging resistance — while rifaximin's non-absorption keeps systemic resistance pressure low, gut-flora resistance can develop with repeated courses
- Methane-dominant SIBO — methane producers (formally now reclassified as "intestinal methanogen overgrowth" or IMO) respond poorly to rifaximin monotherapy and typically require combination with neomycin or metronidazole, which adds cost and side effects
This is the niche that berberine fills. As a botanical antimicrobial with a different mechanism than rifaximin, berberine can be used as primary therapy, as second-line after rifaximin failure, as a rotating agent between rifaximin courses to slow resistance development, or in patients without insurance coverage for whom rifaximin is unaffordable.
Berberine's Antimicrobial Spectrum
Berberine has a notably broad antimicrobial spectrum compared to most natural products:
- Gram-positive bacteria — effective against Staphylococcus aureus (including some MRSA strains in vitro), Streptococcus species, Enterococcus species, Clostridium difficile
- Gram-negative bacteria — effective against Escherichia coli (including some enterotoxigenic and enteropathogenic strains), Salmonella species, Shigella species, Vibrio cholerae, Campylobacter jejuni, Helicobacter pylori, Klebsiella pneumoniae
- Yeasts and fungi — effective against Candida albicans, Candida glabrata, Cryptococcus neoformans
- Protozoa — effective against Giardia lamblia, Entamoeba histolytica, Trichomonas vaginalis, Leishmania species
- Viruses — some in vitro activity against influenza, HSV, and others, but the in vivo evidence is limited
The molecular mechanisms underlying this broad-spectrum activity:
- DNA intercalation — berberine inserts between adjacent DNA base pairs, interfering with DNA replication and transcription. This is similar in concept to how some antibiotics (quinolones target DNA gyrase) and chemotherapy agents (doxorubicin intercalates DNA) work.
- FtsZ inhibition — berberine inhibits bacterial FtsZ, the bacterial tubulin homolog that forms the constriction ring during bacterial cell division. Without functional FtsZ, bacteria cannot complete cytokinesis and stop dividing. This mechanism is bactericidal at high concentrations.
- Cell membrane disruption — berberine inserts into bacterial cell membranes, particularly Gram-positive membranes, disrupting membrane integrity and proton motive force.
- Efflux pump inhibition — berberine inhibits bacterial multi-drug efflux pumps (NorA in S. aureus, AcrAB in E. coli), which can resensitize bacteria that have become resistant to conventional antibiotics. This is a particularly interesting property given the antibiotic resistance crisis.
- Quorum sensing disruption — berberine interferes with bacterial cell-to-cell signaling (autoinducers, AI-2), reducing biofilm formation and virulence factor expression.
The multi-mechanism antimicrobial profile is one reason berberine resistance has been slow to develop — bacterial single-step resistance mutations cannot easily overcome five different molecular targets simultaneously.
Berberine for Clostridium difficile Infection
Clostridium difficile (C. diff) infection is one of the most challenging hospital-acquired infections in modern medicine. The standard treatment paradigm has shifted away from metronidazole toward oral vancomycin and fidaxomicin (Dificid), but recurrence rates remain 20-30% after a first episode and rise to 40-60% after a second. The principal driver of recurrence is the destruction of the protective commensal microbiome by the very antibiotics used to treat the infection — a vicious cycle of dysbiosis-driven C. diff overgrowth.
Berberine is mechanistically attractive in C. diff for several reasons:
- Direct in vitro activity against C. difficile at clinically achievable luminal concentrations
- Less destructive to commensal anaerobes (Lactobacillus, Bifidobacterium, Akkermansia) than vancomycin or fidaxomicin, preserving the microbiome scaffold needed for recovery
- Direct inhibition of toxin A and toxin B activity at the intestinal epithelium (the virulence factors that produce the colitis)
- Affordable for long-duration adjunct or maintenance therapy
The clinical evidence is still pilot-stage. Small case series have reported successful use of berberine 500 mg three times daily as adjunct to vancomycin or fidaxomicin during the initial treatment course, then continued as monotherapy for 4-8 weeks after the prescription antibiotic is discontinued, to suppress vegetative C. diff regrowth while the microbiome recovers. This approach has plausibility but lacks large RCT validation. Berberine should not be used as monotherapy for an acute C. diff infection — the standard-of-care antibiotics (vancomycin, fidaxomicin) are first-line and berberine is at most an adjunct.
For more on C. diff and antibiotic-associated diarrhea, see the C. difficile page, or the Probiotics page for microbiome-restoration approaches.
Berberine for Helicobacter pylori
Helicobacter pylori is the bacterial cause of most peptic ulcer disease, chronic gastritis, and gastric MALT lymphoma, and is a class I carcinogen for gastric adenocarcinoma. Standard eradication therapy is bismuth quadruple therapy (PPI + bismuth subsalicylate + metronidazole + tetracycline) or clarithromycin-based triple therapy (PPI + clarithromycin + amoxicillin), each for 10-14 days. Eradication rates have declined over the past two decades as antimicrobial resistance (particularly clarithromycin resistance) has spread, dropping from >90% to 70-80% in many regions.
Berberine has been tested as both adjunct and substitute in H. pylori eradication regimens. Multiple trials in Chinese populations have shown that:
- Berberine + standard triple therapy produces eradication rates approximately 5-10% higher than triple therapy alone
- Berberine + dual therapy (PPI + amoxicillin) approaches the eradication rate of full triple therapy in some trials
- Berberine appears to be active against clarithromycin-resistant H. pylori strains in vitro
- Berberine reduces gastric inflammation and may accelerate symptom resolution
The mechanism is the broad antimicrobial activity discussed above, plus specific effects on the H. pylori urease enzyme (which neutralizes gastric acid to allow H. pylori colonization) and on the CagA virulence factor expression. The use case is most attractive in patients with prior treatment failure, in regions with high clarithromycin resistance, or as adjunct to maximize eradication rates in first-line treatment.
Berberine for Giardia and Other Protozoa
The historical Ayurvedic use of berberine-containing herbs for "amoebic" diarrhea has been validated mechanistically. Berberine has demonstrated activity against:
- Giardia lamblia — the most common protozoal cause of traveler's diarrhea worldwide; berberine produces in vitro killing at concentrations achievable in the gut lumen
- Entamoeba histolytica — the causative agent of amoebic dysentery; berberine has been used clinically in this indication in regions where standard treatment (metronidazole + paromomycin) is unavailable
- Trichomonas vaginalis — topical and oral berberine has been studied
- Leishmania species — in vitro and limited clinical evidence
The clinical positioning is that berberine is generally an adjunct to or alternative for standard antiprotozoal drugs (metronidazole, tinidazole, nitazoxanide, paromomycin) rather than first-line monotherapy in developed-world settings. In resource-limited settings, the cost advantage and the historical experience make berberine a reasonable first-line option for symptomatic protozoal diarrhea.
Berberine for Candida and Yeast Overgrowth
Candida overgrowth (intestinal and systemic) is a contested concept in mainstream medicine but a real clinical entity in many integrative practices, where patients present with bloating, brain fog, sugar cravings, recurrent vaginal yeast infections, and intolerance to fermented foods. The diagnostic certainty is lower than for SIBO (no breath test equivalent), and the diagnosis often relies on a constellation of symptoms plus stool culture or organic acid testing.
Berberine has documented in vitro activity against Candida albicans, Candida glabrata, and several other yeast species, with mechanisms including direct membrane disruption and inhibition of fungal cell wall synthesis. The clinical evidence in human Candida overgrowth is limited (this is true of essentially all interventions for this entity), but the in vitro evidence and clinical experience in integrative GI practice support berberine as a reasonable component of a multi-agent antifungal protocol.
The herbal blends used in the Chedid 2014 SIBO trial (Candibactin, Dysbiocide) were originally formulated for combined bacterial and fungal overgrowth, reflecting the clinical reality that the two often coexist. Berberine plus caprylic acid, oregano oil, and saccharomyces boulardii is a common combination protocol for Candida-and-bacterial dysbiosis in integrative practice.
The Dysbiosis Rotation Protocol
One of the most useful frameworks in chronic dysbiosis management is the "rotation" concept — cycling between multiple antimicrobial agents with different mechanisms to (a) avoid the resistance development that occurs with repeated use of any single agent, (b) achieve broader-spectrum coverage by addressing the different microbial populations that respond to different agents, and (c) reduce the risk of complete commensal collapse that occurs with prolonged single-agent suppression.
A typical rotation protocol for chronic SIBO or chronic dysbiosis might include:
- Round 1 (4 weeks) — rifaximin 550 mg three times daily, plus a low-FODMAP or biphasic diet
- 2-week washout with prokinetic and digestive support
- Round 2 (4 weeks) — berberine 500 mg three times daily plus oregano oil or thyme essential oil capsules
- 2-week washout
- Round 3 (4 weeks) — allicin-based garlic extract plus neem leaf extract, or a different commercial herbal antimicrobial blend
- Maintenance phase — biofilm disruptors (NAC, lactoferrin), prokinetic agents (low-dose naltrexone, prucalopride, ginger), probiotic re-seeding (multi-strain probiotic plus saccharomyces boulardii)
The rationale for rotation is mechanistic: berberine and rifaximin have entirely different mechanisms (DNA intercalation + FtsZ inhibition + efflux pump inhibition vs RNA polymerase inhibition), so a bacterial population that survives one is unlikely to survive the other. Repeated single-agent treatment selects for resistant subpopulations; rotation prevents this selection pressure from building.
Berberine's role in the rotation is as a broad-spectrum component that covers both bacteria and yeast, and as a low-cost option that doesn't blow through insurance benefits the way repeated rifaximin courses do. The combination with a complementary herbal agent (oregano oil, allicin) maximizes the spectrum.
For more on dysbiosis and integrative gut management, see the Gut Healing page.
Berberine's Effect on the Beneficial Microbiome
A key question with any antimicrobial used long-term is the collateral damage to beneficial commensals. The available evidence suggests berberine has a more favorable profile than broad-spectrum systemic antibiotics:
- Akkermansia muciniphila — this beneficial mucin-degrading bacterium, considered a marker of healthy gut barrier function, has been shown to increase with berberine treatment in both rodent models and human studies. This is one of the most distinctive microbiome signatures of berberine.
- Bifidobacterium and Lactobacillus — effects are mixed; some studies show no change, some show modest decreases that recover with co-administration of probiotics
- Short-chain fatty acid producers — Faecalibacterium prausnitzii, Roseburia, and other butyrate producers generally show stable-to-increased abundance on berberine, in contrast to the suppression seen with broad-spectrum systemic antibiotics
- Lipopolysaccharide-producing Gram-negatives — decreased, which contributes to the reduced metabolic endotoxemia that drives some of berberine's systemic metabolic benefits
- Overall alpha diversity — generally preserved or modestly reduced; the dramatic loss of diversity that follows fluoroquinolone or amoxicillin-clavulanate courses is not seen with berberine
The mechanism for this relatively benign profile appears to be that berberine's antimicrobial activity is most potent against pathobionts and overgrowth-associated organisms while sparing the dominant commensals. Whether this reflects intrinsic species-level differences in berberine sensitivity, ecological dynamics (overgrowth organisms are more metabolically active and therefore more susceptible to FtsZ inhibition), or both, is not fully resolved.
The practical implication is that berberine is more compatible with concurrent probiotic use than systemic antibiotics are — the probiotic dose and the berberine dose can be taken at the same time of day without significant interference, although many clinicians recommend separating by 2 hours as a conservative approach.
Practical Protocol for SIBO Eradication
A typical berberine-based SIBO eradication protocol:
- Diagnostic confirmation — lactulose breath test (LBT) or glucose breath test (GBT) to confirm SIBO and distinguish hydrogen-dominant, methane-dominant (IMO), or mixed
- Pre-treatment preparation (1 week) — start a low-FODMAP or biphasic diet to reduce substrate for the overgrown bacteria; begin a digestive enzyme + ox bile combination with each meal; begin a prokinetic at bedtime (ginger 1,000 mg, low-dose naltrexone 2.5-4.5 mg, or 5-HTP 50-100 mg)
- Antimicrobial phase (4 weeks) —
- Berberine 500 mg three times daily with meals
- Plus oregano oil capsule (containing approximately 200 mg standardized to 60%+ carvacrol) twice daily with meals, OR
- Plus a commercial herbal antimicrobial blend (Candibactin-AR + Candibactin-BR, or Dysbiocide + FC Cidal)
- For methane-dominant SIBO, add allicin (Allimax or similar enteric-coated garlic extract) 450 mg twice daily, since methanogens are particularly resistant to most antimicrobials and allicin has unique activity against archaea
- Biofilm disruption (concurrent) — N-acetylcysteine 600 mg twice daily, plus a biofilm-disruptor enzyme blend (e.g., Interphase Plus, Biofase) 30 minutes before each antimicrobial dose. The rationale is that bacteria in biofilms are 100-1,000× more resistant to antimicrobials than planktonic bacteria, and disrupting biofilms exposes them to berberine.
- Post-antimicrobial reseeding (2 weeks) — multi-strain probiotic with at least 25 billion CFU/day plus Saccharomyces boulardii 5-10 billion CFU/day, taken at least 2 hours apart from any remaining antimicrobial doses
- Maintenance phase (3-6 months) — continued prokinetic (LDN or ginger nightly), continued low-FODMAP or modified-Mediterranean diet, periodic re-treatment with berberine 500 mg twice daily for 7-10 days at first sign of symptom recurrence
- Re-test at 6 weeks post-antimicrobial — repeat LBT to confirm eradication. If still positive, second round with a different rotation (rifaximin if not yet used, or different herbal blend) is reasonable.
For deeper protocol details, see the SIBO main page and the relevant sub-articles in the SIBO deep-dive hub.
Aftercare — Preventing Relapse
The single most important fact about SIBO is the high relapse rate. Approximately 40-50% of patients who achieve initial eradication will relapse within 6-9 months without ongoing prokinetic and dietary management. Berberine's role in relapse prevention:
- Periodic short-course retreatment — rather than waiting for full symptom recurrence and a full breath-test relapse, many patients do well with a 7-10 day course of berberine 500 mg twice daily at the first sign of recurring bloating or distention. This "punctuated maintenance" approach can extend the time between full treatment rounds substantially.
- Continuous low-dose maintenance — some clinicians use berberine 500 mg once daily continuously as part of long-term maintenance in patients with frequent relapse. The safety data out to 24 months are reassuring, although longer-term continuous use has not been formally studied.
- Combination with prokinetic — the underlying driver of SIBO relapse is usually impaired migrating motor complex (MMC) function in the small intestine. Berberine does not directly fix the MMC; prokinetic agents (LDN, prucalopride, ginger, mosapride, 5-HTP) do. Berberine periodic retreatment plus continuous prokinetic is the most effective combination.
For the SIBO relapse-prevention discussion in detail, see the SIBO Prokinetics and Relapse Prevention deep-dive.
Key Research Papers
- Chedid V, Dhalla S, Clarke JO, et al. (2014). Herbal therapy is equivalent to rifaximin for the treatment of small intestinal bacterial overgrowth. Global Advances in Health and Medicine 3(3):16-24. — PubMed
- Rabbani GH, Butler T, Knight J, et al. (1987). Randomized controlled trial of berberine sulfate therapy for diarrhea due to enterotoxigenic Escherichia coli and Vibrio cholerae. Journal of Infectious Diseases. — PubMed
- Sun D, Courtney HS, Beachey EH (1988). Berberine sulfate blocks adherence of Streptococcus pyogenes to epithelial cells, fibronectin, and hexadecane. Antimicrobial Agents and Chemotherapy. — PubMed
- Domadia PN, Bhunia A, Sivaraman J, et al. (2008). Berberine targets assembly of Escherichia coli cell division protein FtsZ. Biochemistry. — PubMed
- Stermitz FR, Lorenz P, Tawara JN, et al. (2000). Synergy in a medicinal plant: antimicrobial action of berberine potentiated by 5'-methoxyhydnocarpin, a multidrug pump inhibitor. PNAS. — PubMed
- Bandyopadhyay S, Patra PH, Mahanti A, et al. (2013). Potential antibacterial activity of berberine against multi drug resistant enterovirulent Escherichia coli isolated from yaks. Asian Pacific Journal of Tropical Medicine. — PubMed
- Tan W, Li Y, Chen M, Wang Y (2011). Berberine hydrochloride: anticancer activity and nanoparticulate delivery system. International Journal of Nanomedicine. — PubMed
- Sack RB, Froehlich JL (1982). Berberine inhibits intestinal secretory response of Vibrio cholerae and Escherichia coli enterotoxins. Infection and Immunity. — PubMed
- Hu Q, Peng Z, Li L, et al. (2018). The efficacy of berberine-containing quadruple therapy on Helicobacter pylori eradication in China: a systematic review and meta-analysis of randomized clinical trials. Frontiers in Pharmacology. — PubMed
- Zhang X, Zhao Y, Zhang M, et al. (2012). Structural changes of gut microbiota during berberine-mediated prevention of obesity and insulin resistance in high-fat diet-fed rats. PLoS One. — PubMed
- Wang Y, Tong Q, Shou JW, et al. (2017). Gut microbiota-mediated personalized treatment of hyperlipidemia using berberine. Theranostics. — PubMed
- Sun R, Yang N, Kong B, et al. (2017). Orally administered berberine modulates hepatic lipid metabolism by altering microbial bile acid metabolism and the intestinal FXR signaling pathway. Molecular Pharmacology. — PubMed
PubMed Topic Searches
- PubMed: Berberine and SIBO
- PubMed: Berberine and C. difficile
- PubMed: Berberine and H. pylori
- PubMed: Berberine and microbiome
- PubMed: Berberine antimicrobial spectrum
- PubMed: Berberine and Candida
Connections
- Berberine Overview
- Berberine Benefits Hub
- Berberine for Blood Sugar
- Berberine for Cholesterol
- Berberine, AMPK & Metabolic Syndrome
- SIBO (Main Page)
- Gastroenterology Conditions
- Gut Healing
- Probiotics
- Oregano Oil
- Garlic / Allicin
- Goldenseal (Berberine Source)
- Barberry (Berberine Source)
- Elimination Diet / Low-FODMAP
- Ginger (Prokinetic)
- All Herbs