Berberine for Blood Sugar & Glycemic Control
Berberine is the most-studied herbal compound for type 2 diabetes management, with the central trial — Yin, Xing, and Ye 2008 in Metabolism — demonstrating that berberine 500 mg three times daily produces a 0.9% HbA1c reduction at three months that is statistically indistinguishable from metformin 500 mg three times daily. Two large meta-analyses (Dong 2012, Lan 2015) have since pooled the evidence from over 25 randomized trials and confirmed the effect size. The mechanism is shared with metformin (AMPK activation) plus several additional pathways (GLUT4 translocation, modest DPP-4 inhibition, microbiome modulation), which has earned berberine the popular nickname "nature's metformin." This deep-dive walks through the evidence, the dosing logic, the management of the predictable transient GI side effects, the practical use cases (metformin intolerance, prediabetes, adjunct to metformin), and the critical limitations including bioavailability, drug interactions, and the absolute contraindication in pregnancy.
Table of Contents
- The Yin 2008 Trial — Berberine vs Metformin Head-to-Head
- Lan 2015 & Dong 2012 Meta-Analyses
- AMPK — The Shared Mechanism With Metformin
- Beyond AMPK — GLUT4, DPP-4, and Microbiome
- "Nature's Metformin" — What the Nickname Gets Right and Wrong
- Practical Dosing — 500 mg Three Times Daily With Meals
- GI Side Effects and How to Mitigate Them
- Clinical Use Cases — Who Benefits Most
- Berberine for Prediabetes and Impaired Glucose Tolerance
- Drug Interactions and Contraindications
- Monitoring — HbA1c, Fasting Glucose, and Fasting Insulin
- Key Research Papers
- Connections
- Featured Videos
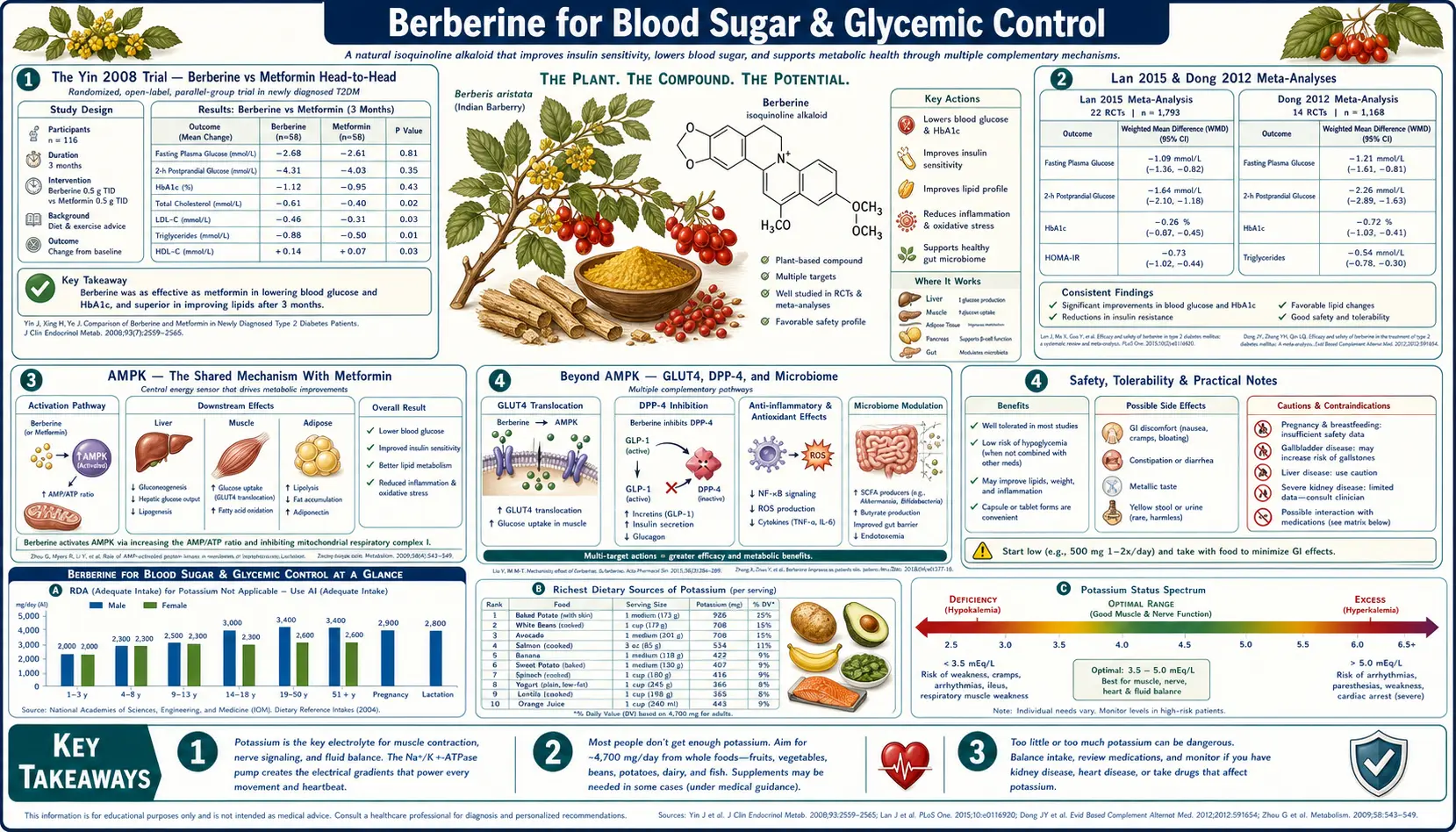
The Yin 2008 Trial — Berberine vs Metformin Head-to-Head
The 2008 Yin trial published in Metabolism is the single most-cited piece of clinical evidence for berberine in type 2 diabetes. The investigators enrolled 36 newly diagnosed patients with type 2 diabetes mellitus at the Beijing Friendship Hospital and randomized them to either:
- Berberine 500 mg three times daily before meals (1,500 mg/day total)
- Metformin 500 mg three times daily before meals (1,500 mg/day total)
After three months of treatment, the results were strikingly similar between groups:
- HbA1c reduction — berberine reduced HbA1c by 2.0% (from 9.5% to 7.5%), metformin reduced it by 1.8%. Both were statistically significant against baseline; the between-group difference was not statistically significant.
- Fasting plasma glucose — berberine reduced FPG from 10.6 to 6.9 mmol/L; metformin reduced it from 10.8 to 6.6 mmol/L. Again, equivalent.
- Postprandial plasma glucose — equivalent reductions in both arms.
- Triglycerides — berberine reduced triglycerides significantly more than metformin (a finding consistent with berberine's additional lipid mechanism — see the cholesterol deep-dive).
- Side effects — both groups had transient GI complaints (diarrhea, abdominal cramping). The berberine group had slightly higher GI symptom rates in the first two weeks, then declined to comparable levels.
The trial is small (n=36) and was conducted at a single Chinese center, so it should not be over-interpreted in isolation. But it established the proof-of-concept that berberine is in the same therapeutic class as metformin for glycemic control, and it provided the dosing template (500 mg TID with meals) that essentially every subsequent berberine diabetes trial has followed.
A common patient question is "if berberine equals metformin, why isn't it the first-line drug?" The honest answer is that the trial base for metformin is enormously larger (the UK Prospective Diabetes Study alone enrolled over 5,000 patients with 20-year follow-up), metformin is FDA-approved with a known safety profile across millions of patient-years, metformin is inexpensive ($4/month at most U.S. pharmacies), and metformin's daily pill burden is lower (twice daily extended-release vs three times daily for berberine). Berberine is best understood not as a replacement for metformin but as a viable alternative for patients who cannot take metformin and as a potential adjunct in patients who need additional glycemic effect on top of metformin.
Lan 2015 & Dong 2012 Meta-Analyses
Two large meta-analyses have now pooled the berberine-for-diabetes trial evidence and confirmed the Yin 2008 effect size. The Dong et al. 2012 systematic review in Evidence-Based Complementary and Alternative Medicine pooled 14 trials with 1,068 participants and reported:
- HbA1c reduction: weighted mean difference -0.71% (95% CI -1.04 to -0.39, p<0.001) compared to placebo or lifestyle alone
- Fasting plasma glucose reduction: weighted mean difference -0.84 mmol/L (p<0.001)
- Postprandial plasma glucose reduction: weighted mean difference -1.32 mmol/L (p<0.001)
- No significant difference in efficacy between berberine alone vs metformin alone, or vs glipizide alone, in head-to-head subgroup analyses
- Combined berberine + metformin produced larger HbA1c reductions than either alone, suggesting additive (non-overlapping) mechanisms in vivo
The Lan et al. 2015 meta-analysis in Journal of Ethnopharmacology pooled 27 trials (2,569 participants) and reached very similar conclusions:
- HbA1c reduction: weighted mean difference approximately -0.7 to -0.9% across analyses
- Fasting glucose reduction: weighted mean difference approximately -0.8 to -1.0 mmol/L
- Berberine was non-inferior to metformin, glipizide, and rosiglitazone in head-to-head comparisons
- Safety profile was favorable — adverse events were predominantly mild GI symptoms, no severe hypoglycemia events were reported (a meaningful advantage over sulfonylureas)
The convergence of two independent meta-analyses on approximately the same effect size — HbA1c reduction of 0.7 to 0.9% — is reassuring. For reference, this is in the same range as most oral diabetes drugs (metformin 1.0-1.5%, sulfonylureas 1.0-2.0%, DPP-4 inhibitors 0.5-0.8%, SGLT2 inhibitors 0.5-1.0%). The qualifier on the meta-analytic evidence is that most underlying trials are Chinese and methodologic quality varies; large Western multi-center trials are still lacking. But the consistency of the signal across trials, mechanisms, and outcome measures makes the glycemic effect one of the best-supported claims in herbal pharmacology.
AMPK — The Shared Mechanism With Metformin
AMP-activated protein kinase (AMPK) is a heterotrimeric enzyme complex that functions as the cellular fuel sensor. When cellular energy is low (the AMP:ATP ratio rises), AMPK is phosphorylated and activated. Once active, AMPK orchestrates a coordinated response to restore energy:
- Increases glucose uptake into cells (via GLUT4 translocation in muscle, GLUT1 elsewhere)
- Increases fatty acid oxidation (via inhibition of acetyl-CoA carboxylase)
- Inhibits fatty acid synthesis and cholesterol synthesis (energy-expensive anabolic pathways)
- Stimulates mitochondrial biogenesis (via PGC-1α)
- Inhibits hepatic gluconeogenesis (the liver's production of new glucose)
- Triggers autophagy (recycling of damaged cellular components for energy)
The net metabolic phenotype of AMPK activation is exactly what a type 2 diabetic patient needs: more glucose uptake into cells, less hepatic glucose output, more fat burning, less fat storage. This is precisely why AMPK is the principal molecular target of metformin — the most prescribed diabetes drug in the world.
Berberine activates AMPK through a different upstream mechanism than metformin (metformin inhibits mitochondrial complex I to raise cellular AMP; berberine appears to act both through a similar mitochondrial inhibition and through direct activation of LKB1, the upstream kinase that phosphorylates AMPK). The downstream consequences, however, are nearly identical, which is why the clinical phenotype — reduced HbA1c, reduced fasting glucose, improved insulin sensitivity — is also nearly identical.
The clinical implication is that berberine and metformin should not be expected to be additive on the AMPK pathway alone. The Dong meta-analysis finding of larger HbA1c reductions with the combination is therefore informative — it suggests that berberine's non-AMPK mechanisms (DPP-4, GLUT4-direct, microbiome) provide the additive benefit. See the AMPK and Metabolic Syndrome page for the broader systemic implications of AMPK activation beyond glucose.
Beyond AMPK — GLUT4, DPP-4, and Microbiome
Berberine's glycemic effect is not purely AMPK-mediated. Three additional mechanisms have been characterized:
GLUT4 translocation — independent of AMPK, berberine appears to directly stimulate translocation of the insulin-responsive glucose transporter GLUT4 from intracellular vesicles to the plasma membrane of skeletal muscle and adipocyte cells. This is the same translocation event that insulin triggers, and it explains why berberine improves insulin sensitivity even in patients with relatively low fasting insulin. The mechanism resembles the effect of exercise on GLUT4 (which is also AMPK-independent in part) and is why some authors describe berberine as an "exercise mimetic" in addition to a metformin mimetic.
Modest DPP-4 inhibition — berberine has measurable inhibitory activity against dipeptidyl peptidase-4 (DPP-4), the enzyme that rapidly degrades the incretin hormones GLP-1 and GIP after they are secreted by intestinal L-cells and K-cells in response to meals. Prescription DPP-4 inhibitors (sitagliptin / Januvia, linagliptin / Tradjenta, saxagliptin / Onglyza) are a well-established diabetes drug class because raising effective GLP-1 levels improves post-prandial glucose control. Berberine's DPP-4 inhibition is modest compared to these prescription agents but contributes additively to its glucose-lowering effect, particularly post-prandial.
Microbiome modulation — this is one of the most exciting recent findings. Berberine, because of its poor systemic bioavailability, exists at high concentrations in the gut lumen, where it directly modifies the gut microbiome. Studies in both rodent models and human patients have shown that berberine shifts the microbial composition toward a phenotype associated with improved glucose metabolism — increased Akkermansia muciniphila, increased short-chain fatty acid producers, decreased lipopolysaccharide-producing Gram-negatives. The reduced metabolic endotoxemia (lower circulating LPS, lower TLR4 signaling) is now thought to account for a meaningful fraction of berberine's glycemic and insulin-sensitivity effects, independent of any direct molecular activity on host enzymes.
The multi-mechanism nature of berberine's glycemic effect is the modern pharmacology explanation for why a single botanical compound can produce effects comparable to several entirely separate drug classes (metformin, gliptins, gliflozins via the microbiome).
"Nature's Metformin" — What the Nickname Gets Right and Wrong
The popular framing of berberine as "nature's metformin" is both informative and misleading. It is informative in the sense that:
- Both compounds activate AMPK as their principal molecular target
- Both reduce HbA1c by approximately the same amount (0.7-0.9%) in head-to-head trials
- Both reduce hepatic gluconeogenesis
- Both improve insulin sensitivity without causing hypoglycemia in monotherapy
- Both have transient GI side effects (diarrhea, cramping, nausea) that resolve with continued use
It is misleading in the sense that:
- Berberine is not a botanical version of metformin chemically — they have entirely different structures (metformin is a synthetic biguanide; berberine is a natural isoquinoline alkaloid). The shared phenotype reflects convergent pharmacology, not chemical resemblance.
- Berberine has additional mechanisms (lipid-lowering via LDLR upregulation, antimicrobial activity, gut-microbiome modulation) that metformin lacks. Some of these are useful, some are simply additional considerations.
- Berberine has a much smaller evidence base for cardiovascular outcomes, all-cause mortality, and cancer prevention than metformin does — metformin has 40+ years of post-marketing data; berberine has perhaps 15 years.
- Berberine costs approximately $20-30/month for a quality product, vs $4-10/month for generic metformin.
- Metformin is FDA-approved as a drug, with manufacturing oversight; berberine is sold as a dietary supplement, with variable third-party verification (NSF, USP, ConsumerLab certifications are recommended).
The fair framing: berberine is a credible alternative to metformin in patients who cannot tolerate metformin (lactic acidosis risk, B12 depletion concern, severe GI intolerance, contrast-imaging interruptions) or who actively prefer a botanical approach, and it can be added as an adjunct in patients on metformin who need additional glycemic effect.
Practical Dosing — 500 mg Three Times Daily With Meals
The standard berberine dose for glycemic control is 500 mg three times daily with meals (1,500 mg/day total). This is the dose used in the Yin 2008 trial and in the majority of subsequent diabetes trials. Practical considerations:
- Take with meals, not on an empty stomach. Food slows absorption and dramatically reduces the GI side effects (cramping, urgent diarrhea) that occur when berberine is taken fasting.
- Three divided doses are important because berberine has a relatively short half-life (approximately 4-5 hours for the parent compound). A single 1,500 mg dose would produce peak-trough fluctuations that reduce efficacy and increase per-dose side effects. Twice-daily dosing (750 mg BID) is a tolerable compromise for patients who cannot manage three doses; some patients find this sufficient.
- Start low and titrate. Begin with 500 mg once daily with the largest meal for 4-7 days. If GI tolerance is acceptable, advance to 500 mg twice daily for another 4-7 days, then to the full 500 mg three times daily. This gradual titration almost completely eliminates the early GI side effects that drive many patients to discontinue.
- Quality matters. Look for products that specify "berberine HCl" (the most-studied salt form) at the labeled dose per capsule (typically 500 mg per capsule). Avoid "berberine complexes" or "berberine blends" that contain less active compound than implied. Third-party certifications (NSF, USP, ConsumerLab) are reassurance of label accuracy.
- Cycling is unnecessary. Some online sources suggest cycling berberine on/off in 3-month intervals to avoid "tolerance." There is no clinical evidence for berberine tolerance — trials have continued daily dosing for 24+ months without loss of effect.
For higher-bioavailability alternatives (dihydroberberine, berberine + sodium caprate), the per-dose amount is lower (typically 100-200 mg dihydroberberine equivalent) but the dosing frequency (three times daily with meals) is the same. There is no convincing trial evidence that these enhanced forms are clinically superior to standard berberine HCl at the standard dose — they may simply allow smaller pills and fewer GI side effects.
GI Side Effects and How to Mitigate Them
The most common and predictable berberine side effect is gastrointestinal — loose stools, cramping, urgency, and occasionally nausea. In the published trials, approximately 30-40% of patients report some GI symptom in the first two weeks, dropping to under 10% after the first month as the gut adapts. The mechanism appears to be a combination of direct osmotic effect on the gut, mild antimicrobial activity altering the microbiome, and stimulation of bile acid secretion.
Practical mitigation strategies, in order of importance:
- Always take with food. The single most important mitigation. Fasted berberine is reliably uncomfortable; berberine taken at the start of a substantial meal is usually fine.
- Titrate up gradually over 2-3 weeks as described above. Starting at the full 1,500 mg/day is the #1 cause of patient discontinuation.
- Hydrate adequately. The osmotic component responds to volume; dehydrated patients tolerate berberine poorly.
- Try a divided pattern — 250 mg with each meal plus 250 mg with a substantial snack, for example, instead of 500 mg three times daily.
- Consider dihydroberberine if standard berberine remains poorly tolerated. The reduced per-dose amount (100-200 mg) often resolves residual GI symptoms.
- Pair with a probiotic in the first month. Berberine's antimicrobial activity is mostly desirable (see the SIBO and gut health deep-dive) but can disrupt commensals transiently; a quality multi-strain probiotic taken at a different time of day than berberine helps with stool consistency.
If GI symptoms persist beyond a month of conservative management, the combination is probably not appropriate for the individual patient. The patient's clinician should be consulted about either dihydroberberine, alternative botanical agents (gymnema, bitter melon, cinnamon), or pharmacologic options.
Clinical Use Cases — Who Benefits Most
The most appropriate clinical use cases for berberine in glycemic management are:
- Metformin-intolerant type 2 diabetics — patients who cannot tolerate metformin due to severe GI symptoms (even after extended-release and gradual titration), B12-depletion concerns, or chronic kidney disease that contraindicates metformin. Berberine produces equivalent glycemic effect with a different side-effect profile and no contraindication in moderate CKD.
- Pre-diabetes / impaired glucose tolerance — patients with HbA1c 5.7-6.4% who want a more aggressive intervention than lifestyle alone but who do not yet meet the threshold for prescription diabetes therapy. Berberine's safety profile and the meta-analytic effect size (approximately 0.5-0.7% HbA1c reduction in this less-advanced population) is well-suited to this use case — see the prediabetes section below.
- Adjunct to metformin in inadequately controlled diabetes — the Dong meta-analysis showed that combined berberine + metformin produces larger HbA1c reductions than either alone. Patients on metformin monotherapy who have HbA1c 7.5-8.5% (above goal but not so high as to require insulin) may be candidates for adding berberine before stepping up to a second prescription drug.
- PCOS with insulin resistance — the Wei 2012 trial in European Journal of Endocrinology showed berberine produced improvements in insulin sensitivity, ovulation rates, and pregnancy outcomes in PCOS patients comparable to metformin. See the AMPK and Metabolic Syndrome page for the PCOS evidence in detail.
- Patients with concurrent dyslipidemia — berberine's additional LDL-receptor mechanism produces meaningful lipid-lowering on top of the glycemic effect. A diabetic patient with HbA1c 7.5% and LDL 140 mg/dL gets a "two-for-one" benefit that pure metformin does not provide. See the cholesterol deep-dive.
- Patients with SIBO or significant gut dysbiosis — the berberine antimicrobial activity is a clinically useful side effect rather than a bug. See the gut health deep-dive.
The use cases where berberine is not the right choice include type 1 diabetes (insulin deficiency, not insulin resistance — berberine has no role here), advanced type 2 diabetes requiring insulin (the effect size is insufficient for severe insulin deficiency), and any pregnant or lactating woman (absolute contraindication — see drug interactions section).
Berberine for Prediabetes and Impaired Glucose Tolerance
Prediabetes (HbA1c 5.7-6.4%, or fasting glucose 100-125 mg/dL, or 2-hour OGTT 140-199 mg/dL) is the most appropriate single use case for berberine in a Western non-diabetic population. The clinical reasoning is straightforward: prediabetes increases the risk of progression to overt diabetes by approximately 10% per year, but most prediabetic patients cannot or will not take prescription metformin (off-label, hard to get insurance coverage for, requires a clinician comfortable with off-label prescribing). Lifestyle intervention (Mediterranean diet, 150 minutes/week of activity, weight loss of 5-7%) is the evidence-based first-line, but only a fraction of patients achieve and sustain the necessary lifestyle change.
Berberine fills the gap. The Yang et al. 2016 trial randomized 105 prediabetic patients to berberine 1,500 mg/day, lifestyle alone, or both, for 24 weeks. Results:
- Berberine + lifestyle achieved the largest HbA1c reduction and the largest reduction in conversion to overt diabetes
- Berberine alone produced approximately 0.6% HbA1c reduction (vs 0.3% with lifestyle alone)
- Fasting insulin and HOMA-IR (a measure of insulin resistance) improved significantly in the berberine arms
- Safety profile was acceptable — transient GI symptoms in the first month, no serious adverse events
The practical protocol for prediabetes:
- Confirm prediabetes with two HbA1c values 5.7-6.4% or two fasting glucose values 100-125 mg/dL
- Implement Mediterranean or low-carb dietary changes simultaneously — berberine is an adjunct to lifestyle, not a substitute
- Begin berberine 500 mg once daily with the largest meal, titrating to 500 mg three times daily over 2-3 weeks
- Recheck HbA1c at 3 months. Effect size should be 0.3-0.7% if working.
- If effect is achieved and tolerated, continue indefinitely. If no effect after 6 months at full dose, discontinue and reconsider.
- Monitor at least annually with HbA1c, fasting glucose, fasting insulin, and lipid panel.
For more on prediabetes and insulin resistance management, see the Insulin Resistance page and the Hemoglobin A1C lab test page.
Drug Interactions and Contraindications
Berberine is a meaningful inhibitor of cytochrome P450 enzymes (CYP2D6, CYP3A4, CYP2C9) and the P-glycoprotein efflux transporter. This produces clinically significant drug interactions:
- Cyclosporine — berberine increases cyclosporine blood levels significantly. Avoid combination in transplant patients on cyclosporine for immunosuppression.
- Macrolide antibiotics (clarithromycin, erythromycin) — potential for additive CYP3A4 interaction and QT prolongation. Avoid combination.
- Warfarin — berberine may increase warfarin effect through CYP2C9 inhibition. INR must be monitored closely if combined.
- Diabetes medications (insulin, sulfonylureas, meglitinides) — additive hypoglycemic effect possible. Patients combining berberine with insulin or sulfonylureas need close glucose monitoring; doses of the prescription agents may need to be reduced.
- SSRIs and other CYP2D6 substrates — berberine may increase serum levels of fluoxetine, paroxetine, venlafaxine, atomoxetine, and other CYP2D6-metabolized drugs. Caution and clinical monitoring required.
- Statins — pharmacokinetic interactions are modest and the pharmacodynamic combination is actually clinically useful (see the cholesterol deep-dive). Combination is reasonable with monitoring.
The absolute contraindications are:
- Pregnancy — berberine displaces bilirubin from albumin and crosses the placenta, with concern for fetal kernicterus, particularly in late pregnancy. Berberine should be avoided throughout pregnancy.
- Lactation — berberine appears in breast milk in measurable quantities. Avoid in breastfeeding mothers; the neonatal liver cannot conjugate berberine adequately and bilirubin displacement risk persists.
- Neonates and infants — never give berberine to neonates. The kernicterus risk is real and well-documented in case reports.
The relative contraindications include severe hepatic impairment (berberine is hepatically metabolized; clearance is reduced), and any patient on multiple CYP-metabolized medications where the cumulative interaction burden makes herbal additions risky. Patients on more than 5 prescription medications should discuss berberine with a pharmacist before starting.
Monitoring — HbA1c, Fasting Glucose, and Fasting Insulin
The recommended monitoring schedule for a patient on berberine for glycemic indications is:
- Baseline — HbA1c, fasting plasma glucose, fasting insulin (for HOMA-IR calculation), lipid panel (total, LDL, HDL, triglycerides), liver function (AST, ALT), basic metabolic panel (creatinine, eGFR).
- 3 months — recheck HbA1c, fasting glucose, fasting insulin. The HbA1c reduction should be measurable by this point if berberine is working (typically 0.3-0.9% reduction depending on baseline).
- 6 months — recheck HbA1c and full lipid panel. The lipid effect (LDL reduction of 20-29%) is typically maximal by 3-6 months.
- Annually thereafter — HbA1c, fasting glucose, fasting insulin, lipid panel, liver function. Long-term safety has been established out to 24 months of continuous use; longer-term data are reassuring but limited.
The relevant lab pages on this site:
- Hemoglobin A1C — the principal glycemic outcome measure (3-month average blood glucose)
- Fasting Insulin — underused but important; allows calculation of HOMA-IR as a measure of insulin resistance
- Lipid Panel — for the berberine lipid-lowering effect (see the cholesterol deep-dive)
If a patient achieves their glycemic target on berberine, the question becomes whether to continue indefinitely or attempt periodic discontinuation. Most clinical practice favors continuing indefinitely as long as the patient is tolerating it well and the prediabetes / diabetes condition is ongoing. Berberine is best understood as a chronic management tool for a chronic condition, not a short-course intervention.
Key Research Papers
- Yin J, Xing H, Ye J (2008). Efficacy of berberine in patients with type 2 diabetes mellitus. Metabolism 57(5):712-717. — PubMed
- Dong H, Wang N, Zhao L, Lu F (2012). Berberine in the treatment of type 2 diabetes mellitus: a systematic review and meta-analysis. Evidence-Based Complementary and Alternative Medicine 2012:591654. — PubMed
- Lan J, Zhao Y, Dong F, et al. (2015). Meta-analysis of the effect and safety of berberine in the treatment of type 2 diabetes mellitus, hyperlipidemia and hypertension. Journal of Ethnopharmacology 161:69-81. — PubMed
- Zhang Y, Li X, Zou D, et al. (2008). Treatment of type 2 diabetes and dyslipidemia with the natural plant alkaloid berberine. Journal of Clinical Endocrinology & Metabolism 93(7):2559-2565. — PubMed
- Yang J, Yin J, Gao H, et al. (2012). Berberine improves insulin sensitivity by inhibiting fat store and adjusting adipokines profile. Evidence-Based Complementary and Alternative Medicine. — PubMed
- Cheng Z, Pang T, Gu M, et al. (2006). Berberine-stimulated glucose uptake in L6 myotubes involves both AMPK and p38 MAPK. Biochimica et Biophysica Acta. — PubMed
- Lee YS, Kim WS, Kim KH, et al. (2006). Berberine, a natural plant product, activates AMP-activated protein kinase with beneficial metabolic effects in diabetic and insulin-resistant states. Diabetes 55(8):2256-2264. — PubMed
- Yin J, Ye J, Jia W (2012). Effects and mechanisms of berberine in diabetes treatment. Acta Pharmaceutica Sinica B. — PubMed
- Zhang X, Zhao Y, Zhang M, et al. (2012). Structural changes of gut microbiota during berberine-mediated prevention of obesity and insulin resistance in high-fat diet-fed rats. PLoS One. — PubMed
- Pang B, Zhao LH, Zhou Q, et al. (2015). Application of berberine on treating type 2 diabetes mellitus. International Journal of Endocrinology. — PubMed
- Liang Y, Xu X, Yin M, et al. (2019). Effects of berberine on blood glucose in patients with type 2 diabetes mellitus: a systematic literature review and a meta-analysis. Endocrine Journal. — PubMed
- Liu Y, Liao Y, Cheng C, et al. (2020). The role of berberine in preventing and treating type 2 diabetes mellitus with associated complications. Frontiers in Pharmacology. — PubMed
PubMed Topic Searches
- PubMed: Berberine type 2 diabetes HbA1c
- PubMed: Berberine vs metformin
- PubMed: Berberine AMPK mechanism
- PubMed: Berberine prediabetes
- PubMed: Berberine insulin sensitivity
- PubMed: Berberine GLUT4
Connections
- Berberine Overview
- Berberine Benefits Hub
- Berberine for Cholesterol
- Berberine for Gut Health & SIBO
- Berberine, AMPK & Metabolic Syndrome
- Diabetes
- Insulin Resistance
- Metabolic Syndrome
- PCOS
- Hemoglobin A1C
- Fasting Insulin
- Lipid Panel
- Blood Sugar
- Gymnema
- Cinnamon
- Bitter Melon
- Inositol
- All Herbs
- Metformin — the first-line diabetes drug berberine matched on HbA1c in the Yin 2008 head-to-head trial.