Abdominal Pain or Discomfort
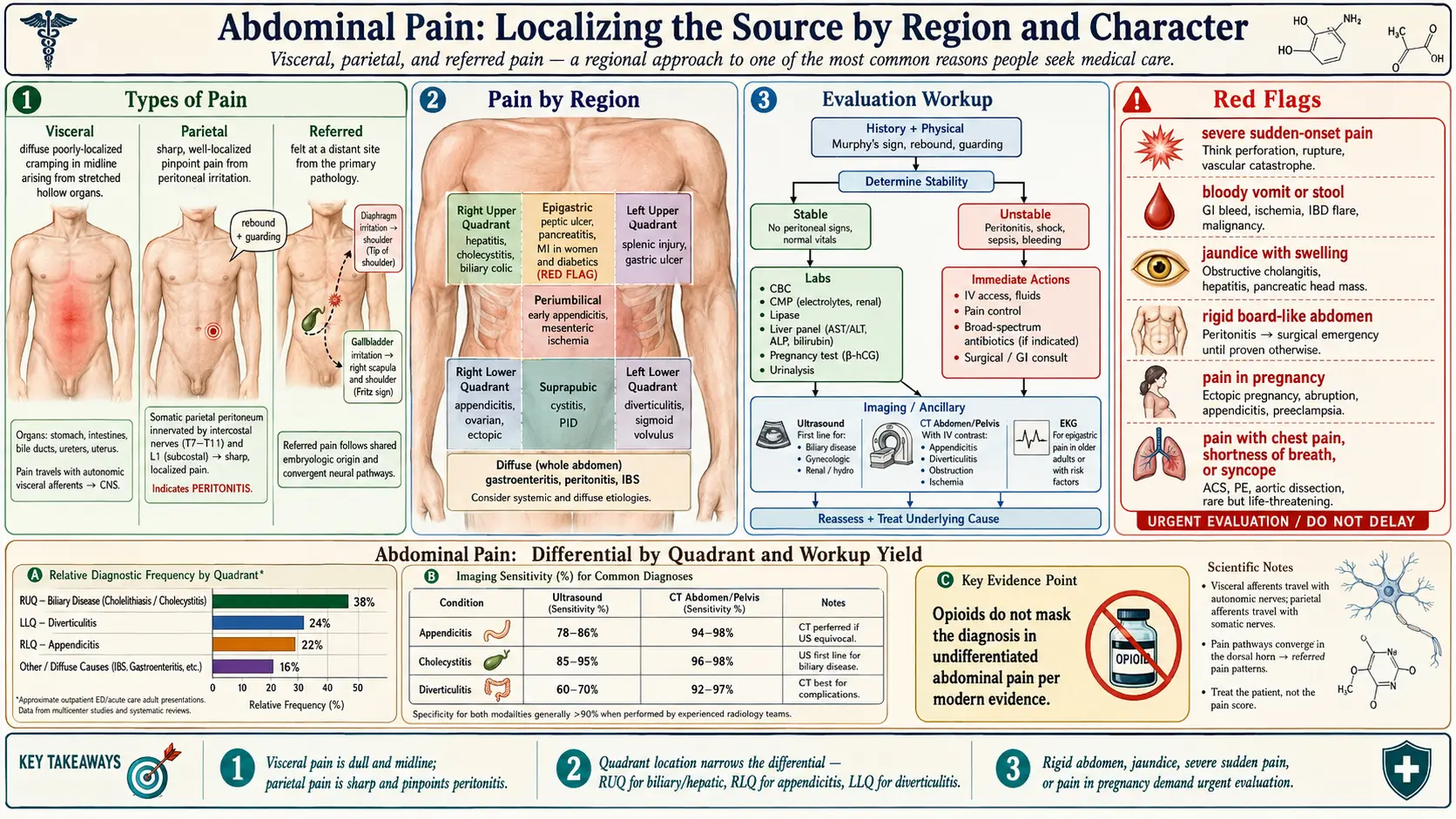

Table of Contents
- Overview
- Types of Abdominal Pain
- Pain by Region
- Common Causes
- Evaluation
- Management
- When to Seek Medical Care
- Connections
- References & Research
- Featured Videos
Overview
Abdominal pain is one of the most common reasons people seek medical care, ranging from mild discomfort that resolves on its own to a life-threatening surgical emergency. The location, character, timing, and accompanying symptoms guide the diagnosis. In viral hepatitis, abdominal pain is typically a dull or aching discomfort in the right upper quadrant, where the inflamed liver stretches its capsule.
Types of Abdominal Pain
- Visceral pain — diffuse, poorly localized, dull or crampy. Arises from stretching, distention, or inflammation of hollow or solid organs. Often midline because of bilateral autonomic innervation.
- Parietal (somatic) pain — sharp, well-localized, worsened by movement or coughing. Comes from irritation of the parietal peritoneum and is the hallmark of peritonitis.
- Referred pain — felt at a site distant from the source. Examples include diaphragmatic irritation referred to the shoulder or biliary pain referred to the right scapula.
Pain by Region
- Right upper quadrant — hepatitis, cholecystitis, biliary colic, hepatic abscess, right lower lobe pneumonia.
- Epigastric — peptic ulcer, gastritis, GERD, pancreatitis, myocardial infarction (especially in women and diabetics).
- Left upper quadrant — splenic injury or infarction, gastric ulcer, pancreatitis.
- Periumbilical — early appendicitis, small bowel obstruction, mesenteric ischemia.
- Right lower quadrant — appendicitis, ovarian pathology, ectopic pregnancy, Crohn's disease.
- Left lower quadrant — diverticulitis, sigmoid volvulus, ovarian pathology.
- Suprapubic — cystitis, urinary retention, pelvic inflammatory disease.
- Diffuse — gastroenteritis, peritonitis, mesenteric ischemia, irritable bowel syndrome, sickle cell crisis.
Common Causes
- Hepatobiliary — viral hepatitis, gallstones, cholecystitis, cholangitis, hepatic congestion.
- Gastrointestinal — gastroenteritis, peptic ulcer, GERD, IBS, IBD (Crohn's, ulcerative colitis), constipation, bowel obstruction.
- Pancreatic — acute and chronic pancreatitis, pancreatic cancer.
- Vascular — mesenteric ischemia, abdominal aortic aneurysm.
- Genitourinary — kidney stones, pyelonephritis, urinary retention.
- Gynecologic — ovarian cyst, ectopic pregnancy, endometriosis, pelvic inflammatory disease.
- Functional — irritable bowel syndrome, functional dyspepsia.
Evaluation
- History and physical exam — onset, character, location, radiation, timing, and aggravating/relieving factors. Examine for tenderness, rebound, guarding, and Murphy's sign.
- CBC, CMP, lipase, liver panel — to look for infection, electrolyte disturbance, pancreatitis, and hepatobiliary disease.
- Pregnancy test — in any woman of reproductive age.
- Urinalysis — for UTI, hematuria, ketones.
- Imaging — ultrasound for biliary, gynecologic, or renal causes; CT for appendicitis, diverticulitis, obstruction, ischemia.
- EKG — for epigastric pain in older or at-risk adults to exclude cardiac ischemia.
Management
Treatment depends on cause. Functional and self-limited causes resolve with supportive care. Surgical conditions (appendicitis, perforation, obstruction, ectopic pregnancy) require urgent intervention. Pain control, hydration, antiemetics, and treatment of the underlying disease are the mainstays. Opioids are not contraindicated in undifferentiated abdominal pain — modern evidence shows they do not mask the diagnosis.
When to Seek Medical Care
- Severe or sudden-onset pain.
- Pain with fever, vomiting blood, bloody stool, or inability to keep down fluids.
- Pain with jaundice or marked abdominal swelling.
- Rigid, board-like abdomen (suggests peritonitis).
- Pain in pregnancy.
- Pain with chest pain, shortness of breath, or syncope.
Connections
- Pancreatitis
- Hepatitis
- Irritable Bowel Syndrome
- Diverticulitis
- Gallbladder Disease
- Inflammatory Bowel Disease
- Peptic Ulcer Disease
- Nausea and Vomiting
- Crohn's Disease
- Constipation
- Jaundice
- SIBO
- Ulcerative Colitis
- Inflammatory Markers
- Liver Disease
- Bloating
- Hepatitis B
- Hepatitis C
References & Research
Historical Background
Surgeon Sir Zachary Cope's 1921 monograph The Early Diagnosis of the Acute Abdomen remains a foundational text for the bedside evaluation of abdominal pain, emphasizing careful history and physical examination over technology. The introduction of CT in the 1970s and bedside ultrasound in the 1990s transformed the diagnostic workup, dramatically improving accuracy for appendicitis, diverticulitis, and biliary disease.
Key Research Papers
- Cartwright SL, Knudson MP. Evaluation of acute abdominal pain in adults. American Family Physician. 2008;77(7):971-978.
- Wagner JM, McKinney WP, Carpenter JL. Does this patient have appendicitis? JAMA. 1996;276(19):1589-1594.
- Manterola C, Vial M, Moraga J, Astudillo P. Analgesia in patients with acute abdominal pain. Cochrane Database of Systematic Reviews. 2011;(1):CD005660.
- Tenner S, Baillie J, DeWitt J, Vege SS. American College of Gastroenterology guideline: management of acute pancreatitis. American Journal of Gastroenterology. 2013;108(9):1400-1415.
- Strate LL, Modi R, Cohen E, Spiegel BM. Diverticular disease as a chronic illness. American Journal of Gastroenterology. 2012;107(10):1486-1493.
- Brown HF, Kelso L. Abdominal pain: an approach to a challenging diagnosis. AACN Advanced Critical Care. 2014;25(3):266-278.
- Mayer EA. Functional gastrointestinal disorders and the brain-gut axis. New England Journal of Medicine. 2008;358(16):1692-1699.