Berberine for Cholesterol & Lipid Metabolism
The 2004 Kong paper in Nature Medicine changed the scientific status of berberine in one publication. Until then, berberine was widely regarded as an antimicrobial folk remedy with some experimental glucose effects. The Kong group at Beijing Genomics Institute showed that berberine produces approximately 29% LDL cholesterol reduction in humans through a previously uncharacterized mechanism — hepatic LDL-receptor mRNA stabilization. This is fundamentally different from how statins work (statins inhibit HMG-CoA reductase to reduce cholesterol synthesis) and explains why the combination of berberine plus statin produces larger LDL reductions than either alone. The downstream consequences are also distinct from statins: berberine produces meaningful triglyceride reductions (statins are weak on triglycerides), modest HDL increases (statins are mostly neutral), and no muscle pain or rhabdomyolysis (the statin-class side effect that drives 10-20% discontinuation). This deep-dive walks through the Kong 2004 mechanism, the comparative efficacy with statins, the use case for statin-intolerant patients, the rationale for combination therapy in resistant hyperlipidemia, and the relevance for patients with concurrent diabetes or metabolic syndrome where the multi-target profile is especially useful.
Table of Contents
- Kong 2004 — The Nature Medicine Paper That Changed Berberine's Status
- The LDL-Receptor Upregulation Mechanism
- Berberine vs Statins — Different Mechanism, Comparable Magnitude
- The Dual AMPK + LDLR Pathway
- Effect on Triglycerides (Where Berberine Beats Statins)
- Effect on HDL Cholesterol
- Use in Statin-Intolerant Patients
- Berberine + Statin Combination Therapy
- Effect on Atherosclerosis and Cardiovascular Endpoints
- Practical Dosing for Lipid Indications
- Monitoring Lipids on Berberine
- Key Research Papers
- Connections
- Featured Videos
Kong 2004 — The Nature Medicine Paper That Changed Berberine's Status
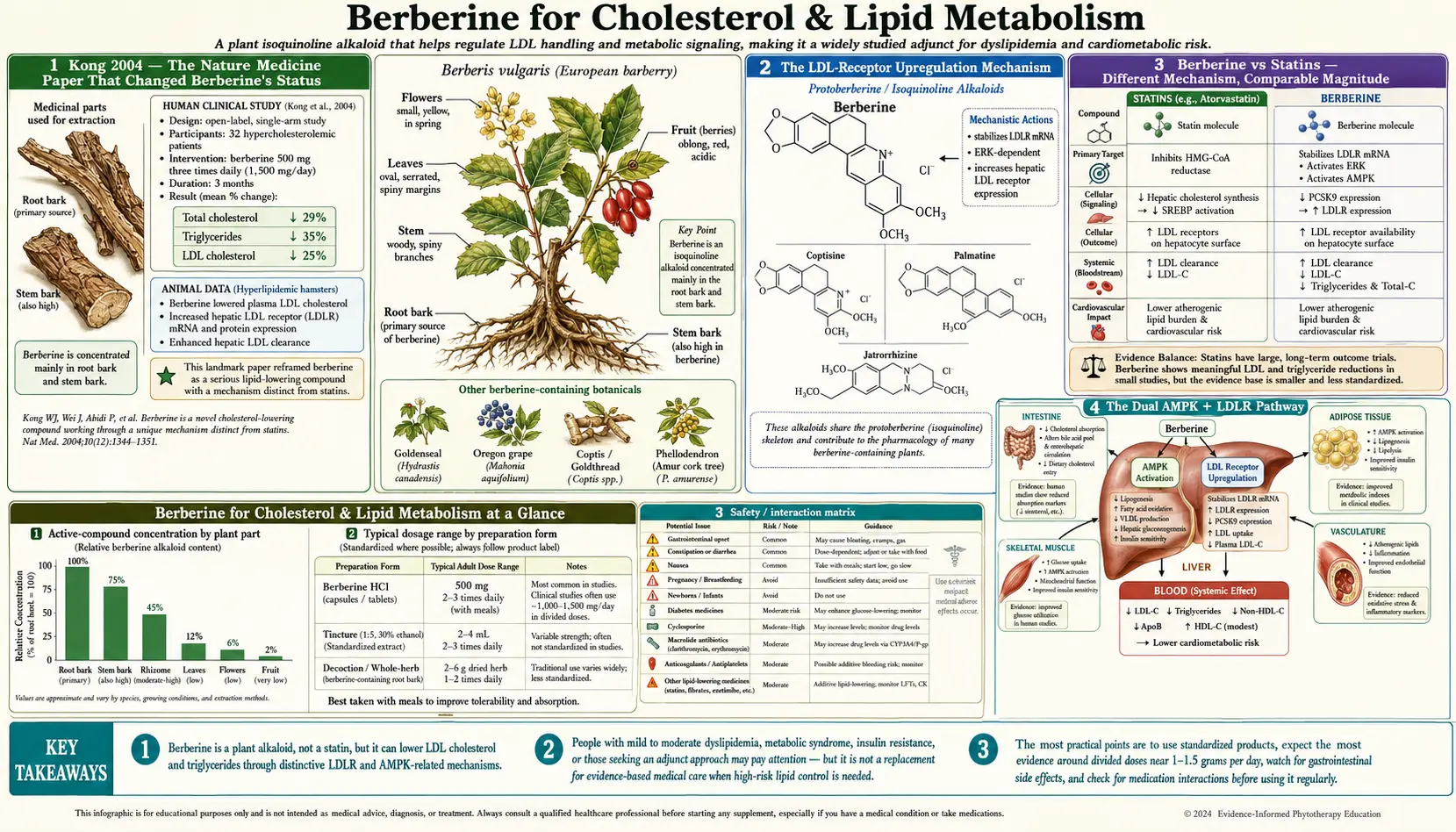
The 2004 Kong, Wei, Abidi, Lin, et al. paper in Nature Medicine titled "Berberine is a novel cholesterol-lowering drug working through a unique mechanism distinct from statins" is the single most important publication in modern berberine pharmacology. The investigators conducted both mechanistic in vitro studies and a clinical pilot:
- In vitro mechanism work — Berberine, applied to cultured hepatocytes (HepG2 cells, the standard human hepatoma cell line for lipid research), dramatically upregulated LDL-receptor protein expression on the cell surface, increased LDL particle uptake from the culture medium, and stabilized LDL-receptor mRNA against rapid degradation. The mechanism was traced to ERK (extracellular signal-regulated kinase) signaling that stabilizes the 3' untranslated region of the LDLR mRNA, increasing its half-life and steady-state level.
- Animal validation — In hyperlipidemic hamsters, oral berberine produced significant LDL reductions that paralleled the in vitro findings.
- Clinical pilot — 32 hyperlipidemic patients were treated with berberine 500 mg twice daily for 3 months. Results:
- Serum cholesterol reduced by 29%
- LDL cholesterol reduced by 25%
- Triglycerides reduced by 35%
- Hepatic LDL-receptor expression was confirmed elevated in patient liver biopsies
The publication in Nature Medicine — one of the highest-impact medical journals in the world — gave berberine a status it had not previously had in Western medicine. It demonstrated that (a) berberine produces clinically meaningful lipid effects in humans, (b) the mechanism is novel and distinct from statins, and (c) the molecular target (LDL-receptor mRNA stabilization) is a legitimate druggable pathway worthy of further investigation. The paper has been cited over 1,500 times in the subsequent two decades.
The clinical pilot is small (n=32) and was followed by larger studies confirming the effect size; modern meta-analyses pool many such trials and converge on approximately 20-25% LDL reduction with berberine monotherapy in hyperlipidemic patients — somewhat lower than the original 29% figure but still clinically meaningful and comparable to a moderate-dose statin.
The LDL-Receptor Upregulation Mechanism
To understand why berberine's mechanism is novel, a brief refresher on LDL metabolism is helpful. Circulating LDL cholesterol is cleared primarily by hepatic LDL receptors, which bind LDL particles via apolipoprotein B and internalize them for degradation in lysosomes. The number of LDL receptors on the hepatocyte surface is the principal determinant of how fast LDL is cleared from the bloodstream — more receptors equals faster clearance equals lower circulating LDL.
The amount of LDL-receptor mRNA in the hepatocyte determines how much LDL-receptor protein is synthesized, which determines how many receptors reach the cell surface. The LDLR mRNA is normally quite unstable — it has a short half-life and is rapidly degraded by ribonucleases that recognize its 3' untranslated region. This rapid turnover is a regulatory feature, not a bug; it allows hepatocyte LDLR expression to respond rapidly to changing cholesterol demand.
Berberine acts on this regulatory step. By activating ERK signaling (one of the MAP kinase pathways), berberine stabilizes the LDLR mRNA against degradation. The mRNA half-life is extended, the steady-state mRNA level increases, more LDL-receptor protein is synthesized, more receptors reach the cell surface, and more LDL is cleared from circulation. The net effect is reduced serum LDL — the same outcome as a statin but achieved by an entirely different route.
The mechanism has some appealing features:
- It does not deplete intracellular cholesterol (statins do, which has been hypothesized to contribute to statin side effects via depletion of mevalonate-pathway intermediates like coenzyme Q10 and dolichol)
- It does not interfere with the mevalonate pathway products that statins block (coenzyme Q10, dolichol, geranylgeraniol pyrophosphate). This explains the absence of statin-class muscle and energy-metabolism side effects.
- It is additive with statins because the two mechanisms target different steps in the same overall pathway (clearance vs synthesis)
- It is independent of the PCSK9 / LDLR turnover pathway that the modern PCSK9 inhibitor monoclonal antibodies (alirocumab, evolocumab) target
For more on the LDL receptor and cardiovascular pathophysiology, see the Atherosclerosis page.
Berberine vs Statins — Different Mechanism, Comparable Magnitude
The fair comparison between berberine and statins on lipid endpoints:
- LDL reduction — berberine: approximately 20-25% in monotherapy. Atorvastatin 10 mg: approximately 35-40%. Atorvastatin 40 mg: approximately 50%. Rosuvastatin 20 mg: approximately 50-55%. Statins are stronger LDL reducers at moderate-to-high doses, but berberine is comparable to a low-dose statin (e.g., atorvastatin 5 mg, rosuvastatin 5 mg, or pravastatin 20 mg).
- Triglyceride reduction — berberine: approximately 25-35%. Statins: approximately 10-20%. Berberine wins on triglycerides. This is one of the few areas where a botanical agent outperforms a major drug class on a hard biomarker.
- HDL cholesterol — berberine: modest increase of 5-10%. Statins: mostly neutral, some have small effect. Roughly equivalent.
- Apolipoprotein B — berberine: reduced. Statins: reduced more. Statins win.
- Lipoprotein(a) — berberine: small reduction. Statins: mostly neutral or slight increase. Berberine has a small edge.
- hs-CRP (inflammation marker) — berberine: reduces. Statins: reduce (the Jupiter trial showed this is independent of LDL reduction). Roughly equivalent.
The cardiovascular hard-outcome evidence is enormously larger for statins. The 4S, WOSCOPS, AFCAPS/TexCAPS, HPS, ASCOT, JUPITER, IDEAL, and dozens of other landmark statin trials have established beyond reasonable doubt that statins reduce myocardial infarction, stroke, cardiovascular mortality, and (in secondary prevention) all-cause mortality. Berberine has no equivalent hard-outcome trial base — the evidence is primarily on biomarkers (LDL, triglycerides, hs-CRP) rather than on heart attack and death.
This is not an argument against berberine; it is an argument for being honest about what we know and what we don't. The biomarker improvements with berberine are large enough that the cardiovascular hard outcomes are likely to translate, but the formal trial evidence is not there. For high-risk secondary prevention patients (post-MI, post-stroke, established peripheral artery disease), statins should remain first-line. For primary prevention patients with moderately elevated LDL and competing concerns about statin tolerability, berberine is a reasonable alternative or adjunct.
The Dual AMPK + LDLR Pathway
Berberine's lipid effect is not purely LDL-receptor-mediated. The AMPK activation that drives the glycemic effect also has direct lipid consequences:
- AMPK inhibits acetyl-CoA carboxylase, which reduces fatty acid synthesis and increases fatty acid oxidation in the liver. This contributes to reduced hepatic triglyceride synthesis and VLDL secretion.
- AMPK inhibits HMG-CoA reductase indirectly through inhibition of SREBP (sterol regulatory element-binding protein) processing. This is a partial overlap with the statin mechanism — both reduce HMG-CoA reductase activity, but through different upstream paths.
- AMPK reduces de novo lipogenesis in the liver, which is particularly relevant in non-alcoholic fatty liver disease (NAFLD) — see the AMPK and Metabolic Syndrome deep-dive.
So berberine produces three converging lipid-lowering effects:
- LDL clearance ↑ via LDL-receptor mRNA stabilization (the Kong mechanism)
- Hepatic cholesterol synthesis ↓ via partial AMPK-mediated reduction in HMG-CoA reductase activity
- Hepatic triglyceride synthesis ↓ via AMPK inhibition of acetyl-CoA carboxylase
This multi-mechanism profile is why berberine's lipid effect is broader than a statin's (LDL plus triglycerides plus modest HDL increase) and why it is meaningfully additive with statins (the LDLR mechanism complements rather than duplicates the HMG-CoA reductase inhibition). The triglyceride effect in particular is mechanistically distinct from the LDL effect, which is why berberine is often a useful add-on in patients with combined hyperlipidemia (elevated LDL and elevated triglycerides) where statins alone are insufficient.
Effect on Triglycerides (Where Berberine Beats Statins)
Triglyceride elevations are increasingly recognized as a significant cardiovascular risk factor, particularly in patients with metabolic syndrome, diabetes, and insulin resistance. The treatment options for hypertriglyceridemia have historically been:
- Lifestyle (weight loss, alcohol reduction, low-carb diet) — effective but hard to sustain
- Omega-3 fatty acids (high-dose EPA/DHA, particularly icosapent ethyl / Vascepa) — expensive at prescription doses
- Fibrates (gemfibrozil, fenofibrate) — effective but with significant drug interactions and rare hepatotoxicity
- Niacin (vitamin B3 in pharmacologic doses) — effective but with flushing and other side effects that limit tolerability
- Statins — weak on triglycerides (10-20% reduction in modest hypertriglyceridemia)
Berberine's 25-35% triglyceride reduction in meta-analytic data places it in the same effective range as fibrates and niacin, with a generally better tolerability profile than either. The Kong 2004 clinical pilot reported 35% triglyceride reduction; the Dong 2012 and Lan 2015 meta-analyses pooled trials and converged on approximately 25-30% triglyceride reduction with monotherapy.
This makes berberine a particularly attractive option for patients with:
- Mild-to-moderate hypertriglyceridemia (200-500 mg/dL)
- Concurrent insulin resistance or type 2 diabetes (where the glycemic benefit is also valuable)
- Combined hyperlipidemia (elevated LDL and elevated triglycerides) where a single agent addressing both is appealing
- NAFLD (where hepatic triglyceride accumulation is a key pathologic feature)
For severe hypertriglyceridemia (>500 mg/dL) with risk of pancreatitis, berberine is not a substitute for prescription fibrate or icosapent ethyl — the effect size is insufficient and the consequences of failure are severe. Berberine has a role for mild-to-moderate cases and as adjunct to prescription therapy in resistant cases.
Effect on HDL Cholesterol
HDL cholesterol effects of berberine are modest and somewhat inconsistent across trials. The pooled meta-analytic estimate is approximately 5-10% HDL increase, which is in the same range as the modest HDL effects of statins and fibrates. The clinical significance is debatable — the CETP inhibitor failures (anacetrapib, dalcetrapib) have shown that raising HDL pharmacologically does not necessarily reduce cardiovascular events, suggesting that the HDL level may be more of a marker than a target.
The mechanistic basis for the HDL increase is unclear. Possibilities include modest reverse cholesterol transport stimulation, reduced CETP activity (cholesteryl ester transfer protein, which transfers cholesterol esters from HDL to other lipoproteins), and indirect effects from improved insulin sensitivity (low HDL is a feature of insulin resistance, and improving insulin sensitivity tends to modestly raise HDL).
The practical guidance is to not expect dramatic HDL increases from berberine; if dramatic HDL changes are the goal, lifestyle (exercise, weight loss, moderate alcohol) and high-dose niacin are more effective tools. Berberine's lipid value lies in LDL and triglyceride reduction, not in HDL elevation.
Use in Statin-Intolerant Patients
Statin intolerance is one of the most common and most clinically important problems in lipid management. The literature estimates range from 5% to 20% of patients started on statins discontinue due to side effects — primarily statin-associated muscle symptoms (myalgia, weakness, sometimes elevated CK), but also brain fog, fatigue, and gastrointestinal symptoms. The mechanism of statin side effects is debated but is thought to involve depletion of mevalonate-pathway intermediates including coenzyme Q10, dolichol, geranylgeraniol pyrophosphate, and possibly impaired mitochondrial function.
Berberine is mechanistically attractive for statin-intolerant patients because:
- It does not inhibit HMG-CoA reductase, so the mevalonate pathway intermediates that statins deplete are unaffected
- Muscle pain and weakness are not characteristic side effects of berberine (the primary berberine side effects are GI — see the blood sugar deep-dive for management)
- It produces lipid effects in the same general magnitude as a low-to-moderate dose statin
- It has additional metabolic benefits (glycemic, insulin sensitivity, anti-inflammatory) that statin-intolerant patients with metabolic syndrome especially value
The clinical pathway for a patient who fails statins:
- Confirm statin intolerance — rechallenge with a different statin (hydrophilic statins like pravastatin and rosuvastatin have lower muscle side effect rates than lipophilic statins like simvastatin and lovastatin), at lower doses, every other day, or with coenzyme Q10 co-supplementation
- If second-statin trial also fails, ezetimibe (Zetia) is the conventional next step — 10 mg/day, well-tolerated, produces approximately 18% LDL reduction
- If ezetimibe alone is insufficient, add berberine 500 mg three times daily — the combined effect approaches that of a moderate-dose statin in a non-statin patient
- If still inadequate, add bempedoic acid (Nexletol) — another non-statin LDL-lowering agent with a different mechanism (ACL inhibition)
- If still inadequate, PCSK9 inhibitor monoclonal antibodies (alirocumab, evolocumab) are the next step — expensive but extremely effective
The role for berberine in this pathway is as a bridge between ezetimibe and the more expensive non-statin alternatives. It is well-tolerated, inexpensive, has additional metabolic benefits, and produces enough LDL reduction to be meaningful.
Berberine + Statin Combination Therapy
Several trials have tested berberine added to ongoing statin therapy in patients who have not reached LDL goal. The Kong group's 2008 follow-up trial randomized 63 patients on simvastatin 20 mg/day with inadequate LDL response to either:
- Simvastatin 20 mg alone (continued)
- Simvastatin 20 mg + berberine 500 mg twice daily
The combination arm achieved an additional 17-21% LDL reduction beyond what the statin alone had achieved, with no significant increase in adverse events. The combination produced LDL reductions comparable to doubling the statin dose (which the FDA and most clinical guidelines discourage because the marginal LDL benefit of statin dose-doubling is small and the marginal increase in side effects is significant). Berberine + low-dose statin appears to be a more favorable risk-benefit ratio than high-dose statin alone, although the long-term hard-outcome data to confirm this are not available.
The clinical use case for berberine + statin combination:
- Patient on a low-to-moderate dose statin (atorvastatin 10-20 mg, rosuvastatin 5-10 mg, simvastatin 20 mg)
- LDL above goal (typical secondary prevention goal: <70 mg/dL; primary prevention with risk factors: <100 mg/dL)
- Doubling the statin dose is undesirable for tolerability reasons
- Adding ezetimibe alone has been tried or is insufficient
- Patient prefers a non-prescription adjunct to the next escalation step
Berberine + ezetimibe (with or without statin) is also a reasonable combination because the three mechanisms (intestinal cholesterol absorption inhibition by ezetimibe, hepatic LDLR upregulation by berberine, HMG-CoA reductase inhibition by statin) are entirely non-overlapping and additive.
Effect on Atherosclerosis and Cardiovascular Endpoints
The biomarker improvements with berberine (LDL down 20-25%, triglycerides down 25-35%, hs-CRP down) would be expected to translate to reduced atherosclerosis progression and reduced cardiovascular events, but the direct trial evidence is limited. The available data:
- Carotid intima-media thickness (CIMT) trials in patients with metabolic syndrome have shown reduced CIMT progression on berberine compared to control
- Endothelial function (flow-mediated dilation of the brachial artery) improves on berberine, suggesting improved vascular reactivity
- Arterial stiffness measures (pulse wave velocity) improve modestly
- hs-CRP reductions of 25-30% are consistently reported, in the same range as moderate-dose statins
The hard cardiovascular outcomes (myocardial infarction, stroke, cardiovascular death, all-cause mortality) have not been directly tested in a large, randomized, long-term trial of berberine. This is the principal evidence gap. Until such a trial is done, the cardiovascular case for berberine has to be made indirectly — the biomarker effects are convincing, the mechanism is mechanistically plausible, and the trial-level evidence for analogous biomarker-improving interventions (statins, fibrates, omega-3s) consistently shows hard-outcome benefit when the biomarker is moved in the right direction.
For atherosclerosis-related condition pages, see Atherosclerosis and the broader Cardiology category.
Practical Dosing for Lipid Indications
The standard berberine dose for lipid indications is the same as for glycemic indications: 500 mg three times daily with meals (1,500 mg/day total). There is no good evidence that higher doses produce greater lipid effects, and tolerability declines at higher doses. Key practical points:
- Take with meals. Same rule as for glycemic dosing — food slows absorption, reduces GI side effects, and may improve effect on post-prandial lipemia.
- Allow 3 months for the full lipid effect. LDL changes are typically measurable at 6 weeks but continue to evolve to a steady state by 3 months. Don't check lipids at 4 weeks and conclude the regimen has failed.
- The triglyceride effect may be faster. Triglycerides often respond within 4-6 weeks, before the LDL effect is at maximum.
- Combination with omega-3 fatty acids. Berberine + 2-4 g/day of EPA/DHA omega-3s is a reasonable combination for combined hyperlipidemia. The mechanisms are non-overlapping and the safety profile is excellent.
- Combination with red yeast rice is generally discouraged. Red yeast rice contains naturally occurring monacolin K, which is chemically identical to lovastatin. Combining berberine with red yeast rice essentially creates a statin + berberine combination but with much less quality control. If statin-class effect is desired, use an actual prescription statin.
- Don't expect dramatic results in patients with familial hypercholesterolemia. Patients with genetically defective LDL receptors (heterozygous or homozygous FH) have a structural problem that berberine's LDLR upregulation cannot fully compensate for. These patients need statins, ezetimibe, and frequently PCSK9 inhibitors.
Monitoring Lipids on Berberine
The recommended lipid monitoring schedule on berberine:
- Baseline — full lipid panel (total cholesterol, LDL, HDL, triglycerides), liver function (AST, ALT), basic metabolic panel. If concurrent diabetes or prediabetes: HbA1c and fasting insulin.
- 3 months — recheck lipid panel. LDL reduction should be 15-25%, triglyceride reduction 20-35% if working. If no measurable response at 3 months, troubleshoot adherence and dosing before concluding berberine has failed.
- 6 months — recheck lipid panel, liver function. Confirm sustained effect.
- Annually — lipid panel and liver function. Long-term safety data are reassuring out to 24 months; longer-term data are limited but not concerning.
The relevant lab pages:
- Lipid Panel — the standard total/LDL/HDL/triglyceride measurements
- Hemoglobin A1C — if concurrent diabetes is being managed
- Fasting Insulin — for HOMA-IR calculation and insulin resistance tracking
Liver function should be monitored because berberine is hepatically metabolized. Mild transient transaminase elevations have been reported occasionally; clinically significant hepatotoxicity is rare. If AST or ALT rise to more than 3× the upper limit of normal, discontinue and recheck.
Key Research Papers
- Kong W, Wei J, Abidi P, et al. (2004). Berberine is a novel cholesterol-lowering drug working through a unique mechanism distinct from statins. Nature Medicine 10(12):1344-1351. — PubMed
- Abidi P, Zhou Y, Jiang JD, Liu J (2005). Extracellular signal-regulated kinase-dependent stabilization of hepatic low-density lipoprotein receptor mRNA by herbal medicine berberine. Arteriosclerosis, Thrombosis, and Vascular Biology. — PubMed
- Kong WJ, Wei J, Zuo ZY, et al. (2008). Combination of simvastatin with berberine improves the lipid-lowering efficacy. Metabolism. — PubMed
- Lan J, Zhao Y, Dong F, et al. (2015). Meta-analysis of the effect and safety of berberine in the treatment of type 2 diabetes mellitus, hyperlipidemia and hypertension. Journal of Ethnopharmacology. — PubMed
- Dong H, Zhao Y, Zhao L, Lu F (2013). The effects of berberine on blood lipids: a systematic review and meta-analysis of randomized controlled trials. Planta Medica. — PubMed
- Pirillo A, Catapano AL (2015). Berberine, a plant alkaloid with lipid- and glucose-lowering properties: from in vitro evidence to clinical studies. Atherosclerosis. — PubMed
- Hu Y, Ehli EA, Kittelsrud J, et al. (2012). Lipid-lowering effect of berberine in human subjects and rats. Phytomedicine. — PubMed
- Cameron J, Ranheim T, Kulseth MA, et al. (2008). Berberine decreases PCSK9 expression in HepG2 cells. Atherosclerosis. — PubMed
- Wang Y, Yi X, Ghanam K, Zhang S, Zhao T, Zhu X (2014). Berberine decreases cholesterol levels in rats through multiple mechanisms. Atherosclerosis. — PubMed
- Marazzi G, Cacciotti L, Pelliccia F, et al. (2011). Long-term effects of nutraceuticals on the cholesterol-lowering effect in patients intolerant to statins. Advances in Therapy. — PubMed
- Affuso F, Mercurio V, Fazio V, Fazio S (2010). Cardiovascular and metabolic effects of berberine. World Journal of Cardiology. — PubMed
- Koppen LM, Whitaker A, Rosene A, Beckett RD (2017). Efficacy of berberine alone and in combination for the treatment of hyperlipidemia: a systematic review. Journal of Evidence-Based Complementary & Alternative Medicine. — PubMed
PubMed Topic Searches
- PubMed: Berberine LDL lowering
- PubMed: Berberine + statin combination
- PubMed: Berberine triglycerides
- PubMed: Berberine LDLR mRNA
- PubMed: Berberine statin-intolerant
- PubMed: Berberine atherosclerosis
Connections
- Berberine Overview
- Berberine Benefits Hub
- Berberine for Blood Sugar
- Berberine for Gut Health & SIBO
- Berberine, AMPK & Metabolic Syndrome
- Lipid Panel
- Hemoglobin A1C
- Atherosclerosis
- Cardiology Conditions
- Metabolic Syndrome
- Diabetes
- Non-Alcoholic Fatty Liver Disease
- Omega-3 Fatty Acids
- Barberry (Berberine Source)
- Goldenseal (Berberine Source)
- Blood Sugar
- All Herbs