Pain Management in Hypermobile EDS
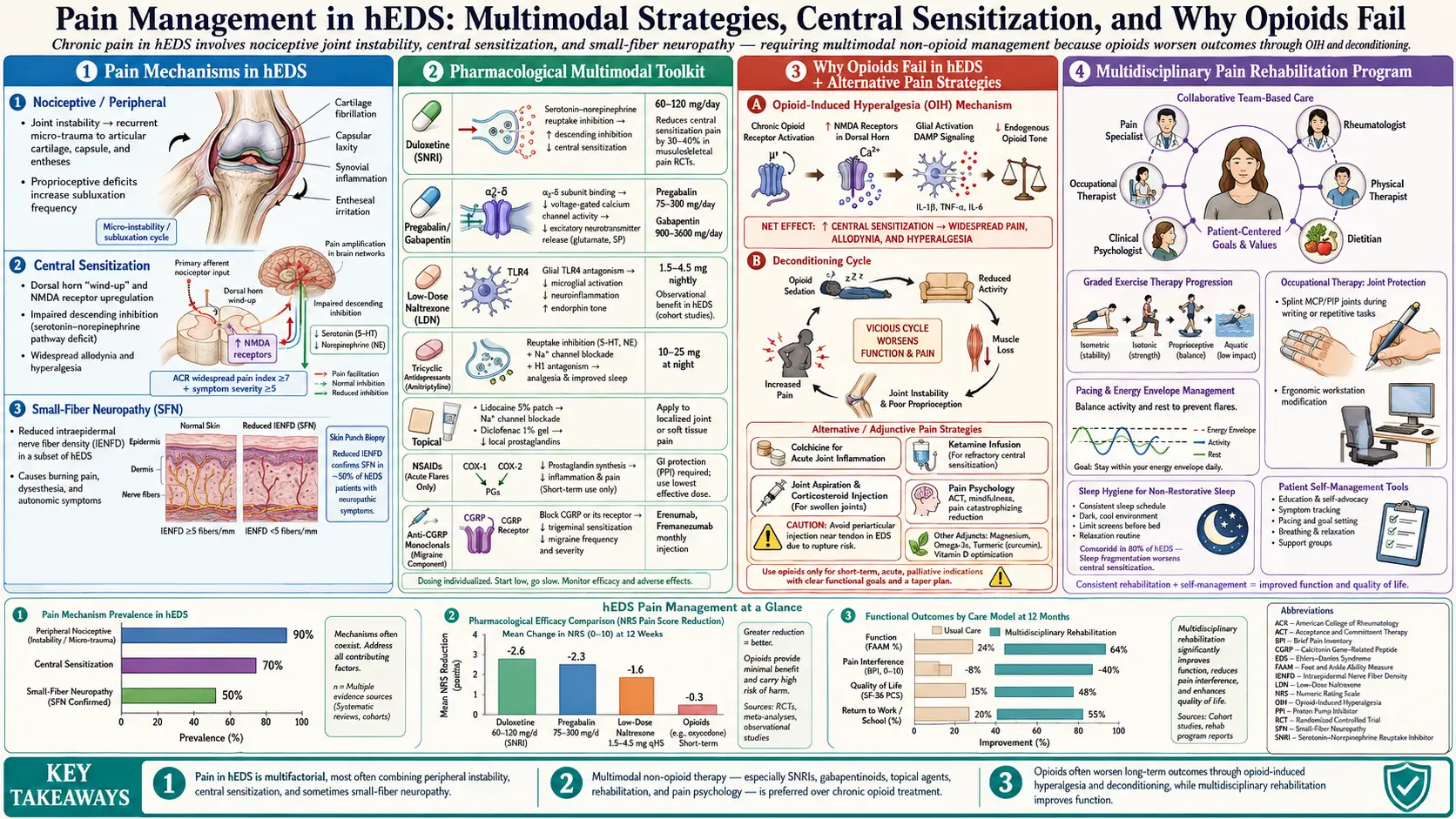
Table of Contents
- Four Kinds of Pain in One Body
- The Fibromyalgia Overlap
- Over-the-Counter and Topical Basics
- SNRIs and Low-Dose TCAs
- Gabapentin and Pregabalin
- Low-Dose Naltrexone
- Medical Cannabis
- Opioids — The Honest Conversation
- Interventional Pain Procedures
- What Not to Do
- Non-Pharmacologic Anchors
- Mind-Body and Nervous System Work
- Sleep — The Pain Amplifier You Can Actually Adjust
- Dental and TMJ Pain
- Headache and Migraine Overlap
- Mental Health as a Pain Lever
- Building Your Team
- Key Research Papers
- Connections
- Featured Videos
Four Kinds of Pain in One Body
If you have hypermobile Ehlers-Danlos syndrome, the most maddening thing about your pain is that it refuses to sit in one category. A single bad afternoon can include a grinding hip that just partially dislocated, a knot of muscle between your shoulder blades that feels like a rock, a burning nerve down your forearm, and a strange whole-body ache that feels unreasonable given what you actually did that morning. That is not four different problems. It is four mechanisms of pain happening simultaneously in the same connective-tissue disorder, and naming each of them is the first step toward treating it.
1. Nociceptive pain is the straightforward kind: your joint subluxes, the capsule stretches, tiny tears occur in ligament fibers, local inflammatory chemicals fire, and pain receptors in the joint send the signal up. This is what hurts after a partial dislocation of your shoulder, a twisted ankle, or an over-extended knee. It resolves when the tissue heals — except in hEDS, where the joint is unstable enough that the next sublux happens before the last one finished healing, and the nociceptive input never fully switches off.
2. Myofascial pain is the muscles doing a job they were never designed for. In a body with lax ligaments, the ligaments cannot hold your joints in their correct alignment, so your muscles take over as the stabilizers. Muscles are not built for continuous low-grade co-contraction; they were built to fire and relax. Asked to hold a joint in place all day every day, they knot, form trigger points, develop referred-pain patterns, and produce the thick ropy bands under your skin that your massage therapist keeps pointing out. This is why hEDS patients often describe pain "everywhere the muscles are," not just "where the joints are."
3. Neuropathic pain shows up as burning, electric, shooting, or pins-and-needles sensations. It has two main sources in hEDS. The first is nerve entrapment — a nerve pinched as it passes through a joint or muscle compartment that is now geometrically abnormal because of laxity. Thoracic outlet syndrome, ulnar nerve compression at the elbow, and piriformis entrapment of the sciatic nerve are classic hEDS presentations. The second is small-fiber neuropathy, in which the tiny unmyelinated nerve fibers in your skin are sparse or dysfunctional. Skin biopsy studies in hEDS cohorts have documented reduced intraepidermal nerve fiber density in a significant minority of patients, which explains the bizarre stocking-glove burning that has no obvious structural cause.
4. Central sensitization is the brain and spinal cord's response to years of inputs one, two, and three. The pain-processing circuitry in the central nervous system up-regulates. Signals that should not hurt (a light touch, a warm shower) now hurt. The pain you do feel lingers longer than the injury. The volume knob on pain, essentially, has been turned up and glued in place. This is not "in your head" — it is measurable neuroplastic change, the same mechanism that underlies fibromyalgia.
Any serious pain plan for hEDS has to address all four. Treating only the joint while ignoring the muscles, or only the muscles while ignoring the nervous system, guarantees partial failure.
The Fibromyalgia Overlap
A remarkable proportion of hEDS patients — studies put it between 30% and 80% depending on cohort — also meet full ACR criteria for fibromyalgia. That is not a coincidence, and it is not a second diagnosis stacked on for convenience. It is the predictable consequence of decades of joint and muscle input wiring the central nervous system into a sensitized state.
The practical consequence: many of the best tools for hEDS pain come from the fibromyalgia playbook, because fibromyalgia research has spent decades on exactly the problem of central sensitization. Duloxetine, low-dose amitriptyline, pregabalin, graded exercise, CBT for chronic pain, and low-dose naltrexone all have fibromyalgia evidence bases and all translate reasonably to hEDS. If your rheumatologist will not touch your pain because "EDS doesn't cause that much pain," ask to be treated for your overlapping fibromyalgia. Same problem, different door.
Over-the-Counter and Topical Basics
NSAIDs — ibuprofen, naproxen, diclofenac, celecoxib — work for nociceptive flare pain after a sublux or soft-tissue injury. The hEDS-specific caution is GI fragility. A large subset of patients have overlapping gastroparesis, reflux, or functional GI disease (see GI involvement in EDS), and NSAIDs can erode an already-vulnerable gut lining. Take them with food, pair with a proton-pump inhibitor for courses longer than a few days, and do not use them daily without a plan. In vascular EDS, avoid NSAIDs entirely — antiplatelet effects plus fragile arterial walls is a dangerous combination.
Acetaminophen is the quiet workhorse. Up to 3,000 mg per day, split into regular doses, gives a gentle analgesic baseline with very little GI or cardiovascular risk. It will not abolish a bad flare, but as a floor under everything else it reduces how much you need from the other drugs.
Topicals are under-used in hEDS. Diclofenac gel (1% or 2%) delivers an NSAID straight to a painful joint with a fraction of the systemic exposure of oral ibuprofen. Lidocaine 5% patches sit over myofascial trigger points or nerve-entrapment areas and numb the skin's pain signaling without drowsiness. Both are useful for patients who cannot tolerate oral NSAIDs or who want to keep systemic drug burden low.
SNRIs and Low-Dose TCAs
Two drug classes sit at the center of modern hEDS pain pharmacology, and both came out of fibromyalgia and neuropathic-pain research.
Duloxetine (Cymbalta) at 30–60 mg once daily modulates descending pain inhibition by raising serotonin and norepinephrine in the spinal cord. It reduces the central-sensitization component of pain, independent of any antidepressant effect. Venlafaxine (Effexor) at 75–225 mg is a close cousin and has an additional practical advantage for some EDS patients: at higher doses it supports blood pressure and can help orthostatic hypotension (distinct from POTS, which is a tachycardia problem — venlafaxine does not treat POTS itself). Both drugs need slow titration and slow taper; stopping abruptly causes unpleasant discontinuation symptoms.
Tricyclic antidepressants at low doses — amitriptyline 10–25 mg or nortriptyline 10–25 mg taken two hours before bed — are an old, cheap, and still-useful tool. At these doses they are not acting as antidepressants; they damp neuropathic firing, deepen sleep, and reduce the next morning's pain levels. Nortriptyline is generally better tolerated than amitriptyline because it has less anticholinergic drag (less dry mouth, constipation, grogginess). For patients with hEDS plus gastroparesis, the anticholinergic load of amitriptyline can worsen gut motility — nortriptyline is a cleaner first choice.
Gabapentin and Pregabalin
When the pain is primarily neuropathic — burning, electric, shooting, stocking-glove distribution — the gabapentinoids earn their place. Gabapentin starts at 100–300 mg at bedtime and can climb to 900–1,800 mg/day split into three doses. Pregabalin is a more potent cousin dosed at 75–150 mg twice daily. Both reduce abnormal firing in over-excited nerve fibers.
The downside is cognitive: brain fog, word-finding difficulty, and sedation are common. Many hEDS patients already live with fatigue and dysautonomia-related cognitive slowing, and stacking a gabapentinoid on top can tip them into functional impairment they cannot afford. Start low, titrate slowly, and be honest with yourself about whether the pain relief is worth the fog. If the first few weeks feel like trading a body problem for a brain problem, the drug is not right for you at that dose.
Low-Dose Naltrexone
Low-dose naltrexone (LDN) is one of the most interesting drugs in the hEDS toolkit. At standard doses (50 mg), naltrexone blocks opioid receptors and is used to treat alcohol and opioid dependence. At 1.5 to 4.5 mg once at bedtime, it does something completely different: it briefly blocks opioid receptors for a few hours, which triggers a rebound increase in the body's own endorphin production, and it inhibits microglial activation in the central nervous system. Microglia are the immune cells of the brain and spinal cord, and sustained microglial activation is a core driver of central sensitization.
LDN has an expanding evidence base in fibromyalgia, and case series and clinical experience increasingly support its use in hEDS specifically, where it appears to help both pain and the mast cell activation that frequently overlaps (see POTS, MCAS and the EDS triad). Typical titration: start 1.5 mg at bedtime, increase by 1.5 mg every two to four weeks up to 4.5 mg. The main side effect is vivid dreams in the first week or two, which usually settle. It is not addictive, does not cause tolerance, and is relatively cheap through compounding pharmacies ($30–$70/month). See the low-dose naltrexone hub for dosing details and sourcing.
Medical Cannabis
In states where it is legal, medical cannabis is a tool many hEDS patients use — especially for the myofascial and central-sensitization components of pain that respond poorly to everything else. Cannabinoids act on the endocannabinoid system, which is distributed throughout pain-processing circuits.
Practical points. THC:CBD ratios matter. High-THC products give more analgesia but more cognitive impairment and anxiety risk; high-CBD products are gentler but often insufficient for moderate-to-severe pain. A balanced 1:1 or 2:1 CBD:THC tincture taken sublingually is a common starting point for patients new to cannabis. Smoked and vaped products deserve extra caution in EDS: connective tissue fragility extends to the lungs, and the vaping-associated lung injury seen in recent years is a reminder that inhaled products carry real risk. Edibles and tinctures are cleaner routes of delivery. Cannabis is not a first-line drug, it is not universally helpful, and it interacts with other central nervous system drugs — but for a specific subset of patients it is genuinely useful.
Opioids — The Honest Conversation
The mainstream position — "avoid opioids in chronic non-cancer pain" — is a reaction to twenty years of over-prescribing and real harm. It is largely correct for hEDS, and the reasons are specific to this condition:
- Opioid-induced hyperalgesia. Long-term opioid use paradoxically increases pain sensitivity by altering the same central pain circuits that are already dysregulated in hEDS. You can end up with worse baseline pain on opioids than off them.
- Constipation. A large fraction of hEDS patients have baseline gastroparesis, slow-transit constipation, or dysautonomia-driven GI dysmotility. Opioids slow the gut further. What was "uncomfortable" becomes "unmanageable."
- Tolerance and escalation. Chronic daily use requires dose increases for the same relief, and tapering a hEDS patient off chronic opioids after years of use is grueling.
That said — severe breakthrough pain is real. A patient with a frankly dislocated shoulder, a rib that just subluxed and is grinding with every breath, or post-surgical pain in fragile tissue needs effective short-term analgesia, and pretending otherwise is cruel. Short courses of tramadol, hydrocodone, or oxycodone — days, not weeks — for defined injuries are appropriate and reasonable. What the evidence argues against is the daily long-term opioid prescription as a chronic pain management strategy. If you are already on chronic opioids and functioning, do not stop abruptly on the strength of this article; any taper should be collaborative, slow, and ideally supported by simultaneous introduction of LDN, SNRIs, or other alternative tools.
Interventional Pain Procedures
A pain physiatrist or interventional pain physician can add procedural tools to your medication plan. Options relevant to hEDS:
- Dry needling and trigger point injections. For myofascial knots in the shoulder girdle, paraspinals, and piriformis, these can produce dramatic short-term relief. Low risk, usually covered by insurance as physical therapy or pain procedures.
- Prolotherapy. Injection of an irritant solution (commonly dextrose) into a lax ligament or joint capsule with the goal of stimulating local collagen repair. Controversial — evidence is mixed and mostly from small trials — but some hEDS patients report meaningful stabilization of specific problem joints (especially SI joints, cervical spine facets). Usually not insurance-covered; expect $150–$500 per session, typically several sessions.
- Platelet-rich plasma (PRP). Emerging. Draws the patient's own blood, spins out a platelet concentrate rich in growth factors, and injects it into an injured tendon, ligament, or joint. Evidence is strongest in non-EDS tendinopathies; EDS-specific data are limited but some patients benefit. Generally $500–$1,500 per injection, out of pocket.
- Nerve blocks. Occipital nerve blocks for cervicogenic headache, stellate ganglion blocks for upper-limb complex regional pain syndrome, lumbar medial branch blocks for facet-driven back pain. These are reasonable but require a physician aware of hypermobility — a neck that is already ligamentously unstable does not need an aggressive needle technique.
- Cervical and craniocervical procedures. A subset of hEDS patients have craniocervical instability or Chiari-like symptoms, and in these people aggressive cervical interventional procedures can worsen things. If a procedure is proposed near the upper cervical spine, make sure the proceduralist knows about hEDS and has imaging of your craniocervical junction first.
What Not to Do
A short list of interventions that look helpful in non-hEDS back and neck pain but carry specific dangers in hypermobility:
- High-velocity, low-amplitude (HVLA) chiropractic adjustments. The dramatic "crack" manipulations of the spine. In a patient with already-lax ligaments, HVLA can worsen instability, push joints past their stable range, and in rare but documented cases cause vertebral or carotid artery dissection — a catastrophic risk, especially elevated in vascular EDS. Gentle mobilization, instrument-assisted techniques, or activator methods are acceptable alternatives if chiropractic is desired.
- Deep-tissue massage over unstable joints. Heavy pressure on a hypermobile thoracic outlet, cervical spine, or SI joint can trigger a sublux. Myofascial release, gentle trigger-point work, and positional release are safer.
- Aggressive stretching and "hyper-stretching" yoga. Patients with hEDS usually do not need more flexibility. They need stability. Advanced pretzel poses feel great in the moment and wreck joints over months.
- Prolonged bed rest. Every day of immobility increases central sensitization, deconditions stabilizer muscles, and worsens dysautonomia. Pain that keeps you in bed for more than a day needs active management.
Non-Pharmacologic Anchors
Drugs alone never solve hEDS pain. The non-drug anchors carry as much weight as the pharmacy:
- Graded movement within a stable range. See the physical therapy article for protocols. The core principle: strengthen the muscles that must now do the ligaments' job, avoid the ranges where the joint is unstable, progress slowly enough that the tissue adapts.
- Heat and ice. Heat for myofascial tightness, ice for acute sublux or inflammation. Cheap, effective, underused.
- Compression garments. Medical-grade compression (20–30 mmHg) in lower-body garments helps POTS by improving venous return and — importantly for pain — provides proprioceptive feedback to joints that cannot read their own position accurately. Upper-body compression shirts, SI joint belts, and shoulder stabilizers work the same way: they remind the joint where it is supposed to be.
- Aqua therapy. Water unweights joints, allowing movement without compressive load. A warm therapy pool (88–92°F) is better than a cold lap pool for hEDS; cold provokes muscle guarding.
- Float tanks. Sensory-deprivation flotation in Epsom salt water removes gravity, reduces afferent input, and for some patients produces hours-long pain relief. Not covered by insurance; roughly $60–$100/session.
- TENS units. Transcutaneous electrical nerve stimulation over a painful area gates pain signals at the spinal cord. Home units cost $30–$80 and are worth a trial.
Mind-Body and Nervous System Work
When a clinician mentions "mind-body" for chronic pain, many hEDS patients hear "they think it's psychological." That is not what the evidence says and not what this section means. Central sensitization is a neuroplastic change in the central nervous system — a physical change — and the tools that rewire it are behavioral.
Pacing is the foundation. The hEDS "push-crash" cycle — three good days, six bad days — flattens out dramatically when activity is paced against energy rather than against enthusiasm. Pacing sounds trivial and is one of the hardest things high-functioning patients ever learn.
Cognitive behavioral therapy for chronic pain (CBT-CP) has a strong evidence base for reducing disability and improving function. It is not "think away your pain." It is identifying catastrophic thought patterns, graded exposure to feared movements, and building a realistic relationship with a symptom that is not going away soon. Acceptance and Commitment Therapy (ACT) is a closely related approach focused on values-based action despite pain.
Vagal-tone work. Heart-rate variability (HRV) biofeedback, yoga nidra, slow paced breathing (six breaths per minute), and cold-water face immersion all increase parasympathetic tone. Higher vagal tone is correlated with lower pain sensitivity and better dysautonomia control. Avoid, however, the aggressive positional yoga practices that push hypermobile joints further into instability. Restorative yoga, yoga nidra (meditative, lying still), and gentle breath-focused practices are the right doors.
Sleep — The Pain Amplifier You Can Actually Adjust
One night of disrupted sleep measurably raises pain sensitivity the next day. Chronic poor sleep raises the baseline set-point of central pain circuits. Fix sleep and pain improves; ignore sleep and nothing else works as well.
The hEDS-specific sleep problems are mechanical and chemical. Mechanically, an unstable neck, shoulder, or hip keeps waking you up as you shift. A supportive pillow (cervical contour), a body pillow to prevent hip adduction, and side-lying with a pillow between the knees all help. Chemically, mast-cell activation produces nocturnal histamine surges that fragment sleep — if you have overlapping MCAS, an evening H1 antihistamine is often a game-changer. Thyroid dysfunction, which disproportionately overlaps with connective tissue disorders, also fragments sleep — if you have not had TSH, free T4, and antibodies checked recently, that is worth doing.
Dental and TMJ Pain
Temporomandibular joint dysfunction is extremely common in hEDS. The jaw is a joint; ligaments are lax; the articular disc subluxes or displaces; the surrounding muscles of mastication overwork and knot. Symptoms include clicking, locking, facial pain radiating to the ear, morning soreness, and headache.
Practical management: a soft night guard fitted by a dentist familiar with TMJ; gentle self-mobilization and jaw-opening exercises; avoiding foods that require wide opening (apples, thick sandwiches) during flares; and, for the myofascial component, trigger-point therapy to masseter and temporalis muscles. Avoid aggressive orthodontia that applies sustained force to already-lax dental ligaments — teeth can over-respond and drift unpredictably after treatment.
Headache and Migraine Overlap
Headache in hEDS has multiple generators: cervicogenic (from the upper cervical spine and suboccipital muscles), tension-type (from myofascial overwork of the head and neck), migraine (disproportionately prevalent in hEDS cohorts), and in a smaller subset, pressure-related headaches from craniocervical instability or intracranial hypertension/hypotension.
True migraine management in hEDS follows the standard migraine protocols: abortive triptans or gepants for acute attacks, preventive therapy (topiramate, CGRP inhibitors, beta-blockers — though beta-blockers can complicate POTS) when attacks exceed four per month. What is hEDS-specific is the need to distinguish headaches coming from the neck (which respond to cervical stability work, occipital nerve blocks, and myofascial treatment) from true migraine (which responds to migraine drugs). A pain physiatrist or headache neurologist who knows hypermobility is worth seeking out. Any new headache pattern that worsens lying down, is accompanied by positional changes in symptoms, or comes with neurological signs needs imaging, not another pain pill.
Mental Health as a Pain Lever
Depression roughly doubles the subjective intensity of any chronic pain condition. Anxiety tightens muscles, which worsens myofascial pain. PTSD — which accumulates in patients who have spent years being dismissed, misdiagnosed, or gaslit by the medical system — keeps the nervous system in sympathetic overdrive, which amplifies central sensitization.
Treating the mental health component is not an admission that the pain is imagined. It is recognition that mood circuits and pain circuits share anatomy and neurochemistry, and that you cannot turn the volume down on one without also turning the volume down on the other. A therapist who understands chronic illness (not every therapist does) can be as important to your pain plan as your rheumatologist. If you cannot afford in-person therapy, several validated CBT-CP and ACT workbooks exist and have evidence for self-directed use.
Building Your Team
Nobody manages hEDS pain alone, and nobody finds one doctor who does everything. The realistic team:
- A primary care physician willing to act as your quarterback — renewing prescriptions, coordinating specialists, taking your symptoms seriously. This is the single hardest role to fill and the most important.
- A pain physiatrist or pain management physician familiar with hEDS or at least with central sensitization. They run the medication optimization (SNRIs, LDN, gabapentinoids) and interventional procedures.
- A physical therapist familiar with hEDS. A PT who is going to hand you a resistance band and tell you to "strengthen your core" is not enough. You need someone who knows stabilization progressions, neuromuscular re-education, and when to hold back.
- A therapist familiar with chronic illness. Not "a therapist." Someone who has treated medically complex patients before, ideally with CBT-CP or ACT training.
- A rheumatologist or geneticist for diagnosis and surveillance — but do not expect them to run your pain day-to-day. Most do not want that role.
- Specialists as needed: cardiology for POTS, gastroenterology for GI symptoms, allergist/immunologist for mast cell issues, dentist for TMJ, ophthalmology if you have ocular involvement.
The team takes years to assemble. The fact that you do not have it yet is not your fault and not a failure. Start with the two people who will listen: usually a primary care physician and a PT. Build from there.
Key Research Papers
- Castori M, et al. Natural history and manifestations of the hypermobility type of Ehlers-Danlos syndrome. Disabil Rehabil. 2010.
- Rombaut L, et al. Chronic pain in patients with the hypermobility type of Ehlers-Danlos syndrome: evidence for generalized hyperalgesia. Clin Rheumatol. 2012.
- Chopra P, et al. Pain management in the Ehlers-Danlos syndromes. Am J Med Genet C Semin Med Genet. 2017.
- Younger J, et al. The use of low-dose naltrexone as a novel anti-inflammatory treatment for chronic pain. Clin Rheumatol. 2014.
Live PubMed Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on pain mechanisms and management in hypermobile EDS:
- Hypermobile EDS and chronic pain
- EDS and central sensitization
- EDS and small-fiber neuropathy
- Hypermobility and fibromyalgia overlap
- Low-dose naltrexone in fibromyalgia and chronic pain
- Duloxetine in chronic musculoskeletal pain
- EDS and temporomandibular joint dysfunction
- EDS, headache, and migraine
- Prolotherapy and joint instability
Connections
- Ehlers-Danlos Syndrome
- Hypermobile EDS and 2017 Diagnostic Criteria
- Classical and Vascular EDS
- Craniocervical Instability and AAI
- GI Involvement in EDS
- POTS, MCAS and the EDS Triad
- Pediatric EDS and Transition of Care
- Physical Therapy and Joint Protection
- Pregnancy and EDS
- Chronic Pain
- Fibromyalgia
- Central Sensitization Explained
- Low-Dose Naltrexone for Fibromyalgia
- Migraine
- POTS
- MCAS
- Low Dose Naltrexone
- Anxiety