Physical Therapy and Joint Protection in EDS
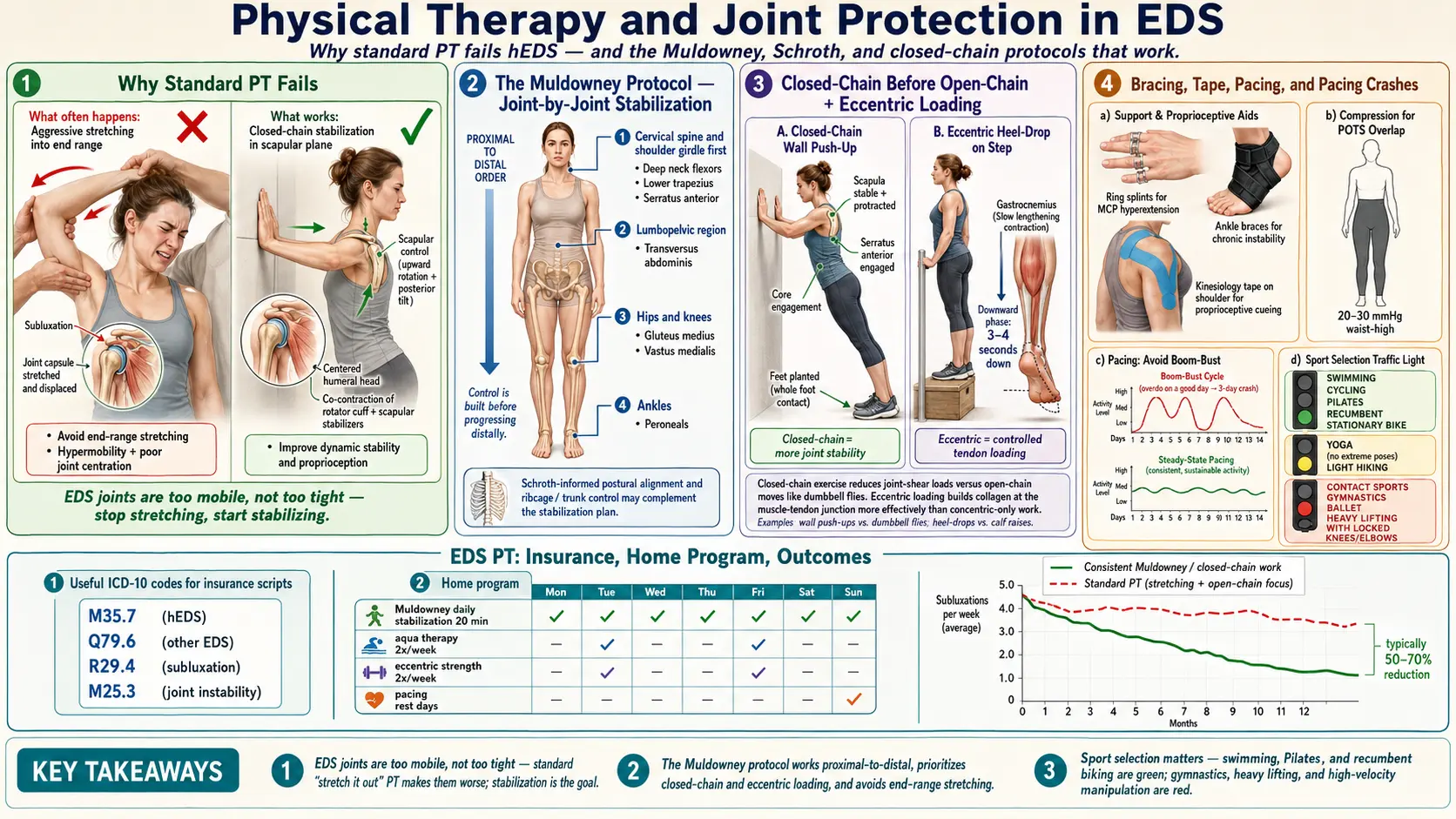
Table of Contents
- Why Standard PT Fails Many hEDS Patients
- The Muldowney Protocol
- The Schroth Method for Kyphoscoliotic EDS
- Joint-by-Joint Stabilization Principles
- Closed-Chain Before Open-Chain
- Eccentric-Focused Loading
- Aqua Therapy
- Pilates and Reformer Work
- Bracing, Splints, and Orthotics
- Kinesiology Tape and Compression Garments
- Pacing and the Post-Activity Crash
- What to Avoid
- Finding an EDS-Aware PT
- Insurance, ICD-10 Codes, and Scripts
- The Home Program
- Ergonomics — Desk, Sleep, and Daily Life
- Sport Selection — Safe, Caution, Avoid
- Return to Exercise After a Flare
- Key Research Papers
- Connections
- Featured Videos
Why Standard PT Fails Many hEDS Patients
If you have hypermobile Ehlers-Danlos Syndrome and a previous round of physical therapy left you worse, you are not imagining it, not weak, and not failing. Generic orthopedic PT is built for a population whose joints need more mobility and more stretch. Yours do not. Your ligaments and joint capsules are already lax — the problem is not range of motion, it is control of the range you have. Push an hEDS patient into end-range hamstring stretches, pec-minor stretches, or aggressive hip flexor lengthening, and you are prying apart tissue that is already too loose. The short-term relief of a "good stretch" is followed by days of subluxations, flares, and cascading pain.
The second failure mode is strengthening without proprioception. A trainer prescribes squats, rows, and deadlifts; the patient's form looks off but tolerable; three weeks later the knees buckle inward, the low back spasms, or a shoulder pops out reaching for a coffee mug. The muscles grew stronger but the brain never learned where the joint actually was in space. In hEDS, proprioception — joint position sense — is measurably impaired (see the Rombaut and Palmer papers below). Strength without position sense is a loaded gun with a broken sight.
A good hEDS physical therapy program is built on three premises. First, stop stretching; you are already stretchy. Second, train the small stabilizing muscles that cross individual joints before adding any whole-body load. Third, retrain the brain-to-joint signal with balance and proprioceptive drills in every single session. The programs that work — Muldowney, Levine-style, and the protocols emerging from The Ehlers-Danlos Society — all share this backbone.
The Muldowney Protocol
Kevin Muldowney, a Rhode Island physical therapist, published Living Life to the Fullest with Ehlers-Danlos Syndrome in 2015 after a decade of trial-and-error with hEDS patients. The protocol is a four-phase graded program that takes months, not weeks, and that asks for consistency over intensity.
Phase 1 — Closed-chain stabilization. The patient lies on a mat or sits supported; the therapist works one joint at a time, teaching the surrounding stabilizers to fire in isolation. Hip stabilization comes first because the pelvis is the platform for everything above and below. Supine bridges with a block between the knees, clamshells with a resistance band, and single-leg stands against a wall are the early building blocks. No barbell, no free weights, no cardio machines. Weeks, not days.
Phase 2 — Isometric hold work. Once each joint can be moved through a small controlled arc, the work shifts to holding position against gentle resistance. Isometrics (muscle contracts without joint movement) build tendon stiffness and neural drive without stressing lax capsules. Think wall-sits at a shallow angle, glute-bridge holds, and scapular retraction holds with a band. Holds of 10 to 30 seconds, repeated through the day.
Phase 3 — Controlled mid-range movement. Now the patient works through the middle of each joint's range, stopping well before end-range. Mid-range squats to a chair (not a deep squat), mid-range rows, mid-range step-ups. Slow eccentrics. Pause at the bottom. This is where most hEDS patients fail when they try to skip ahead from a gym program — they go straight to full-range lifts without the stabilization base.
Phase 4 — Return to activity. Only after the earlier phases hold up does the patient reintroduce sport, hiking, dance, or recreational lifting. The point is not to avoid activity forever; it is to earn the right to do it without subluxating.
The Muldowney book is not a substitute for a therapist, but it is a realistic roadmap patients can bring to their PT to set expectations. If your therapist has never heard of it, consider that a yellow flag.
The Schroth Method for Kyphoscoliotic EDS
The Schroth Method was developed in Germany in the 1920s for idiopathic scoliosis and remains the most evidence-based conservative approach for spinal curvature. For patients with kyphoscoliotic EDS (kEDS) or hEDS with secondary scoliosis, a Schroth-certified PT can be transformative. The method uses three-dimensional corrective breathing, mirror-guided postural re-training, and isometric holds in a corrected posture to de-rotate and stabilize the spine. Certification is real and checkable — search the Barcelona Scoliosis Physical Therapy School (BSPTS) or Schroth Best Practice directories. Schroth is not appropriate as general EDS PT; it is specific to scoliotic patterns.
Joint-by-Joint Stabilization Principles
The most useful clinical habit in hEDS is mapping your own instability. Every body is different. Instead of a generic "full-body strengthening" program, a good PT walks through each quadrant and identifies which joints sublux, which pop, which ache at night, and which feel stable. Common hot spots:
- Shoulders. Often the worst offender. The glenohumeral joint is a shallow socket held in by the rotator cuff and capsule. In hEDS both are lax. Train serratus anterior, lower trapezius, and the rotator cuff in tiny ranges with low load. Wall slides, scapular retraction against a band, and prone Y-T-W holds are staples.
- Pelvis and SI joint. Unilateral sacroiliac pain, "clunking" when rolling over in bed, a sense the hip is "out." Gluteus medius and deep core (transversus abdominis, pelvic floor) are the targets. An SI belt during flares can be a game-changer.
- Knees. Patellar subluxation, especially medial-to-lateral tracking problems. Vastus medialis oblique (VMO) and gluteus medius work together to hold alignment. Terminal knee extensions with a band, step-downs, and single-leg bridges.
- Ankles. Chronic sprains, rolled ankles, weak peroneals. Single-leg balance on a firm surface, then foam, then wobble board. Towel scrunches and resisted eversion.
- Cervical spine. Craniocervical instability (CCI) is a serious subgroup — do not load the neck without imaging and a specialist opinion. For uncomplicated cervical hypermobility, deep neck flexor training with a pressure biofeedback cuff is the foundation.
- TMJ. Jaw subluxation, clicking, and locking. A TMJ-trained PT or dentist can teach tongue-posture and controlled mouth-opening drills. Avoid wide yawns, big bites, and gum.
The rule across every joint is the same: train the stabilizers, not the mobilizers. Retrain proprioception with wobble boards, foam pads, BOSU balls, and eyes-closed balance drills. Avoid passive end-range stretches that lengthen tissue you need to keep short.
Closed-Chain Before Open-Chain
A closed-chain exercise is one in which the working hand or foot is fixed against a surface — push-ups, squats, step-ups, planks. Open-chain exercises move the limb through the air — bench press, leg extensions, dumbbell curls. Closed-chain movements co-contract the muscles on both sides of a joint, which produces joint compression and stability. Open-chain movements shear the joint. For hEDS, closed-chain is the default and open-chain is earned later, if at all.
Practical translation: a wall push-up is safer than a dumbbell bench press. A wall-supported squat is safer than a leg-extension machine. A plank is safer than a sit-up. Start closed-chain, graduate to partial open-chain with band resistance, and only add free weights when the joint has learned control.
Eccentric-Focused Loading
Eccentric contractions — the lengthening phase of a movement — build tendon stiffness and connective-tissue quality better than concentric work alone. For hEDS, this matters because your collagen is the problem; you want to give the tendons every possible signal to remodel toward stiffness rather than slack. Cue a 3- to 4-second lowering phase on every rep. Lower slowly out of a squat, lower slowly from a wall push-up, lower slowly on a step-down. Keep concentric (lifting) phases in the 1- to 2-second range. Research on Achilles and patellar tendons consistently shows eccentric programs outperform concentric-only programs for tendon health.
Aqua Therapy
Warm-water therapy pools (typically 90 to 94 F) are among the single best environments for hEDS exercise. Buoyancy offloads gravity — a neck-deep patient bears roughly 10% of their body weight — which lets you move without compressing painful joints. The warm water soothes mast cells in patients with the POTS/MCAS triad, and water resistance is gentle and three-dimensional, matching the drag to the speed of your movement. Walking forward, backward, and sideways in chest-deep water; gentle flutter kicks holding the pool edge; and light arm sweeps against the water are good starting points. Avoid very cold pools — they trigger muscle guarding and POTS symptoms. Check local hospitals and YMCAs for therapy pools; Medicare often covers aqua therapy when prescribed as PT.
Pilates and Reformer Work
Pilates — particularly reformer-based Pilates with an instructor trained in hypermobility — is one of the few movement disciplines that naturally matches hEDS needs. The reformer provides spring resistance that is graduated and controllable, supports the spine in a range of positions, and encourages small-muscle control before whole-body movement. The non-negotiable is the instructor. A general Pilates teacher may cue "lengthen, lengthen, lengthen" and push you into end-range positions that wreck a lax spine. Look for instructors certified by Polestar Pilates, Balanced Body, or STOTT who advertise hypermobility experience.
For patients with craniocervical instability or suspected CCI, avoid aggressive spinal flexion movements (roll-ups, neck curls, chest-lifts). Work with a neurosurgeon-informed PT before any loaded spinal flexion.
Bracing, Splints, and Orthotics
Bracing is controversial in hEDS because prolonged passive support weakens the muscles around the joint. The right frame is situational and time-limited. Bracing is appropriate:
- During an acute flare or subluxation, to restore proprioceptive input and offload pain.
- During specific high-demand tasks (long walks, travel, carrying groceries) in patients whose joints still fail with those loads.
- As a training wheel while PT progresses, with an explicit plan to wean.
Bracing is not appropriate as a permanent substitute for stabilization training. Specific options patients find useful:
- Custom ankle braces (lace-up or articulated) for chronic lateral instability.
- SI belts (Serola, Scosche) for sacroiliac flares — worn during activity, removed at rest.
- Cervical collars (soft foam or Philadelphia) for neck flares only — long-term daily wear weakens deep neck flexors and can worsen instability.
- Finger ring splints — Oval-8 (inexpensive plastic, great for trialing) and Silver Ring Splints (custom-sized, jewelry-grade, durable). They prevent hyperextension at PIP and DIP joints and are the single highest-ROI intervention for hand-dominant work such as typing, writing, and cooking.
- Custom foot orthotics for patients with pes planus, over-pronation, or posterior tibial tendon strain.
Kinesiology Tape and Compression Garments
Kinesiology tape (KT Tape, RockTape) does not structurally hold a joint in place — it provides sensory feedback. For hEDS patients with impaired proprioception, that tactile input can be enough to help the nervous system recruit the right stabilizer at the right moment. Patellar tracking tape, shoulder-posture tape, and SI-joint tape are common applications. Expect 2 to 4 days of wear per application.
Compression garments serve double duty. For patients with co-morbid POTS, medical-grade compression (20 to 30 mmHg) reduces venous pooling; see the POTS compression and exercise program for specifics. For hEDS, the same garment provides continuous proprioceptive input to the skin and soft tissues, subtly improving joint position sense. Trusted brands include Juzo, Mediven, Sigvaris, and for lighter-duty daytime wear Tommie Copper. Waist-high or thigh-high is more effective than knee-high for POTS support. Abdominal binders add splanchnic compression for patients with significant GI symptoms.
Pacing and the Post-Activity Crash
Many hEDS patients have overlapping POTS, ME/CFS-like fatigue, or fibromyalgia, and will flare for days after a single overzealous workout. The solution is graded, heart-rate-aware pacing — the same framework detailed in the fibromyalgia exercise pacing article and the POTS exercise program. Short, frequent sessions beat one long workout. Stop while you still have gas in the tank. Track heart rate and cap intensity below the level that triggers post-exertional malaise.
What to Avoid
- Chiropractic high-velocity low-amplitude (HVLA) manipulation. The thrust techniques chiropractors use on a stable neck or back can cause frank dislocations and vertebral artery injury in hEDS. Soft tissue work, instrument-assisted techniques, and gentle mobilization may be acceptable with an EDS-literate practitioner — but no thrusts, ever, especially cervical.
- Aggressive or contortion-style yoga. Going deeper into a pose is the wrong direction. If you do yoga, do it with an instructor who will actively cue you to shorten instead of lengthen, stay well shy of end range, and skip inversions if CCI is a concern.
- End-range ballet, gymnastics, or cheerleading past adolescence without medical supervision. Many hEDS patients were praised for their flexibility as children; continuing those disciplines into adulthood accelerates joint damage.
- Acupuncture directly into lax joint capsules is an uncommon but real source of bleeding or joint aggravation. Acupuncture in muscle bellies is generally fine; ask before needling near a joint line.
- Competitive powerlifting and contact sports carry a high risk-to-reward ratio for hEDS joints. If the goal is strength, train strength the Muldowney way, not the one-rep-max way.
Finding an EDS-Aware PT
The single biggest determinant of PT success in hEDS is the therapist. Tools for finding one:
- The Ehlers-Danlos Society Healthcare Professionals Directory (ehlers-danlos.com) — searchable by specialty and country.
- Chopra Center / Chopra Physiatry and the Muldowney Physical Therapy referral network.
- Patient groups on social media (EDS Wellness, The Zebra Network) for local recommendations.
- Interview your candidate PT by phone before the first appointment. Ask: "Have you treated hEDS before? Are you familiar with the Muldowney protocol? Do you use end-range stretching in your programs?" The answer to the last should be "rarely, and not for this population."
Insurance, ICD-10 Codes, and Scripts
Insurance often caps PT visits per year (20 to 30 is common). Make every visit count and make sure the script gets approved on the first pass. Relevant ICD-10 codes:
- Q79.6 — Ehlers-Danlos syndromes (unspecified).
- Q79.60 — Ehlers-Danlos syndrome, unspecified (2024 revision).
- Q79.62 — hypermobile Ehlers-Danlos syndrome (where available).
- M35.7 — Hypermobility syndrome.
- M25.3 — Other instability of joint (useful as a secondary code).
- M62.81 — Muscle weakness, generalized.
- R26.81 — Unsteadiness on feet (for balance/proprioception work).
Ask your prescribing physician to include the specific joint codes that are flaring (e.g., M25.312 for left shoulder instability) plus a goal statement like "proprioceptive retraining and stabilization, joint protection education." Pure "chronic pain" codes trigger denials more often than specific instability codes. If you exhaust visits, consider cash-pay packages with an EDS-literate PT — often cheaper per hour than insurance co-pays once deductibles are counted.
The Home Program
The home program is where recovery actually happens. Clinic visits teach technique; the work between visits creates adaptation. Realistic pragmatics:
- 20 to 30 minutes per day, scheduled like medication. A 90-minute Saturday session does not replace six 15-minute weekday sessions.
- Priorities, in order: core (transversus abdominis, pelvic floor, deep spinal stabilizers); gluteals (medius, maximus); scapular stabilizers (lower trap, serratus, rhomboids). These three complexes anchor everything else.
- Bed-based isometrics on flare days. Do not skip on bad days — scale down. Glute squeezes, quad sets, supine diaphragmatic breathing, and gentle scapular retractions can all be done flat on your back.
- Log sessions. A simple checkbox calendar is enough. Patterns — "my shoulders always feel worst after a gap of more than two days" — emerge within weeks.
- Progress slowly. If an exercise goes well for 10 to 14 days, add one variable (reps, hold time, or a slightly harder variation) — not three variables at once.
Ergonomics — Desk, Sleep, and Daily Life
Exercise is two percent of the day. The other 98 percent decides whether your joints survive. Ergonomic wins for hEDS:
- Chair with full arm support so your shoulders can let go of the keyboard. Armrests at elbow height, not an inch below.
- Standing desk with an anti-fatigue mat. Alternate sit and stand every 30 to 45 minutes. Lock your knees off when standing — micro-bends protect hypermobile knees.
- External keyboard and monitor raised to eye level. No laptop-on-lap hunching — it crushes the cervical spine.
- Sleep setup. A medium-firm mattress; a pillow that fills the gap between shoulder and ear without tipping the head; a pillow between the knees for side-sleepers; a small lumbar roll or pillow under the low back for back-sleepers. Avoid stomach-sleeping — it hyper-rotates the neck.
- Kitchen and bathroom. Lever door handles, bigger-grip utensils, electric can opener, jar openers. Anything that reduces thumb and wrist strain on a lax CMC joint is worth the money.
- Driving. Seat upright, lumbar support, ten-and-two grip (not white-knuckle), take breaks every 60 to 90 minutes.
Sport Selection — Safe, Caution, Avoid
Generally safe. Swimming (especially backstroke and sidestroke; avoid aggressive butterfly). Stationary cycling and recumbent elliptical. Walking, including Nordic walking with poles. Tai Chi and Qigong. Hatha yoga with a hypermobility-aware teacher. Aqua therapy.
Caution. Moderate-load weight training with strict form and a trainer who understands hypermobility. Hiking on smooth terrain with trekking poles. Recreational dance with no deep back-bends or aggressive turns. Road cycling on good roads (watch for wrist and neck strain on drop bars).
Avoid or strongly limit. Contact sports (football, rugby, hockey, martial arts with throws). Gymnastics, cheerleading, and ballet past adolescence without medical clearance. Competitive powerlifting. CrossFit-style high-rep Olympic lifting. Trampolines. Running long distances on hard surfaces (short, soft-surface runs may be tolerable).
Return to Exercise After a Flare
When a flare resolves, the temptation is to pick up where you left off. Don't. Restart at roughly 25% of pre-flare volume and intensity, and rebuild over two to three weeks. A four-day flare can cost a week of deconditioning; pushing back to 100% on day one triggers the next flare within 72 hours. This is the single most common self-sabotage pattern in hEDS rehab. Label it, expect it, and pre-commit to the 25% rule before the flare starts.
Key Research Papers
- Rombaut L, et al. Muscle strength, proprioception, and functional ability in patients with hypermobility type Ehlers-Danlos syndrome. BMC Musculoskelet Disord. 2012.
- Palmer S, et al. The effectiveness of therapeutic exercise for joint hypermobility syndrome: a systematic review. Am J Med Genet C. 2014.
- Castori M. Ehlers-Danlos syndrome, hypermobility type: an underdiagnosed hereditary connective tissue disorder with mucocutaneous, articular, and systemic manifestations. Dermatol Ther. 2012.
- Keer R, Simmonds J. Joint protection and physical rehabilitation of the adult with hypermobility syndrome. Curr Opin Rheumatol. 2011.
Live PubMed Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on rehabilitation and joint protection in Ehlers-Danlos Syndrome:
- Ehlers-Danlos and physical therapy
- Hypermobility, proprioception, and rehabilitation
- Hypermobility and closed-chain exercise
- Ehlers-Danlos and aquatic therapy
- Schroth method and kyphoscoliotic curves
- Hypermobility, bracing, and splinting
- Ehlers-Danlos and craniocervical instability
- Eccentric exercise and tendon collagen remodeling
Connections
- Ehlers-Danlos Syndrome
- Hypermobile EDS and 2017 Diagnostic Criteria
- Classical and Vascular EDS
- Craniocervical Instability and AAI
- GI Involvement in EDS
- POTS, MCAS and the EDS Triad
- Pain Management in hEDS
- Pediatric EDS and Transition of Care
- Pregnancy and EDS
- POTS
- POTS Compression and Exercise Program
- Fibromyalgia
- Exercise Pacing and Graded Movement
- Osteoporosis
- Arthritis
- Collagen