Pediatric EDS and Transition of Care
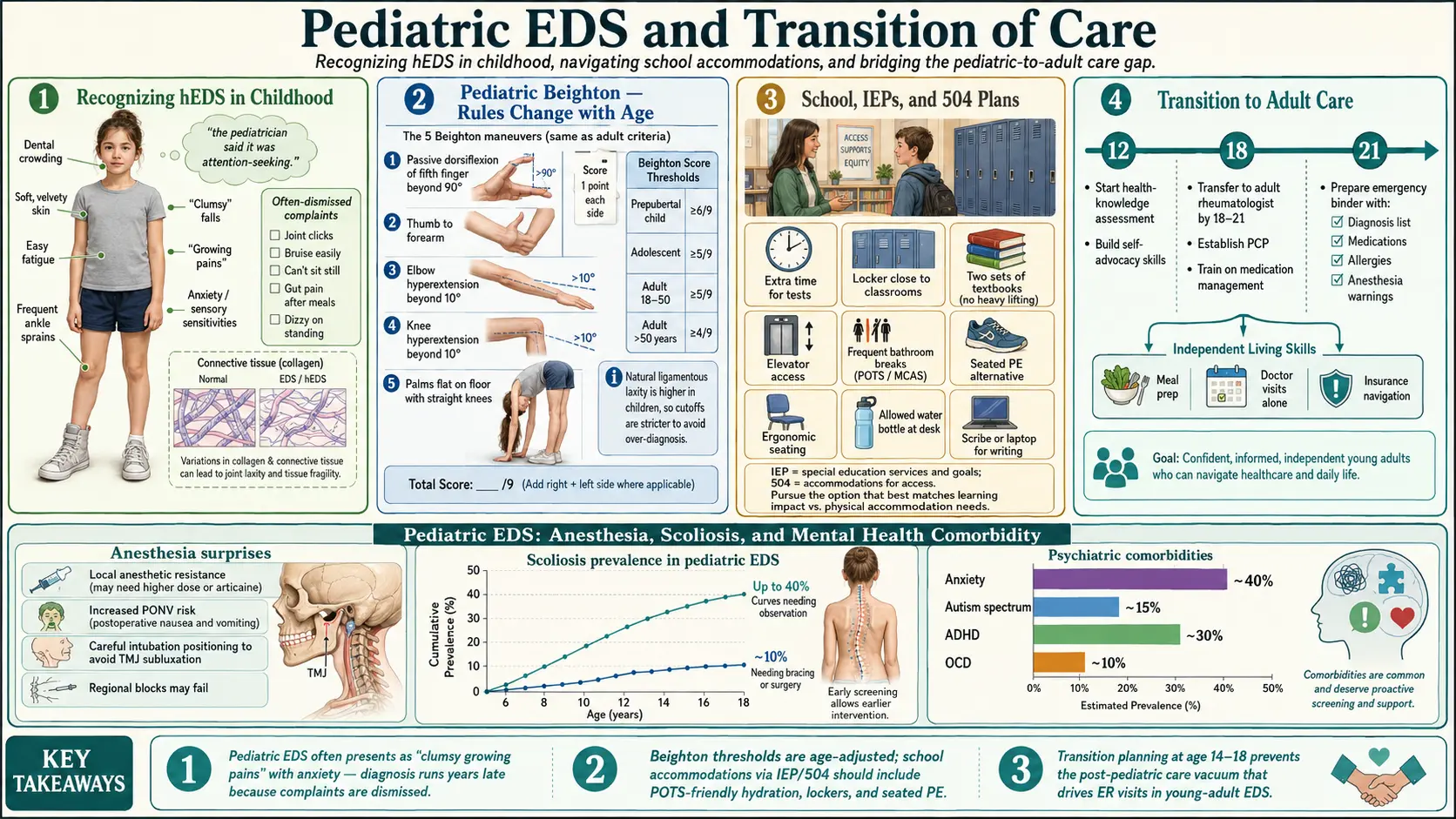
Table of Contents
- Recognizing hEDS in Childhood and Adolescence
- Common Complaints That Get Dismissed
- Pediatric Beighton — Why the Rules Change with Age
- Establishing the Diagnosis in a Child
- Anesthesia, Dental, and Surgical Surprises
- Scoliosis Screening
- School, IEPs, and 504 Plans
- Growth Spurts and the Teen Flare
- Mental Health and Neurodevelopmental Overlap
- Managing a Pediatric EDS Family
- The Transition to Adult Care
- Independent Living Skills
- College, Sports, and Career Planning
- Emergency Preparedness
- Key Research Papers
- Connections
- Featured Videos
Recognizing hEDS in Childhood and Adolescence
For decades pediatricians have used the phrase "benign joint hypermobility of childhood" to reassure parents that a bendy toddler will grow out of it. Many do. A meaningful minority do not — they grow into teenagers with hypermobile Ehlers-Danlos syndrome (hEDS) and the full constellation of pain, fatigue, dysautonomia, and GI symptoms that goes with it. The word "benign" can delay a useful diagnosis by ten or fifteen years.
Early clues, often overlooked, include:
- Delayed motor milestones. Late walkers (after 15 months), children who skip crawling, toddlers who tire quickly on playgrounds.
- W-sitting. Sitting on the floor with legs folded behind in a W shape. Comfortable for hypermobile hips because the joints splay passively instead of requiring muscular support.
- "Floppy" posture. Slumping into chairs, draping over furniture, leaning against walls while standing in line.
- Frequent sprains and subluxations. Ankles that "roll" repeatedly, shoulders that pop out during routine play, fingers that bend backward alarmingly.
- "Growing pains" at night that do not resolve. Real growing pains fade by age 10-12. EDS pain intensifies through puberty.
- Flat feet and persistent toe-walking. Arches that collapse under weight; tippy-toe walking that continues past age 3 despite typical development otherwise.
- Poor handwriting. Grip instability makes the pencil wobble; fine-motor fatigue comes quickly and looks like laziness.
- Fatigue out of proportion to activity. A twenty-minute grocery run followed by a two-hour nap.
None of these is diagnostic alone. Taken together in a child with hypermobile joints and a family history of "clumsy," "bendy," or chronically painful relatives, they warrant a formal evaluation.
Common Complaints That Get Dismissed
Before a child with hEDS gets an accurate diagnosis, their symptoms are often reframed as behavioral or psychological. Parents hear, in sequence, some combination of: growing pains, conversion disorder, school avoidance, anxiety, malingering, Munchausen by proxy. This is not because individual clinicians are cruel. It is because the symptom pattern — multi-system, fluctuating, invisible on routine imaging, worse on days with a social trigger — looks exactly like a somatic presentation to someone who does not know EDS exists.
Keep a written symptom log with dates. Photograph subluxations, bruises, and skin findings. Bring the same parent to every visit. Ask for every recommendation and differential to be written in the chart. This is not adversarial; it is how you build a medical record that survives being handed off to the next provider who will read the last five lines and form an opinion in thirty seconds.
Pediatric Beighton — Why the Rules Change with Age
The Beighton score is the standard bedside measure of joint hypermobility: nine points awarded for specific maneuvers (fifth-finger hyperextension, thumb-to-forearm, elbow and knee hyperextension, palms-to-floor). In adults, five of nine signals generalized hypermobility. In children, the same score means much less.
Young children are naturally bendy. Their collagen is still maturing, and normal preschoolers routinely score 7 or 8 of 9. As the child grows, ligaments stiffen. The cutoff for "abnormal" hypermobility therefore has to tighten with age:
- Prepubertal children (up to about age 12): six or more of nine.
- Postpubertal adolescents and adults: five or more of nine.
- Adults over 50: four or more of nine (collagen continues to stiffen with age).
The Bulbena scale is a pediatric-friendly alternative developed in Spain. It uses ten signs, some of which (passive dorsiflexion of the foot, hip external rotation) are easier to elicit in a squirming four-year-old than the adult Beighton maneuvers. Either tool is acceptable — ask your clinician which they prefer and have them document the specific score in the chart, not just "hypermobile" or "not hypermobile."
Establishing the Diagnosis in a Child
A working hEDS diagnosis in a child usually takes three elements:
- Age-adjusted Beighton or Bulbena in the hypermobile range.
- Symptoms consistent with the condition — chronic pain in multiple joints, repeated sprains or subluxations, fatigue, skin that feels soft or stretchy, a family history of similar problems.
- Exclusion of other heritable connective-tissue disorders — most importantly Marfan syndrome, Loeys-Dietz syndrome, and the rarer EDS subtypes (classical, vascular, kyphoscoliotic). This is the job of a pediatric geneticist.
A pediatric geneticist referral is the single most valuable visit you can schedule. The geneticist will take a detailed family history, examine skin extensibility and scarring, measure arm-span-to-height ratio, inspect palate and teeth, and — crucially — decide whether genetic testing is indicated. Most children with suspected hEDS do not need a DNA test, because no gene has been consistently linked to hypermobile EDS. Genetic testing is indicated when:
- Skin shows classical-EDS features: fish-mouth scars on knees and elbows, doughy feel, marked stretchiness → test for COL5A1, COL5A2.
- Family history includes arterial aneurysm, arterial rupture, bowel perforation, or sudden death in a young relative → test for COL3A1 (vascular EDS). This is the test you never want to skip if the family history fits.
- Severe early-onset scoliosis with thin blue sclerae → test for PLOD1 (kyphoscoliotic EDS).
- Marfan-like body habitus → test for FBN1 and the Loeys-Dietz gene panel.
A negative panel does not rule out hEDS; it rules out the subtypes you would not want to miss.
Anesthesia, Dental, and Surgical Surprises
Children with EDS come up against the healthcare system most often for routine things — tonsillectomies, ear tubes, dental work, broken arms — and that is exactly where unexpected complications show up. Two patterns recur:
- Local anesthetic failure. Lidocaine for a dental cavity or a laceration repair sometimes wears off in ten minutes, or never fully numbs the area. The child is labeled dramatic. The anesthetic is real; EDS tissue appears to metabolize or distribute local agents differently, and many families describe the same pattern across generations. Ask the provider in advance for a larger volume, longer-acting agents (bupivacaine), or a regional block if the procedure warrants it.
- Prolonged bleeding and bruising. Platelet counts are usually normal, but capillary fragility and connective-tissue laxity cause extended oozing and impressive bruises after minor procedures. Warn the surgeon. Pre-op screening for von Willebrand disease is reasonable because VWD is overrepresented in EDS cohorts.
Dental issues are their own chapter. Expect: a high-arched palate, crowding that often requires orthodontics, delayed or ectopic tooth eruption, gum recession, and fragile oral tissue that tears on routine suction. Find a pediatric dentist who has seen EDS before and is willing to work slowly.
Scoliosis Screening
Scoliosis is more common in hEDS and much more common in kyphoscoliotic EDS. Every child with an EDS diagnosis should have a spinal exam at each well-child visit through adolescence, with an Adams forward-bend test and a scoliometer reading when curvature is suspected. Curves that progress rapidly during a growth spurt need a prompt pediatric orthopedic referral; bracing is most effective when started early in a skeletally immature spine. Scoliosis in an EDS child is also a reason to ask the geneticist to revisit the differential — severe early scoliosis shifts the probability toward kyphoscoliotic EDS or a Marfan-spectrum diagnosis.
School, IEPs, and 504 Plans
School is where chronic illness meets bureaucracy. Two legal tools exist in the United States:
- An IEP (Individualized Education Program), under the federal IDEA law, applies when the medical condition interferes with learning and specialized instruction is needed.
- A 504 Plan, under the Rehabilitation Act, applies when a student needs accommodations to access a regular curriculum — this is the usual route for EDS families.
Accommodations worth requesting in writing:
- Modified PE or adapted PE — no contact sports, no trampolines, no full-speed sprints; swimming and stationary bike are usually safe.
- Unlimited bathroom access without asking (GI and bladder urgency are real).
- Permission to carry a water bottle and snacks everywhere (blood sugar and POTS salt/fluid needs).
- Extra time on handwritten assignments and tests; access to a laptop, speech-to-text, or a note-taker when dysgraphia is significant.
- An elevator key in multi-story buildings.
- Permission for fidget tools, compression garments, braces, and seat cushions.
- A flexible attendance policy acknowledging medically excused absences.
- Two sets of textbooks — one at home, one in the classroom — so a heavy backpack does not aggravate shoulder and spine pain.
Chronic absenteeism is the norm, not an aberration. When a brick-and-mortar schedule becomes unsustainable, options include hybrid schedules, homebound instruction (usually triggered by a physician letter stating 15+ days of expected absence), online public charter schools, and college dual-enrollment. When the student reaches college, register with Disability Services (sometimes called DSPS or the Office of Accessibility) before classes begin, not after the first failing grade.
Growth Spurts and the Teen Flare
The single most predictable feature of pediatric EDS is the teen flare. Between roughly ages 13 and 15, during the rapid adolescent growth spurt, pain often escalates sharply. Joints that were bendy and slightly achy at age 10 become unstable and intensely painful at 14. Fatigue deepens. POTS frequently emerges for the first time as cardiovascular volume fails to keep up with the newly longer body. GI symptoms appear or worsen. Mental-health distress peaks alongside the physical one.
This is not regression or somatization; it is the predictable intersection of rapid skeletal growth, incomplete muscular support for newly long limbs, and adolescent cardiovascular/hormonal change. The flare is usually partially reversible once growth slows in the late teens, provided the child reaches that point with intact physical therapy habits, adequate mental-health support, and a functioning care team.
Mental Health and Neurodevelopmental Overlap
A growing research literature describes elevated rates of ADHD, autism spectrum, anxiety, depression, and PANS/PANDAS in EDS cohorts compared with the general population. The mechanisms are not fully understood; proposed links include shared connective-tissue effects on the central nervous system, chronic dysautonomia altering arousal regulation, and the sheer cumulative weight of chronic pain and medical invalidation on a developing brain.
Practically, this means two things. First, an EDS diagnosis does not exclude — and often accompanies — a neurodevelopmental diagnosis, and both should be evaluated and supported. Second, the anxiety and depression that show up in EDS teens are usually reactive — a reasonable response to pain, lost activities, missed school, and years of being disbelieved. A pediatric pain psychologist familiar with chronic illness is far more useful than a generalist who will default to "your symptoms are caused by anxiety." Cognitive-behavioral therapy and acceptance-and-commitment therapy have both been studied in pediatric chronic pain and both help when delivered by someone who takes the physical illness seriously.
Managing a Pediatric EDS Family
Having a chronically ill child reshapes an entire household. Common patterns:
- Parent exhaustion. One parent — usually but not always the mother — becomes the full-time medical project manager: appointments, insurance appeals, IEP meetings, prescription refills, advocacy phone calls. Burnout is the rule.
- Sibling dynamics. Healthy siblings alternately feel ignored, resentful, guilty, and frightened. They may become precociously caretaking or act out to get the share of attention their brother or sister receives automatically.
- Marital stress. Parents frequently disagree on how sick the child really is, how much to restrict activity, when to push and when to rest, and how to divide the caretaking labor.
The Ehlers-Danlos Society parent forum is a practical, unglamorous source of help: other parents who have been there, script templates for school letters, insurance-appeal strategies, and honest talk about marriage and sibling issues. Consider also a family therapist (for household dynamics, not the child's EDS) and respite care when available.
The Transition to Adult Care
Nothing in pediatric EDS falls through the cracks more reliably than the handoff from pediatric to adult care. The standard transition window is age 16 to 22, and it should be planned starting at 14, not scrambled in the waiting room on someone's eighteenth birthday.
A good transition includes:
- A warm handoff: the pediatric provider communicates directly with the adult provider, not just via chart notes.
- A written medical summary: diagnoses, medication list with doses and tried-and-failed history, subspecialist contacts, PT program, flare pattern, what works and what does not.
- An adult primary care physician who is at minimum EDS-aware (willing to learn) if not EDS-experienced. A short list can usually be crowdsourced from local EDS Facebook groups.
- Subspecialty re-establishment — adult rheumatology, cardiology for POTS, GI, pain management. Some pediatric subspecialists see patients up to age 21; others cut off at 18.
- Insurance planning. In the United States, a young adult can remain on a parent's health plan until age 26 under the ACA, but employer-sponsored plans vary, and dependent disability extensions require paperwork filed before the 26th birthday. Marketplace plans, Medicaid (income-based), and SSI/SSDI (disability-based) are the fallback options.
Ask the pediatric clinic whether they use a formal transition tool such as Got Transition or TRxANSITION. Both walk family and teen through the skills the adolescent needs before the handoff.
Independent Living Skills
The functional skills a healthy teen picks up by osmosis often have to be explicitly taught to a chronically ill one, because their parents have been doing everything medical on their behalf. Target skills to transfer gradually through high school:
- Medication self-management — ordering refills, using a pill organizer, tracking side effects.
- Scheduling and attending appointments alone; knowing when to bring a parent as a second set of ears.
- Reading an insurance card, understanding deductibles and copays, calling member services when a claim is denied.
- Deciding when and how to disclose a disability to an employer or a professor. Disclosure is legally optional in most settings but practically necessary to obtain accommodations.
- Driving modifications — grip aids on the steering wheel, prioritizing power steering when car-shopping, knowing when a shoulder subluxation makes driving unsafe for the day.
College, Sports, and Career Planning
Sports at the college level are usually a bad idea for an hEDS body. Low-impact activities — swimming, recumbent cycling, rowing on a machine with attention to form, Pilates — can be continued for life. Contact sports, heavy running, and gymnastics cause a trajectory of injury that the connective tissue does not recover from the way a typical athlete's does.
Career planning benefits from early honesty about which jobs are sustainable. Generally favorable: remote-eligible roles, knowledge work with flexible hours, creative fields that allow recovery days, teaching at levels that permit sitting, research and analytical work, medical and mental-health fields (many EDS patients become excellent clinicians). Generally difficult: nursing floor work, retail standing, restaurant and hospitality, construction, long-haul driving, surgery, any work with rigid eight-hour schedules and no flexibility for flares. Fertility and reproductive choices belong in the same conversation early — see the Pregnancy and EDS page for details on genetic counseling, pregnancy risk by subtype, and timing decisions.
Emergency Preparedness
Every EDS teen and young adult should carry an emergency contact card in their wallet and a copy in their phone's medical ID. It should list:
- Full diagnosis and subtype, with the name and contact of the diagnosing physician.
- Current medications with doses.
- Known allergies and anesthetic issues.
- Two emergency contacts with relationship noted.
- Any cardiac or vascular imaging results that would change ER management (for classical or vascular EDS patients especially).
- A short statement: "If I present confused or with chest, abdominal, or head pain, please consider EDS-related vascular or spinal emergencies and contact my specialist."
For families with vascular EDS, a hospitalization plan — which hospital, which surgeon, which vascular team — should be worked out in advance, not decided in an ambulance.
Key Research Papers
- Tinkle B, et al. Hypermobile Ehlers-Danlos syndrome (a.k.a. Ehlers-Danlos syndrome Type III and Ehlers-Danlos syndrome hypermobility type): Clinical description and natural history. Am J Med Genet C. 2017.
- Scheper MC, et al. Children with generalised joint hypermobility and musculoskeletal complaints: state of the art on diagnostics, clinical characteristics, and treatment. Clin Rehabil. 2015.
- Kovacic K, et al. Joint hypermobility: a common association with complex functional gastrointestinal disorders and pediatric dysautonomia. J Pediatr. 2018.
- Pacey V, et al. Generalized joint hypermobility and risk of lower limb joint injury during sport in children. Pediatr Int. 2010.
Live PubMed Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on pediatric EDS recognition, management, and the transition to adult care:
- Pediatric Ehlers-Danlos and joint hypermobility
- Beighton score age adjustment in children
- Bulbena hypermobility scale
- EDS and local anesthetic resistance
- Hypermobility and pediatric scoliosis
- EDS school accommodations and 504 plans
- EDS, autism, and ADHD overlap
- Pediatric-to-adult care transition in chronic illness
- Joint hypermobility and pediatric dysautonomia
Connections
- Ehlers-Danlos Syndrome
- Hypermobile EDS and 2017 Diagnostic Criteria
- Classical and Vascular EDS
- Craniocervical Instability and AAI
- GI Involvement in EDS
- POTS, MCAS and the EDS Triad
- Pain Management in hEDS
- Physical Therapy and Joint Protection
- Pregnancy and EDS
- POTS
- POTS-MCAS-EDS Triad
- MCAS
- Fibromyalgia
- Chronic Fatigue Syndrome
- Migraine
- Chronic Pain
- Anxiety