Craniocervical Instability (CCI) & AAI in EDS
If you have Ehlers-Danlos syndrome and your neck feels like it cannot hold your head up — if the base of your skull pounds with every step, if bending forward makes your vision blur or your heart race, if lying flat is the only position that brings relief — you may be dealing with craniocervical instability (CCI) or atlantoaxial instability (AAI). These are real, measurable conditions in which the ligaments that normally lock your skull onto your spine have stretched enough to let the bones shift abnormally under the weight of your head.
This article is for patients. It explains the anatomy in plain language, lists the symptoms and the red flags that require urgent evaluation, walks through the imaging that can confirm the diagnosis, and gives an honest account of what conservative care and surgery actually involve. Most importantly: it urges caution. CCI surgery is irreversible, contested among neurosurgeons, and should be considered only at highly specialized centers and only after conservative care has failed and objective imaging proves instability.
Table of Contents
- The Ligaments That Hold Your Skull On
- Symptoms — What CCI and AAI Feel Like
- Red Flags for Myelopathy — Act Immediately
- The EDS Triad Plus — POTS, MCAS, and CCI
- Imaging — Why Supine MRI Often Misses CCI
- Key Measurements Your Radiologist Should Report
- Chiari Malformation and Overlap
- Conservative First-Line Care
- Surgical Fusion — An Honest Conversation
- Second Opinions and Choosing a Center
- Key Research Papers
- PubMed Topic Searches
- Connections
- Featured Videos
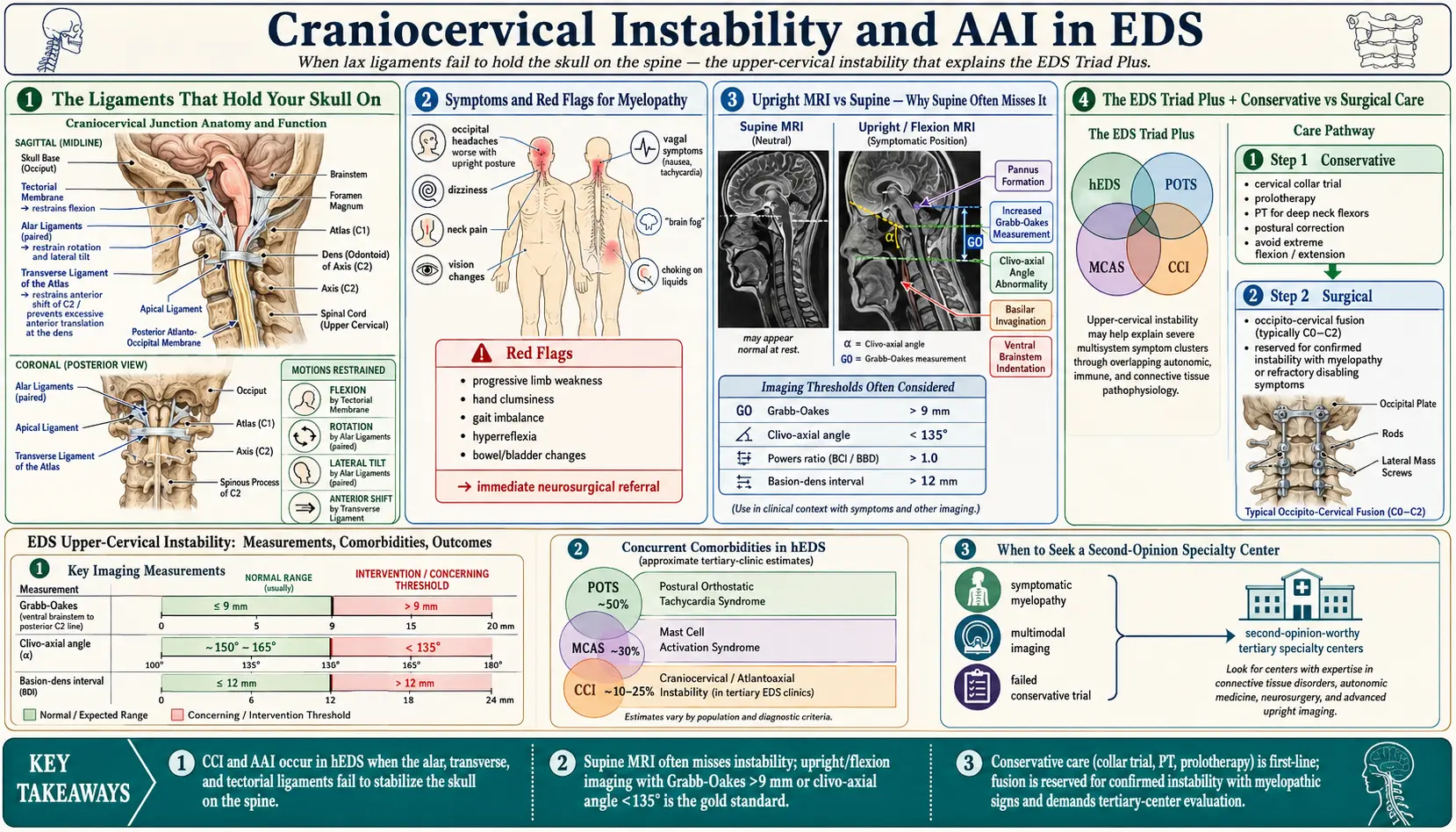
The Ligaments That Hold Your Skull On
Your head weighs ten to twelve pounds. It balances on a small ring of bone — the atlas (C1) — which in turn sits on the peg-shaped axis (C2). The connection between your skull and C1 is called the atlanto-occipital joint (C0-C1), and the connection between C1 and C2 is the atlantoaxial joint (C1-C2). Together they handle more rotation, flexion, and extension than any other part of the spine, yet they have almost no bony interlock. Stability comes almost entirely from ligaments.
Three ligaments matter most:
- Alar ligaments — paired cords running from the dens (the peg of C2) to the sides of the occiput. They limit side-bending and rotation.
- Transverse atlantal ligament — a horizontal strap that pins the dens against the front of the C1 ring, preventing the peg from sliding backward into the spinal cord.
- Tectorial membrane — a broad sheet continuous with the posterior longitudinal ligament; it covers the dens and stops the skull from dropping too far forward.
In EDS — particularly hypermobile and classical types — the collagen in these ligaments is structurally abnormal. They stretch more under load, creep over time, and fail to spring back. The result is that the skull can drift, tilt, or slide relative to C1 and C2 beyond the normal range. When that abnormal motion pinches the brainstem, the upper spinal cord, the vertebral arteries, or the lower cranial nerves, symptoms begin.
Symptoms — What CCI and AAI Feel Like
The symptom list is long because the structures packed into this tiny region do so many different jobs. Most patients do not have all of these; most have a cluster that gets worse when upright and better when lying flat.
- Occipital and upper neck pain — a heavy, pressing ache at the base of the skull, often described as "my head is too heavy for my neck." Worse late in the day, worse after reading or driving, better lying down.
- Cervicogenic headaches that start at the occiput and wrap forward behind the eyes.
- Vertigo and disequilibrium — not classic spinning, but a sense of the floor moving or of needing to grip furniture.
- Visual disturbances — blurred vision, double vision, trouble tracking moving objects, light sensitivity, pressure behind the eyes.
- Dysautonomia flares — sudden tachycardia, blood-pressure swings, temperature dysregulation, and syncope that worsen when upright (see the POTS/MCAS triad article).
- Swallowing difficulties — food catching, a choking sensation, or a feeling of something pressing on the throat from behind.
- Tingling, weakness, or heaviness in the arms or legs, sometimes worse with neck flexion (Lhermitte's phenomenon — an electric jolt down the spine when the chin drops to the chest).
- Cognitive fog — word-finding trouble, short-term memory lapses, and a feeling of running at half speed, often worse upright.
- Facial numbness, ear fullness, or tinnitus from irritation of lower cranial nerves.
- Sleep-disordered breathing and central apnea in severe cases, from brainstem compression.
A hallmark pattern is positional dependence. Symptoms ease within minutes of reclining, worsen within minutes of sitting or standing, and worsen further with head-forward posture (phone use, reading, cooking). Many patients learn to prop their chin in their hands or lean against walls without consciously realizing why.
Red Flags for Myelopathy — Act Immediately
Some signs indicate the spinal cord itself is being compressed. These require urgent neurosurgical evaluation — not next month, not "after your next rheumatology appointment," but within days. Go to an emergency department if they are new or rapidly progressing:
- Hyperreflexia — knee-jerk and biceps reflexes that snap back exaggeratedly.
- Clonus — rhythmic, involuntary beats of the foot when the ankle is dorsiflexed.
- Positive Hoffman's sign — flicking the middle fingernail causes the thumb and index finger to twitch inward.
- Positive Babinski sign — the big toe lifts upward when the sole is stroked.
- New bowel or bladder changes — urinary retention, incontinence, or loss of the urge to urinate or defecate.
- Progressive weakness, loss of fine motor control (buttoning, handwriting), or a wide-based, unsteady gait.
- New difficulty breathing, swallowing, or speaking.
These signs do not appear in isolated ligament strain or in most cases of mild instability. When they do appear, the spinal cord is telling you something mechanical is happening that it cannot tolerate. Bring a written list to the emergency department and ask specifically for a neurosurgery consult.
The EDS Triad Plus — POTS, MCAS, and CCI
Researchers describe a "terrible triad" of hypermobile EDS plus postural orthostatic tachycardia syndrome (POTS) plus mast cell activation syndrome (MCAS). Adding craniocervical instability creates a "triad plus" that accounts for some of the most disabling EDS presentations.
These conditions feed one another. Brainstem compression irritates the vagus nerve and the autonomic nuclei that regulate heart rate and blood pressure, worsening POTS. Chronic pain and mechanical stress on cervical tissue sites trigger mast cell degranulation, worsening MCAS. Mast-cell mediators then loosen connective tissue further. Many patients spend years being treated for "just POTS" or "just migraines" when a mechanical driver at the craniocervical junction is quietly making everything worse.
If standard POTS care (hydration, salt, compression, beta-blockers, midodrine, ivabradine) has plateaued — especially if tilt or upright activity produces neurological symptoms beyond tachycardia — it is reasonable to ask whether CCI belongs on the workup list.
Imaging — Why Supine MRI Often Misses CCI
Standard cervical-spine MRI is performed with the patient lying flat, neck neutral, muscles relaxed. That is exactly the position in which a lax craniocervical junction looks its best. The ligaments are unloaded, the skull is not pressing down, and the measurements can come back within normal limits even when the patient cannot function upright.
The imaging that actually shows CCI is:
- Upright (weight-bearing) MRI — performed on a specialized open magnet while the patient sits or stands. Gravity reveals displacements that disappear when supine. Available at a limited number of centers.
- Flexion-extension MRI — imaging taken with the chin tucked to the chest, then with the head tilted back. This captures how much the skull-C1-C2 complex translates and angulates under real motion.
- Dynamic (flexion-extension) CT — faster, higher bony resolution; useful when MRI is inconclusive or when rotational (AAI) instability is suspected. Involves more radiation.
- Rotational CT — head turned fully left, then fully right, looking for excessive C1-on-C2 rotation or subluxation.
If you have been told your neck MRI is "normal" but your symptoms are classic, the normal scan may simply be the wrong test. Ask specifically about upright imaging or flexion-extension views, and have them interpreted by a radiologist or neurosurgeon experienced in EDS instability measurements.
Key Measurements Your Radiologist Should Report
Getting the right scan is only half the battle. The images must be measured correctly. The following numbers are the ones that matter, and they should appear in the report by name:
- Clivo-axial angle (CXA) — the angle between a line along the lower clivus and a line along the back of the dens (C2). Normal in adults is roughly 150–165°. Below 135° is considered abnormal and correlates with brainstem kinking.
- Grabb-Oakes measurement (pB-C2) — the distance from a line connecting the basion to the posterior-inferior corner of C2, measured forward to the dura. Greater than 9 mm suggests ventral brainstem compression.
- Basion-axial interval (BAI) — the horizontal distance from the basion to a vertical line extending upward from the posterior cortex of C2. Excessive translation on flexion-extension is abnormal.
- Basion-dens interval (BDI) — the distance from the basion to the tip of the dens; increases indicate vertical instability (cranial settling).
- Horizontal Harris measurement — the horizontal distance from the basion to a line along the posterior axial cortex. Values over 12 mm suggest anterior displacement of the skull on the spine.
- Atlanto-dental interval (ADI) — the gap between the front of the dens and the back of the anterior C1 arch. Adults: over 3 mm abnormal; children: over 5 mm. A widened ADI is the core sign of AAI.
Request that the report include these specific measurements. A general statement that "the craniocervical junction appears unremarkable" without numbers does not rule out instability.
Chiari Malformation and Overlap
Some EDS patients also have a Chiari I malformation — the lower tips of the cerebellum (tonsils) descending more than 5 mm below the foramen magnum. When present together, Chiari and CCI can each amplify the other's symptoms and make decisions about decompression versus fusion more complex.
Importantly, decompressing Chiari without addressing underlying CCI can make a patient worse because removing bone at the back of the skull may further destabilize an already loose junction. This is one of several reasons surgery in this region must be planned by a team familiar with EDS biomechanics.
Conservative First-Line Care
Even when imaging confirms instability, conservative care is the first step for nearly everyone. Most patients improve meaningfully, and some improve enough that surgery is permanently off the table.
- Cervical collar, properly fitted. A soft foam collar is not enough for significant instability. A semi-rigid collar (Aspen Vista, Miami J, Philadelphia) fitted by an orthotist or an experienced PT can offload the ligaments during flare periods. Collars are used intermittently — typically during upright activity, long car rides, or symptomatic days — not 24/7, because continuous use weakens the very muscles you need.
- Manual physical therapy, with strict limits. Look for a PT familiar with EDS and upper-cervical work. The protocol emphasizes deep-neck-flexor activation (chin tucks, low-load isometrics), scapular stabilization, and postural re-education. High-velocity manipulation (chiropractic "cracking" of the neck) is contraindicated in suspected or confirmed CCI — it can cause acute neurological injury.
- Postural training. Screens at eye level. Voice-to-text instead of prolonged texting. Supportive pillows that keep the neck neutral. Avoiding chin-to-chest sleep positions.
- Vagus-nerve calming. Slow nasal breathing, humming, cold-water face exposure, and graded aerobic pacing can reduce the dysautonomic storm that rides alongside CCI symptoms.
- Comorbidity care. Treating POTS (hydration, salt, compression, medications) and MCAS (H1/H2 blockers, mast-cell stabilizers) often lowers the overall symptom burden even when the mechanical problem remains.
- Prolotherapy and PRP injections. Dextrose or platelet-rich plasma injections into cervical ligaments are offered by some clinics as a non-surgical "tightening" approach. Evidence is limited, studies are small and mostly uncontrolled, and outcomes vary widely. It is reasonable to understand this as experimental rather than proven, and to ask for published outcomes from the specific practitioner before paying out of pocket.
Surgical Fusion — An Honest Conversation
For a minority of patients — those with documented instability on dynamic imaging, red-flag neurological signs, or disabling symptoms unresponsive to prolonged conservative care — occipito-cervical fusion (C0-C2, sometimes extended to C3 or below) is offered. Titanium hardware anchors the skull to the upper cervical vertebrae, and over months the bones grow together into a single rigid block.
This surgery can be life-changing. It can also make things permanently worse. Every patient considering it should understand the following before consenting:
- It is irreversible. Once the skull is fused to C2, normal head rotation, nodding, and tilting at those joints are gone forever. Compensatory motion shifts to the levels below, which in EDS patients may themselves become unstable over time (adjacent-segment disease).
- It is controversial. Neurosurgical societies do not agree on imaging thresholds, patient selection, or long-term outcomes in hEDS. Published case series come from a small number of centers. Randomized trials do not exist.
- Hardware failure, infection, pseudoarthrosis (non-fusion), dysphagia, and persistent pain are real post-operative risks, and appear to be somewhat higher in EDS patients because the bone and soft tissue heal less robustly.
- Recovery is long. Expect three to six months in a collar, a year before return to most activities, and ongoing PT for longer.
- It treats the mechanical problem, not the underlying collagen disorder. POTS, MCAS, GI dysmotility, and pain in other joints will still be there.
Surgery should be considered only when: (1) conservative care with a collar, EDS-trained PT, and comorbidity management has genuinely failed over many months; (2) dynamic imaging documents measurable instability using the criteria above; (3) symptoms are disabling; (4) the surgical team has specific experience with hEDS patients and has discussed alternatives honestly. If any of these is missing, wait and seek another opinion.
Second Opinions and Choosing a Center
Very few centers in the United States have built deep experience with EDS-related craniocervical instability. Published series have come out of programs associated with Johns Hopkins, the Mayo Clinic, and a handful of private neurosurgical practices with EDS-focused clinics. A genuinely experienced team will:
- Order upright or flexion-extension imaging before discussing surgery.
- Report the specific measurements above and explain their thresholds.
- Insist on a trial of conservative care and document its failure.
- Work jointly with cardiology (for POTS), allergy/immunology (for MCAS), and PT before operating.
- Discuss adjacent-segment disease and long-term outcomes candidly.
- Be willing to say "you are not a surgical candidate" when that is the honest answer.
A clinic that offers surgery after a single supine MRI, that pressures you to commit on a first visit, or that does not mention conservative alternatives is a clinic to walk away from. Get at least two independent neurosurgical opinions, from programs with different institutional affiliations, before consenting. The permanence of fusion makes a few extra months of evaluation the safest thing you can do.
Pursuing a CCI diagnosis can also be psychologically difficult. Some patients feel validated when imaging finally confirms what they have been describing for years. Others find that a new diagnosis brings fresh anxiety, confusing treatment choices, and disagreement between specialists. Both reactions are normal. Having an experienced EDS physician or geneticist quarterback the workup — rather than a single neurosurgeon — helps keep surgery-versus-conservative decisions grounded in the whole clinical picture.
Key Research Papers
- Henderson FC Sr, et al. Neurological and spinal manifestations of the Ehlers-Danlos syndromes. Am J Med Genet C Semin Med Genet. 2017.
- Milhorat TH, et al. Syndrome of occipitoatlantoaxial hypermobility, cranial settling, and Chiari malformation type I in patients with hereditary disorders of connective tissue. J Neurosurg Spine. 2007.
- Klinge PM, et al. Craniocervical instability in Ehlers-Danlos syndrome: outcomes and imaging. Am J Med Genet C Semin Med Genet. 2021.
- Henderson FC Sr, et al. Cervical medullary syndrome associated with craniocervical instability and Chiari malformation: diagnosis and surgical outcomes. Am J Med Genet C Semin Med Genet. 2017.
- Castori M, Voermans NC. Neurological manifestations of Ehlers-Danlos syndrome(s): a review. 2014.
PubMed Topic Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on craniocervical instability in EDS:
- Craniocervical instability and Ehlers-Danlos syndrome
- Atlantoaxial instability and joint hypermobility
- Clivo-axial angle and connective tissue disorders
- Upright MRI of the craniocervical junction
- Chiari malformation and Ehlers-Danlos syndrome
- Occipitocervical fusion in EDS — outcomes
- POTS and craniocervical instability overlap
- Grabb-Oakes measurement and brainstem compression
- Cervical prolotherapy for ligament laxity
- Cervical myelopathy clinical signs
Connections
- Ehlers-Danlos Syndrome
- Hypermobile EDS and 2017 Diagnostic Criteria
- Classical and Vascular EDS
- GI Involvement in EDS
- POTS, MCAS and the EDS Triad
- Pain Management in hEDS
- Pediatric EDS and Transition of Care
- Physical Therapy and Joint Protection
- Pregnancy and EDS
- POTS
- MCAS
- Chronic Pain
- Collagen
- Chronic Fatigue Syndrome