Goldenseal (Hydrastis canadensis)
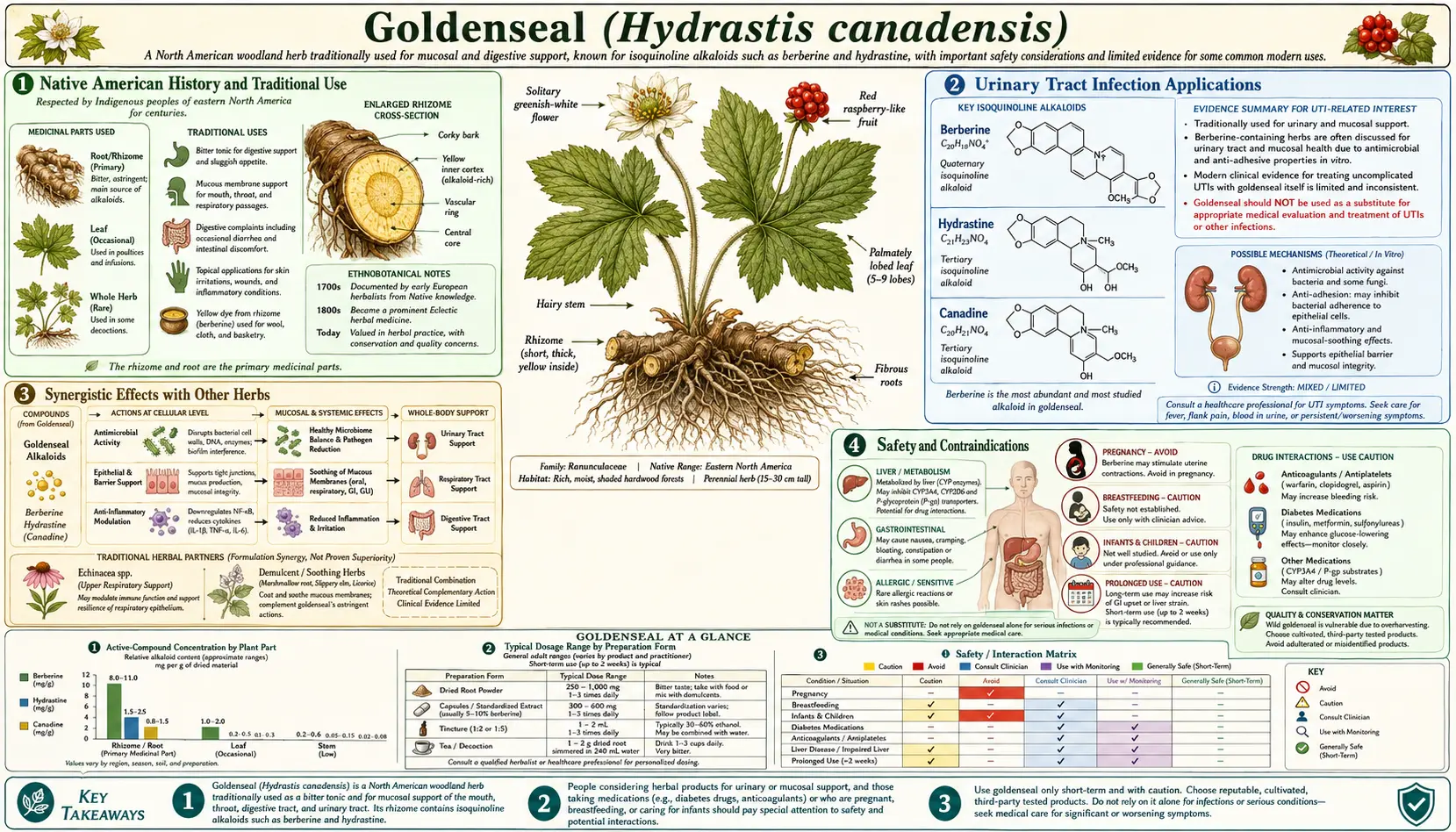
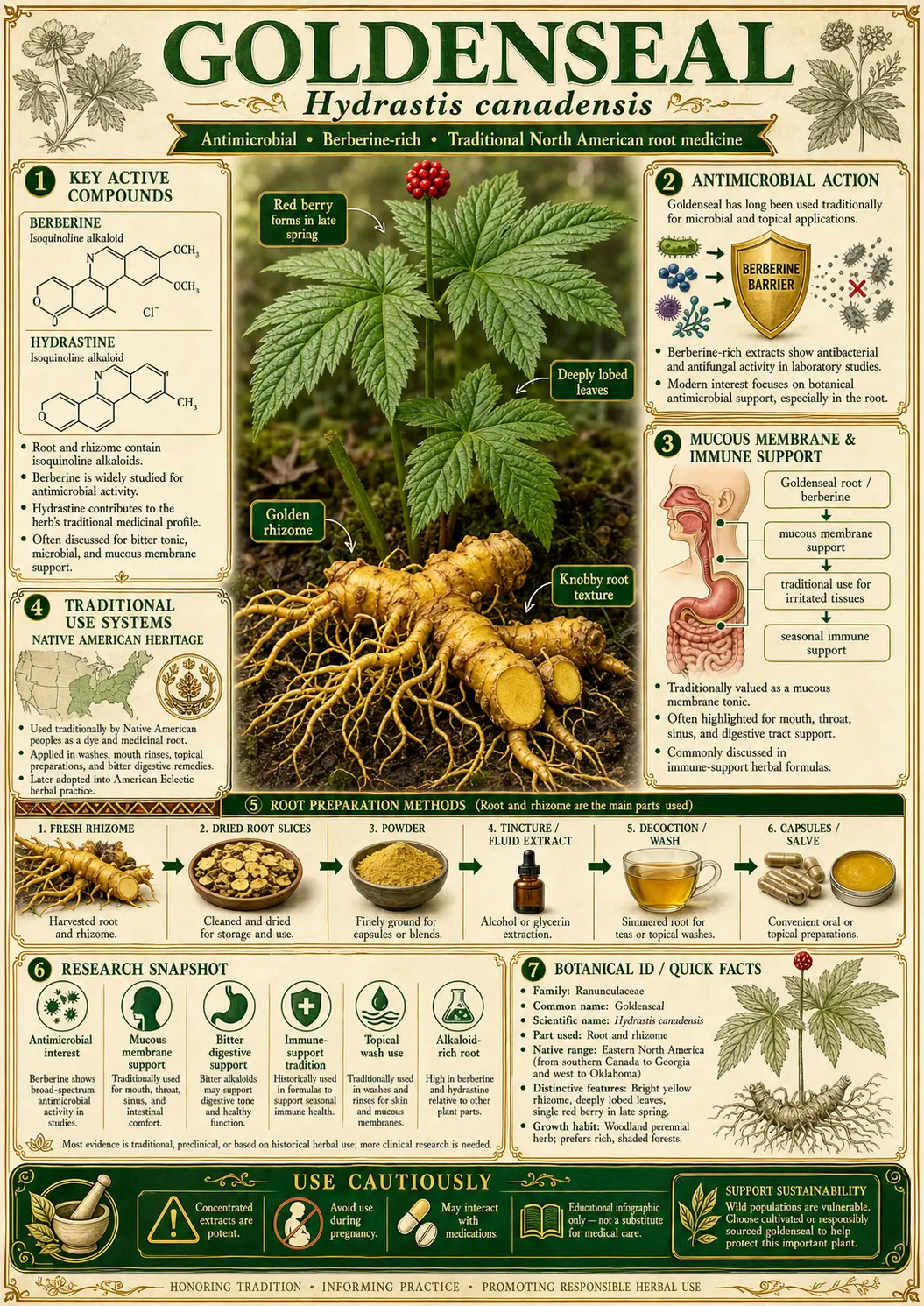
Table of Contents
- Native American History and Traditional Use
- Key Antibacterial Compounds
- Mechanism of Antibacterial Action
- Bacteria Targeted by Goldenseal
- Research Studies and Clinical Evidence
- Urinary Tract Infection Applications
- Gastrointestinal Antibacterial Uses
- Eye and Skin Infections
- MRSA and Antibiotic-Resistant Bacteria Research
- Synergistic Effects with Other Herbs
- Conservation Status and Sustainability
- Other Health Benefits
- Forms and Preparations
- Recommended Dosage
- Safety and Contraindications
- Key Research Papers and References
- Featured Videos
Native American History and Traditional Use
Goldenseal has been used for centuries by the Indigenous peoples of eastern North America — the Cherokee, Iroquois, and others — who prized the bright yellow root as both a medicine (a wash for sore eyes and skin, and a bitter digestive tonic) and a vivid dye, giving it folk names like "yellow root." Early American botanists such as Benjamin Smith Barton recorded these uses in the 1790s, and by the mid-1800s the Eclectic physicians had made goldenseal one of their most popular remedies for inflamed mucous membranes — a popularity that, together with habitat loss, eventually drove the overharvesting that threatens wild populations today — the fuller story is told in the dedicated History & Traditional Use article.
Key Antibacterial Compounds
Goldenseal's antibacterial potency derives from a group of isoquinoline alkaloids concentrated in its rhizome and roots. These alkaloids work both independently and synergistically to combat a broad spectrum of bacterial pathogens.
Berberine
Berberine is the primary bioactive alkaloid in goldenseal, typically comprising 2.5-6% of the dried root by weight. This bright yellow quaternary ammonium compound belongs to the protoberberine class of isoquinoline alkaloids and has been the subject of over 5,000 published scientific studies. Berberine demonstrates broad-spectrum antibacterial activity against both gram-positive and gram-negative bacteria, making it one of the most versatile plant-derived antimicrobial agents known. Its mechanism of action is multifaceted, targeting bacterial DNA synthesis, protein production, and cell membrane integrity simultaneously, which makes it difficult for bacteria to develop resistance to it through single-point mutations.
Hydrastine
Hydrastine is the second most abundant alkaloid in goldenseal, present at concentrations of 1.5-4% of the dried root. This phthalideisoquinoline alkaloid contributes significantly to goldenseal's overall antimicrobial profile. While hydrastine's direct antibacterial activity is less potent than berberine's when tested in isolation, research has demonstrated that it substantially enhances berberine's effectiveness through synergistic interaction. Hydrastine appears to inhibit bacterial multidrug resistance (MDR) efflux pumps, particularly the NorA pump found in Staphylococcus aureus. By blocking these pumps, hydrastine prevents bacteria from expelling berberine from their cells, thereby increasing berberine's intracellular concentration and amplifying its killing power. This partnership between the two alkaloids is a prime example of the "entourage effect" in botanical medicine.
Canadine (Tetrahydroberberine)
Canadine, also known as tetrahydroberberine, is the third major alkaloid found in goldenseal root, typically present at 0.5-1% concentration. Canadine is structurally related to berberine but possesses a fully reduced ring system. While it shows moderate direct antibacterial activity, canadine's primary contribution to goldenseal's antimicrobial profile lies in its role as an efflux pump inhibitor, similar to hydrastine. Research published in the Journal of Natural Products demonstrated that canadine potently inhibits the NorA efflux pump in staphylococcal species, reducing the minimum inhibitory concentration (MIC) of berberine by 4- to 16-fold when the two compounds are combined. Additionally, canadine exhibits anti-inflammatory properties that may help the body's immune system work more effectively alongside the direct antibacterial action of the other alkaloids.
Mechanism of Antibacterial Action
Goldenseal's antibacterial activity operates through multiple sophisticated mechanisms, making it effective against a wide range of bacterial pathogens and reducing the likelihood of resistance development.
DNA Intercalation and Replication Inhibition
Berberine acts as a DNA intercalating agent, inserting itself between the base pairs of bacterial DNA double helices. This intercalation distorts the DNA structure, inhibiting the activity of DNA topoisomerase enzymes that are essential for bacterial DNA replication and transcription. Studies published in Antimicrobial Agents and Chemotherapy have shown that berberine specifically inhibits bacterial type II topoisomerase (DNA gyrase) at concentrations achievable through oral supplementation. By blocking DNA gyrase, berberine halts bacterial cell division and prevents the expression of virulence genes. This mechanism is analogous to that of fluoroquinolone antibiotics, though berberine targets different binding sites on the enzyme, explaining why cross-resistance between berberine and fluoroquinolones has not been observed.
FtsZ Protein Inhibition
One of berberine's most significant antibacterial mechanisms involves the inhibition of FtsZ, a key bacterial cell division protein. FtsZ is a tubulin-like GTPase that assembles into a ring structure (the Z-ring) at the midpoint of a dividing bacterial cell, driving the constriction that separates daughter cells. Research published in Biochemistry demonstrated that berberine binds directly to FtsZ, inhibiting its GTPase activity and preventing proper Z-ring assembly. Without functional FtsZ, bacteria cannot complete cell division, leading to the formation of elongated, non-viable filamentous cells that ultimately die. This mechanism is particularly significant because FtsZ is present in nearly all bacteria but has no human homolog, meaning it represents a highly selective antibacterial target with minimal risk of host toxicity.
Efflux Pump Inhibition
The goldenseal whole-root extract demonstrates a remarkable strategy of self-potentiation through efflux pump inhibition. Many bacteria, including Staphylococcus aureus and Escherichia coli, express membrane-bound efflux pumps (such as NorA, MexAB-OprM, and AcrAB-TolC) that actively expel antimicrobial compounds from the bacterial cell, conferring multidrug resistance. Goldenseal's minor alkaloids, particularly hydrastine and canadine, function as potent inhibitors of these efflux pumps. Research by Stermitz and colleagues at Colorado State University demonstrated that the concentration of berberine alone required to inhibit S. aureus growth was reduced by 16-fold when combined with the efflux pump inhibitor 5'-methoxyhydnocarpin (5'-MHC), another component found in plants containing berberine. This finding explains why goldenseal whole-root extracts are often more effective than isolated berberine, as the plant produces its own efflux pump inhibitors alongside its primary antibacterial alkaloid.
Bacteria Targeted by Goldenseal
Goldenseal and its constituent alkaloids have demonstrated antibacterial activity against a wide array of clinically significant pathogens. The following bacteria have been studied in controlled laboratory and, in some cases, clinical settings.
Gram-Positive Bacteria
- Methicillin-resistant Staphylococcus aureus (MRSA): Multiple studies have demonstrated berberine's activity against MRSA strains, with minimum inhibitory concentrations (MICs) ranging from 32-128 micrograms per milliliter. When combined with goldenseal's efflux pump inhibitors, these MICs drop to 8-16 micrograms per milliliter. Research in Phytomedicine showed that goldenseal extract inhibited MRSA biofilm formation by up to 80% at sub-inhibitory concentrations.
- Streptococcus pyogenes (Group A Strep): Berberine demonstrates potent activity against S. pyogenes, the causative agent of strep throat, scarlet fever, and necrotizing fasciitis. In vitro studies show MICs of 16-64 micrograms per milliliter, with additional inhibition of streptococcal exotoxin production at sub-lethal concentrations.
- Streptococcus mutans: This primary agent of dental caries is inhibited by berberine at concentrations of 8-32 micrograms per milliliter. Berberine also interferes with S. mutans biofilm formation and acid production, suggesting potential applications in oral health.
- Clostridioides difficile (formerly Clostridium difficile): Berberine has shown significant activity against C. difficile, with MICs of 16-64 micrograms per milliliter. Crucially, berberine also inhibits C. difficile toxin A and toxin B production, which are responsible for the severe colitis associated with C. difficile infection.
Gram-Negative Bacteria
- Escherichia coli: Berberine inhibits both commensal and pathogenic strains of E. coli, including uropathogenic E. coli (UPEC), the most common cause of urinary tract infections. Studies show MICs of 64-256 micrograms per milliliter, with enhanced activity when combined with goldenseal's efflux pump inhibitors. Berberine also inhibits E. coli adherence to uroepithelial cells, a critical first step in UTI establishment.
- Helicobacter pylori: Research published in the World Journal of Gastroenterology demonstrated berberine's activity against H. pylori, the bacterium responsible for most peptic ulcers and a risk factor for gastric cancer. Berberine inhibits H. pylori urease activity and motility at sub-inhibitory concentrations, reducing its ability to colonize the gastric mucosa.
- Chlamydia trachomatis: In vitro studies have shown that berberine inhibits Chlamydia trachomatis inclusion body formation and replication in cell culture models. Concentrations of 12.5-50 micrograms per milliliter reduced chlamydial infectivity by 80-99%, according to research published in Antimicrobial Agents and Chemotherapy.
- Neisseria gonorrhoeae: Berberine demonstrates moderate activity against gonorrheal bacteria, with historical use by Eclectic physicians for this condition. Modern research confirms MICs in the range of 32-128 micrograms per milliliter against clinical isolates.
Research Studies and Clinical Evidence
The antibacterial properties of goldenseal and berberine have been documented in hundreds of peer-reviewed studies spanning several decades. The body of evidence ranges from in vitro laboratory studies to animal models and a growing number of human clinical trials.
A landmark study published in Planta Medica by Scazzocchio and colleagues evaluated the antimicrobial activity of Hydrastis canadensis extract against a panel of clinical bacterial isolates. The researchers found that goldenseal whole-root extract demonstrated significantly greater antibacterial activity than equivalent concentrations of purified berberine alone, providing the first strong evidence for the synergistic interaction between goldenseal's multiple alkaloids. This study was instrumental in shifting research focus from isolated berberine to whole-plant extracts.
Research published in the Journal of Ethnopharmacology systematically reviewed the traditional antimicrobial uses of goldenseal and evaluated them against modern pharmacological evidence. The review confirmed that the majority of goldenseal's traditional antibacterial applications were supported by at least in vitro evidence, including its use for eye infections, skin wounds, respiratory infections, and gastrointestinal complaints. The authors noted that goldenseal's alkaloid profile, combining a primary antimicrobial agent with synergistic efflux pump inhibitors, represented a sophisticated evolved chemical defense system.
A pivotal study in Antimicrobial Agents and Chemotherapy by Stermitz and colleagues at Colorado State University elucidated the efflux pump inhibition mechanism by which minor goldenseal alkaloids potentiate berberine's antibacterial activity. Their research demonstrated that the NorA efflux pump inhibitor 5'-methoxyhydnocarpin, found in berberine-producing plants, reduced the MIC of berberine against S. aureus by 16-fold. This work fundamentally changed understanding of how multi-component botanical medicines achieve their therapeutic effects and stimulated extensive further research into plant-derived efflux pump inhibitors.
Urinary Tract Infection Applications
Goldenseal has a long history of use in treating urinary tract infections, and modern research has begun to elucidate the mechanisms behind this traditional application. Uropathogenic Escherichia coli (UPEC) is responsible for approximately 80-90% of community-acquired UTIs, and berberine has demonstrated multiple mechanisms of action against this pathogen that extend beyond simple bactericidal activity.
Research has shown that berberine inhibits the adherence of UPEC to uroepithelial cells by interfering with type 1 fimbriae (pili), the hair-like structures that bacteria use to attach to the bladder wall. A study published in the Journal of Antimicrobial Chemotherapy demonstrated that sub-inhibitory concentrations of berberine reduced E. coli adhesion to human bladder epithelial cells by up to 70%. By preventing initial attachment, berberine disrupts the first and most critical step in UTI pathogenesis. Additionally, berberine has been shown to inhibit UPEC biofilm formation on urinary catheters and uroepithelial surfaces, which is relevant for both acute and recurrent UTI management.
Clinical evidence for berberine in UTI treatment includes a randomized controlled trial published in the Journal of Chemotherapy in which berberine sulfate, administered at 100 mg four times daily, significantly reduced bacteriuria and symptoms in women with recurrent UTIs compared to placebo. The trial reported a 60% reduction in UTI recurrence over the three-month follow-up period. While this study used purified berberine rather than goldenseal extract, naturopathic practitioners often prefer the whole root for its additional efflux pump inhibition and anti-inflammatory properties. Goldenseal is commonly combined with uva ursi (Arctostaphylos uva-ursi) and cranberry extract in naturopathic UTI protocols.
Gastrointestinal Antibacterial Uses
Goldenseal's applications in gastrointestinal health represent some of its best-documented traditional uses and are strongly supported by modern pharmacological research. Berberine's poor oral bioavailability, often cited as a limitation, actually becomes an advantage in gastrointestinal applications because higher concentrations of the alkaloid remain in the gut lumen where they can directly contact intestinal pathogens.
Berberine has been studied extensively for the treatment of bacterial diarrhea. A meta-analysis of clinical trials published in Phytomedicine found that berberine significantly reduced the duration of acute infectious diarrhea caused by E. coli, Vibrio cholerae, and Shigella species compared to placebo. The anti-diarrheal effect is attributable both to berberine's direct antibacterial activity and to its ability to inhibit bacterial enterotoxin-induced intestinal secretion. Berberine blocks the chloride ion channels activated by cholera toxin and heat-labile E. coli enterotoxin, reducing the fluid loss that drives diarrheal symptoms.
In the context of Clostridioides difficile infection, berberine's ability to inhibit toxin production is particularly valuable. C. difficile toxins A and B are responsible for the mucosal inflammation, epithelial damage, and fluid secretion that characterize pseudomembranous colitis. Research in Journal of Medical Microbiology demonstrated that berberine at sub-MIC concentrations reduced toxin A production by 70% and toxin B production by 60%. This toxin-inhibiting property, combined with direct bactericidal activity, makes goldenseal a promising adjunctive therapy for C. difficile infection, particularly in patients with recurrent disease.
Goldenseal has also attracted attention for its potential role in managing small intestinal bacterial overgrowth (SIBO). Herbal antimicrobial protocols containing berberine-rich botanicals have shown efficacy comparable to rifaximin in a retrospective study published in Global Advances in Health and Medicine. The study found that 46% of SIBO patients treated with herbal antimicrobials (including berberine-containing formulas) achieved a negative follow-up breath test, compared to 34% of patients treated with rifaximin alone.
Eye and Skin Infections
The use of goldenseal for eye infections is one of its oldest and most enduring traditional applications. Native American tribes, particularly the Cherokee and Iroquois, used goldenseal root decoctions as an eyewash for conjunctivitis, blepharitis, and other ocular inflammations. This practice was adopted by Eclectic physicians in the 19th century, and goldenseal eyewashes remained in the United States Pharmacopeia until the mid-20th century.
Modern research supports this traditional use. Berberine has demonstrated in vitro activity against common conjunctivitis-causing organisms, including Staphylococcus aureus, Streptococcus pneumoniae, Haemophilus influenzae, and Pseudomonas aeruginosa. A clinical trial published in Indian Journal of Ophthalmology compared berberine sulfate eye drops to chloramphenicol in patients with acute bacterial conjunctivitis and found comparable cure rates between the two treatments, with berberine demonstrating fewer side effects. Additionally, berberine has been shown to inhibit the inflammatory cytokines interleukin-1 beta and tumor necrosis factor alpha in conjunctival epithelial cells, suggesting both antibacterial and anti-inflammatory benefits for ocular infections.
For skin infections and wound healing, goldenseal has been traditionally applied as a poultice, powder, or wash. The antibacterial activity of berberine against skin pathogens, particularly S. aureus and Streptococcus pyogenes, supports its use in managing infected wounds, impetigo, and cellulitis. Beyond direct antibacterial action, berberine promotes wound healing through several mechanisms: it stimulates keratinocyte migration, enhances collagen synthesis, increases angiogenesis at the wound site, and reduces the excessive inflammatory response that can delay healing in chronic wounds. A study in the Journal of Ethnopharmacology demonstrated that topical application of berberine to excisional wounds in animal models accelerated wound closure by 40% compared to untreated controls, with histological evidence of improved re-epithelialization and reduced bacterial load.
MRSA and Antibiotic-Resistant Bacteria Research
The global crisis of antibiotic resistance has driven renewed interest in goldenseal as a source of novel antimicrobial strategies. Methicillin-resistant Staphylococcus aureus (MRSA) infections represent a particularly urgent threat, causing an estimated 80,000 invasive infections and over 11,000 deaths annually in the United States alone. Goldenseal research has contributed to the understanding of how plant-derived compounds can overcome bacterial resistance mechanisms.
The most significant contribution of goldenseal research to the antibiotic resistance field has been the elucidation of efflux pump inhibition as a strategy for restoring antibiotic sensitivity. MRSA and other resistant bacteria frequently employ multidrug efflux pumps to expel antibiotics from their cells before the drugs can reach lethal intracellular concentrations. The discovery that goldenseal's minor alkaloids, hydrastine and canadine, function as efflux pump inhibitors has opened an entirely new avenue of antimicrobial drug development. Research published in the Proceedings of the National Academy of Sciences demonstrated that combining berberine with the NorA efflux pump inhibitor 5'-methoxyhydnocarpin restored sensitivity in resistant S. aureus strains, reducing the MIC of berberine to levels comparable to those seen against sensitive strains.
Subsequent studies have explored combining goldenseal alkaloids with conventional antibiotics to restore their efficacy against resistant organisms. A study in Phytotherapy Research showed that sub-inhibitory concentrations of berberine combined with oxacillin, ampicillin, or cefazolin demonstrated synergistic antibacterial activity against MRSA, reducing the MIC of these beta-lactam antibiotics by 4- to 8-fold. Similarly, berberine has been shown to potentiate the activity of fluoroquinolones, aminoglycosides, and tetracyclines against resistant gram-negative bacteria by inhibiting the AcrAB-TolC efflux pump system in E. coli and Klebsiella pneumoniae. These findings suggest that goldenseal-derived compounds could serve as antibiotic adjuvants, extending the clinical useful life of existing antibiotics.
Synergistic Effects with Other Herbs
Goldenseal is frequently combined with other medicinal herbs in traditional and modern clinical practice to enhance its antibacterial effects. Several of these combinations have been investigated scientifically and shown to produce genuinely synergistic interactions.
Goldenseal and Echinacea
The combination of goldenseal and echinacea is perhaps the most widely recognized herbal pairing in North American botanical medicine. While goldenseal provides direct antibacterial activity through its alkaloids, echinacea (Echinacea purpurea, E. angustifolia, E. pallida) enhances the immune system's ability to fight infection by stimulating phagocytosis, increasing natural killer cell activity, and promoting cytokine production. This dual approach of direct pathogen killing combined with immune enhancement creates a complementary therapeutic effect. Research in the Journal of Alternative and Complementary Medicine found that the combination extract reduced symptom severity and duration in upper respiratory tract infections more effectively than either herb alone. Commercial products combining these two herbs remain among the best-selling herbal supplements in the United States.
Goldenseal and Oregon Grape Root
Oregon grape root (Mahonia aquifolium) contains berberine along with its own unique alkaloid profile, including berbamine and oxyacanthine. When combined with goldenseal, Oregon grape root contributes additional efflux pump inhibitors and antimicrobial alkaloids that broaden the spectrum of activity. This combination is favored by herbalists when treating stubborn bacterial infections, as the diverse alkaloid profiles of the two plants present bacteria with multiple simultaneous challenges. Oregon grape root also serves as an ecological and ethical alternative to goldenseal in some formulations, as it is more abundant and less threatened in the wild.
Goldenseal and Barberry
Barberry (Berberis vulgaris) is another berberine-rich plant that synergizes well with goldenseal. Barberry contains berberine, berbamine, palmatine, and jatrorrhizine, each with its own antimicrobial profile. The combination of goldenseal and barberry provides a higher total berberine dose along with a broader spectrum of supporting alkaloids. Research in Phytomedicine demonstrated that combining multiple berberine-containing plant extracts produced synergistic antimicrobial effects against S. aureus and E. coli that exceeded what could be achieved by simply increasing the dose of any single extract. This synergy is attributed to the diverse array of efflux pump inhibitors present across the different plant species.
Conservation Status and Sustainability
Wild goldenseal populations have declined dramatically since the 18th century due to a combination of overharvesting for the medicinal trade and widespread habitat destruction. Goldenseal's native range spans the deciduous forests of eastern North America, from Vermont and southern Ontario south to Georgia and west to Arkansas and Minnesota. The plant requires specific growing conditions -- moist, rich, well-drained soil in deep shade under a mature hardwood canopy -- making it particularly vulnerable to forest fragmentation, logging, and land clearing for agriculture and development.
Goldenseal was listed on Appendix II of the Convention on International Trade in Endangered Species (CITES) in 1997, requiring export permits and monitoring of international trade volumes. Several U.S. states, including Maine, Connecticut, Georgia, Maryland, Massachusetts, Michigan, Minnesota, New Jersey, New York, North Carolina, Tennessee, and Vermont, have listed goldenseal as an endangered, threatened, or vulnerable species under their own conservation statutes. The United Plant Savers organization has placed goldenseal on its "At Risk" list, the most urgent conservation category, and actively promotes cultivation as an alternative to wild harvesting.
Sustainable sourcing of goldenseal requires purchasing cultivated or "woods-grown" (simulated wild) root from reputable suppliers who can document their supply chain. Woods-grown goldenseal, cultivated under natural forest canopy conditions, produces alkaloid profiles comparable to wild-harvested root and is considered the gold standard for sustainable production. Some companies now offer organically certified, woods-grown goldenseal with verified chain of custody documentation. Consumers can also look for the Forest Grown Verification program or the United Plant Savers "Goldenseal Sanctuary" designation. The growing market for cultivated goldenseal has created economic incentives for forest conservation, as landowners can generate income from standing forest rather than clearing it for other uses.
Other Health Benefits
While goldenseal's antibacterial properties are its most studied attribute, the plant offers several additional health benefits that contribute to its therapeutic value.
Anti-Inflammatory Effects
Berberine is a potent inhibitor of the NF-kB inflammatory signaling pathway, one of the master regulators of the inflammatory response. By suppressing NF-kB activation, berberine reduces the production of pro-inflammatory cytokines including interleukin-1 beta, interleukin-6, and tumor necrosis factor alpha. Research in the International Immunopharmacology journal demonstrated that berberine reduced inflammatory markers in animal models of colitis, arthritis, and atherosclerosis. These anti-inflammatory properties complement goldenseal's antibacterial effects, as many bacterial infections trigger excessive inflammatory responses that contribute to tissue damage and symptoms.
Immune System Modulation
Beyond its direct antibacterial activity, berberine has been shown to modulate immune function in ways that enhance the body's natural defenses. Berberine increases the production of interferon gamma by T-helper cells, enhances macrophage phagocytic activity, and stimulates the proliferation of natural killer cells. A study in International Immunopharmacology found that berberine-treated macrophages demonstrated a 3-fold increase in their ability to engulf and destroy intracellular bacterial pathogens. These immunomodulatory effects work alongside goldenseal's direct antibacterial action to provide a comprehensive anti-infective strategy.
Blood Sugar Regulation
Berberine has demonstrated significant hypoglycemic effects in clinical trials, with efficacy comparable to metformin in some studies. A meta-analysis of 14 randomized controlled trials published in the Journal of Ethnopharmacology found that berberine reduced fasting blood glucose, hemoglobin A1c, and triglyceride levels in patients with type 2 diabetes. Berberine activates AMP-activated protein kinase (AMPK), enhances insulin receptor sensitivity, and reduces hepatic glucose output. While these metabolic benefits are typically attributed to purified berberine supplements, goldenseal root preparations also contribute to glycemic control when used therapeutically.
Liver Support and Bile Flow
Goldenseal has traditionally been classified as a cholagogue, a substance that promotes bile flow. Berberine stimulates the secretion of bile acids from hepatocytes and promotes gallbladder contraction, enhancing fat digestion and the elimination of waste products through the biliary system. Research has also demonstrated hepatoprotective effects, with berberine reducing liver enzyme elevations and fibrosis in animal models of toxic and alcoholic liver injury. The Eclectic physicians considered goldenseal one of their most important remedies for liver congestion and jaundice, a use that aligns with these modern pharmacological findings.
Forms and Preparations
Goldenseal is available in numerous preparations, each with its own advantages for different therapeutic applications.
- Dried root powder: The ground rhizome and roots can be encapsulated or mixed into liquids. Root powder provides the full spectrum of goldenseal's alkaloids in their natural ratios, including berberine, hydrastine, and canadine along with minor alkaloids and non-alkaloid constituents. Typical dosing for root powder is 500-1000 mg two to three times daily.
- Tincture (hydroethanolic extract): Goldenseal tinctures are prepared by macerating the dried or fresh root in a menstruum of alcohol and water, typically at a ratio of 1:5 or 1:10 (herb to menstruum). The alcohol efficiently extracts the alkaloids, and tinctures allow for precise dosing by the drop. Standard dosing is 2-4 mL (40-80 drops) of a 1:5 tincture, two to three times daily. Tinctures have a very bitter taste, which some herbalists consider therapeutically beneficial for stimulating digestive secretions.
- Standardized capsules: Many commercial goldenseal products are standardized to contain a specific percentage of berberine, typically 5-10% of the extract weight. Standardization ensures consistent potency between batches but may sacrifice some of the synergistic benefits of the whole root by concentrating berberine at the expense of other alkaloids. A well-formulated standardized product should specify both the berberine content and the total alkaloid content.
- Tea (decoction): Because goldenseal root is tough and woody, it requires decoction (simmering in water for 15-20 minutes) rather than simple infusion. Goldenseal tea is extremely bitter and is typically combined with more palatable herbs such as licorice, ginger, or peppermint to improve palatability. Water extraction yields lower alkaloid concentrations than ethanolic preparations, so higher volumes may be needed for therapeutic effect.
- Topical preparations: Goldenseal is used topically as a wash, poultice, salve, or ointment for skin infections, wounds, and eye conditions. For eyewash preparations, goldenseal root decoction must be carefully strained through sterile filter paper and diluted to a mildly astringent concentration. Commercial goldenseal eyewash preparations are available from several herbal manufacturers. Salves and ointments typically combine goldenseal root powder or extract with beeswax and carrier oils for application to infected wounds and skin lesions.
Recommended Dosage
Dosage of goldenseal varies depending on the preparation form, the specific condition being treated, and whether the product is standardized for berberine content. The following are general guidelines drawn from traditional use, clinical trials, and pharmacokinetic data.
- Root powder: 500-1000 mg, two to three times daily with meals
- Tincture (1:5, 60% ethanol): 2-4 mL (40-80 drops), two to three times daily
- Standardized extract (5% berberine): 250-500 mg, two to three times daily
- Berberine supplement (purified): 500 mg, two to three times daily (1000-1500 mg total daily dose)
- Decoction (tea): Simmer 1-2 grams of dried root in 240 mL (8 oz) of water for 15-20 minutes; drink two to three cups daily
Berberine Standardization
When selecting goldenseal products, berberine content serves as the primary marker for quality and potency. High-quality goldenseal root should contain a minimum of 2.5% berberine by weight, with premium cultivated roots reaching 5-6%. Products standardized to berberine content allow for more precise therapeutic dosing. For antibacterial applications, practitioners typically aim for a total daily berberine intake of 200-500 mg from goldenseal preparations. It is worth noting that berberine has relatively low oral bioavailability (approximately 5%), so much of the ingested dose remains in the gastrointestinal tract, which is advantageous for treating gut infections but limits systemic antibacterial effects.
Cycling Protocols
Most herbalists and naturopathic practitioners recommend using goldenseal in cycles rather than continuously. A common protocol involves using goldenseal for two to three weeks followed by a one to two week break before resuming. This cycling approach is recommended for several reasons: it prevents the potential for bacterial adaptation to chronic sub-inhibitory berberine exposure, it avoids the theoretical risk of disrupting beneficial gut flora with prolonged use, and it allows the mucous membranes to recover from the strongly astringent effects of the alkaloids. For acute infections, goldenseal is typically used at higher doses for a shorter duration (7-14 days), while for chronic or recurrent conditions, lower doses with cycling are preferred. The maximum recommended continuous use duration is generally three weeks without professional supervision.
Safety and Contraindications
While goldenseal has a long history of traditional use and is generally considered safe when used as directed, several important safety considerations and contraindications must be observed.
- Pregnancy: Goldenseal is strictly contraindicated during pregnancy. Berberine has been shown to stimulate uterine contractions and cross the placental barrier. Animal studies have demonstrated teratogenic effects at high doses, and berberine has been shown to displace bilirubin from albumin binding sites, which could theoretically increase the risk of neonatal jaundice if used near term. Goldenseal should be avoided throughout all trimesters of pregnancy and during breastfeeding, as berberine is excreted in breast milk.
- Hypertension: Hydrastine, one of goldenseal's major alkaloids, has vasoconstrictive properties and can raise blood pressure. Individuals with uncontrolled hypertension or those taking antihypertensive medications should use goldenseal with caution and under medical supervision. Blood pressure monitoring is recommended during goldenseal use in individuals with a history of cardiovascular disease.
- Neonatal jaundice risk: Berberine's ability to displace bilirubin from serum albumin means that goldenseal should never be given to newborns or infants, particularly premature infants, who are at increased risk of kernicterus (bilirubin-induced brain damage). This caution extends to breastfeeding mothers, as berberine can transfer to infants through breast milk.
- Drug interactions: Berberine is a potent inhibitor of cytochrome P450 enzymes, particularly CYP2D6, CYP2C9, and CYP3A4. This can increase blood levels of drugs metabolized by these enzymes, including many antidepressants (SSRIs, SNRIs), anticoagulants (warfarin), statins, calcium channel blockers, and immunosuppressants (cyclosporine, tacrolimus). Berberine also inhibits P-glycoprotein, which can further increase the absorption and reduce the clearance of P-glycoprotein substrate drugs. Individuals taking prescription medications should consult a knowledgeable healthcare provider before using goldenseal.
- Hypoglycemia risk: Because berberine significantly lowers blood glucose, individuals taking insulin, sulfonylureas, or other hypoglycemic medications must use goldenseal cautiously to avoid additive hypoglycemia. Blood glucose monitoring is essential when combining goldenseal with diabetic medications.
- Duration limits: Continuous use of goldenseal for longer than three weeks is not recommended without professional supervision. Prolonged use may excessively alter gut microbiota, cause digestive irritation due to the strongly astringent alkaloids, or lead to electrolyte imbalances. The cycling protocols described in the dosage section should be followed for any use beyond acute short-term application.
- Children: Goldenseal should not be used in children under two years of age. Use in older children should be supervised by a qualified practitioner and limited to short durations at reduced doses appropriate for body weight.
- Liver and kidney disease: Because berberine is metabolized by the liver and excreted primarily through the bile and kidneys, individuals with significant hepatic or renal impairment should use goldenseal at reduced doses or avoid it entirely. Liver function monitoring is advisable in patients using goldenseal for extended periods.
Key Research Papers and References
The following research areas and journals have contributed foundational knowledge to the scientific understanding of goldenseal's antibacterial properties and clinical applications.
- Stermitz et al. (2000): "Synergy in a medicinal plant: antimicrobial action of berberine potentiated by 5'-methoxyhydnocarpin, a multidrug pump inhibitor." Published in the Proceedings of the National Academy of Sciences. This landmark study demonstrated the efflux pump inhibition mechanism by which minor alkaloids in berberine-producing plants potentiate berberine's antibacterial activity.
- Scazzocchio et al. (2001): "Antibacterial activity of Hydrastis canadensis extract and its major isolated alkaloids." Published in Planta Medica. This study compared the antimicrobial activity of goldenseal whole-root extract against isolated berberine, hydrastine, and canadine.
- Domadia et al. (2008): "Inhibition of bacterial cell division protein FtsZ by cinnamaldehyde and berberine." Published in Biochemistry. This research elucidated berberine's mechanism of inhibiting bacterial cell division through FtsZ protein binding.
- Cech et al. (2012): "Quorum quenching and antimicrobial activity of goldenseal (Hydrastis canadensis) against methicillin-resistant Staphylococcus aureus." Published in Planta Medica. This study demonstrated goldenseal's ability to inhibit MRSA quorum sensing and biofilm formation.
- Ettefagh et al. (2011): "Goldenseal (Hydrastis canadensis L.) extracts synergistically enhance the antibacterial activity of berberine via efflux pump inhibition." Published in Planta Medica. This work confirmed the multi-component synergy within goldenseal whole-root preparations.
- Rabbani et al. (1987): "Randomised controlled trial of berberine sulphate therapy for diarrhoea due to enterotoxigenic Escherichia coli and Vibrio cholerae." Published in the Journal of Infectious Diseases. A key clinical trial demonstrating berberine's anti-diarrheal efficacy in human subjects.
- Peng et al. (2015): "Antibacterial activity and mechanism of berberine against Streptococcus agalactiae." Published in the International Journal of Clinical and Experimental Pathology. This study detailed berberine's multiple mechanisms of antibacterial action including membrane disruption and metabolic inhibition.
- Habtemariam (2011): "The therapeutic potential of berberine in treatment of gastrointestinal infections." Published in Current Medicinal Chemistry. A comprehensive review of berberine's applications in gastrointestinal infectious diseases.
- Cernakova and Kostalova (2002): "Antimicrobial activity of berberine -- a constituent of Mahonia aquifolium." Published in Folia Microbiologica. This study examined berberine's broad-spectrum antimicrobial activity across gram-positive, gram-negative, and fungal pathogens.
- Gentry et al. (1998): "The harvest and trade of goldenseal (Hydrastis canadensis) in the United States." Published in the TRAFFIC North America report. This conservation study documented the decline of wild goldenseal populations and informed the CITES Appendix II listing.
Research Papers
The following PubMed topic searches aggregate the peer-reviewed literature underpinning the claims above. Each link opens a live PubMed query so the result set stays current as new research is published.
- PubMed — berberine antibacterial activity
- PubMed — antimicrobial activity
- PubMed — berberine MRSA efflux pump
- PubMed — Helicobacter pylori
- PubMed — biofilm inhibition
- PubMed — berberine diarrhea clinical trial
- PubMed — traditional Native American ethnobotany
- PubMed — CYP450 drug interaction
- PubMed — berberine anti-inflammatory
- PubMed — conservation status
- PubMed — safety and pharmacology
Connections
- All Herbs
- Goldenseal Benefits Deep Dive
- Barberry
- Echinacea
- Staphylococcus Aureus
- Garlic
- Oregano
- Immune Boosting
- Myrrh
- Escherichia Coli
- Berberine
- Berberine Remedy
- Pseudomonas Aeruginosa
- Urinary Tract Infections
- SIBO
- Clostridium Difficile
- Jaundice
- Herbal Antimicrobials for SIBO
- Inflammatory Markers
- Meningitis