Fertility and Endometriosis
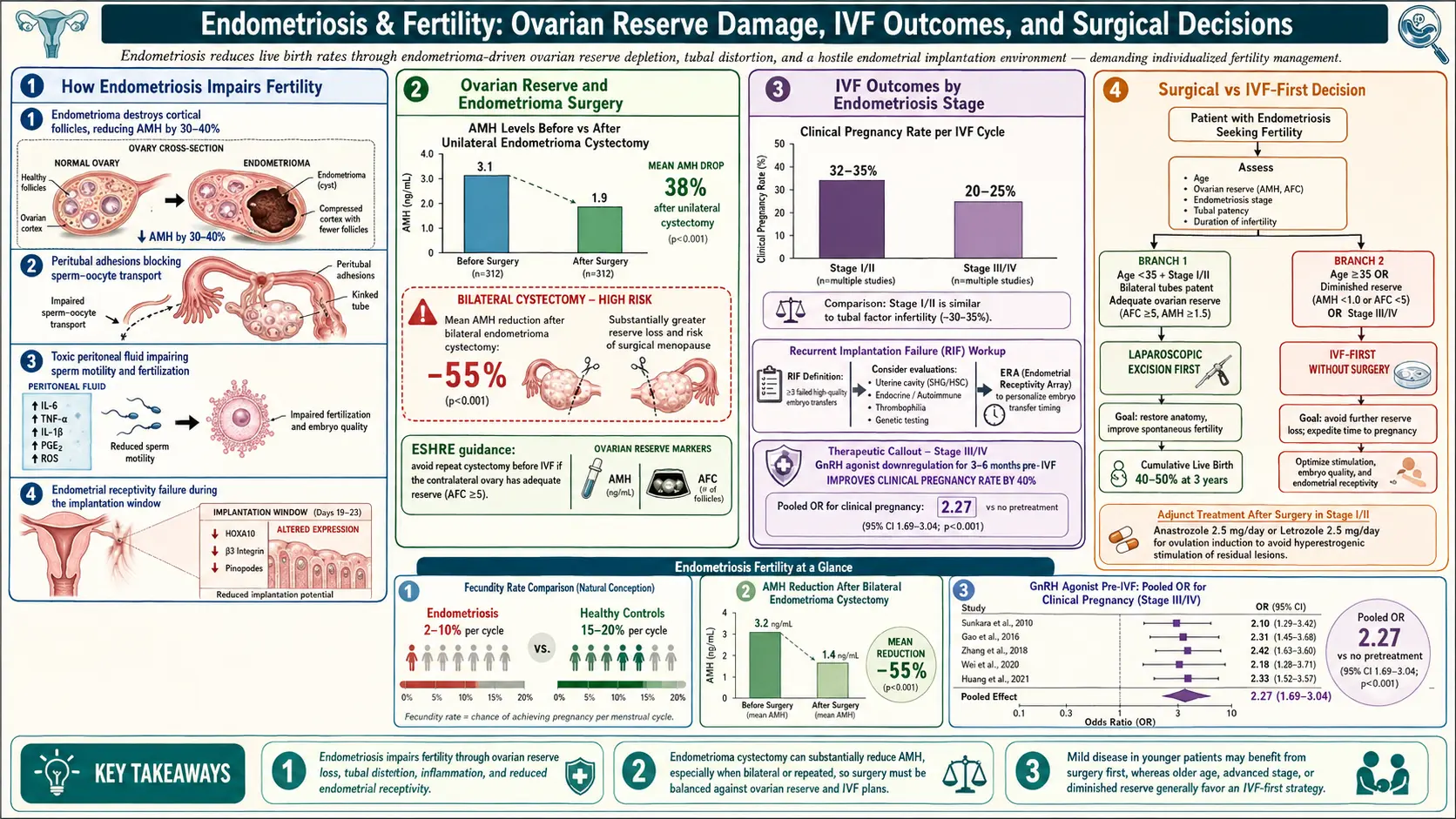
Table of Contents
- The Fertility Impact — The Real Numbers
- How Endo Gets Between You and Pregnancy
- Endometriomas and Ovarian Reserve
- ASRM Stages I–IV and Fertility
- When to See a Reproductive Endocrinologist
- The Fertility Workup
- Excision Before IVF — The Debate
- IVF Protocols for Endometriosis
- Egg Freezing — When to Consider It
- Natural Conception After Excision
- Ovarian Reserve Monitoring
- Adenomyosis and Fertility
- Pregnancy With Endometriosis
- Breastfeeding and Endo
- The Emotional Journey
- Alternative Paths to Parenthood
- Key Research Papers
- Connections
- Featured Videos
The Fertility Impact — The Real Numbers
If you have endometriosis and you are trying to conceive, the first thing to know is that your odds are not zero — but they are not the odds the fertility posters at your OB's office advertise. Somewhere between 30% and 50% of people with endometriosis experience subfertility, compared with roughly 10–15% of the general reproductive-age population. That means your chance of needing medical help to conceive is roughly three to five times higher than the friend sitting next to you who does not have this disease.
The number is a range rather than a single figure because endometriosis itself is a range. Stage I disease in someone with otherwise normal anatomy might have almost no fertility impact. Stage IV disease with frozen pelvis, bilateral endometriomas, and deep bowel involvement can effectively close the natural-conception door. The honest answer to "will I need IVF?" is usually "we don't know yet, and most of the variables are within your control only partially."
The good news buried in the statistics: most people with endometriosis who want a biological child will eventually have one, even if the route is longer, more expensive, and more emotionally punishing than they expected. What follows is a map of that route.
How Endo Gets Between You and Pregnancy
Endometriosis interferes with fertility through at least four distinct mechanisms, often layered on top of one another in the same person.
Mechanical distortion. Endometriosis lesions cause fibrotic adhesions — bands of scar tissue that glue pelvic organs together. Fallopian tubes get kinked, pulled, or sealed shut. Ovaries become tethered to the pelvic sidewall or the back of the uterus. The delicate choreography of ovulation, tubal pickup, and fertilization depends on free-floating, mobile anatomy. A pelvis with extensive adhesions simply cannot perform the mechanical work of conception, no matter how healthy the eggs and sperm are.
Inflammatory environment. Endo lesions pump out prostaglandins, cytokines (IL-1, IL-6, TNF-alpha), and reactive oxygen species that flood the peritoneal fluid. This inflammatory soup is toxic to eggs, sperm, and early embryos. Studies show reduced sperm motility in endometriotic peritoneal fluid, impaired fertilization rates even in IVF dishes, and lower egg quality retrieved from affected ovaries.
Endometrial receptivity changes. Even when an embryo reaches the uterine cavity, the uterine lining in endometriosis often does not respond normally to progesterone. Researchers call this progesterone resistance. Key implantation genes fail to switch on in the expected pattern, and the "implantation window" — the five or six days each cycle when the endometrium is receptive — narrows or shifts.
Ovarian reserve reduction. This is the mechanism most patients do not hear about until they are already in a fertility clinic. Endometriomas — ovarian cysts filled with old blood — damage the ovarian cortex around them, killing off resting follicles. Surgery on endometriomas can remove even more. The result is a smaller starting egg pool at every age.
Endometriomas and Ovarian Reserve
An endometrioma (often called a "chocolate cyst" for its dark old-blood contents) is an endometriosis lesion that has invaded an ovary and built a cyst cavity inside it. On ultrasound they have a classic ground-glass appearance. They are common — roughly 17–44% of people with endometriosis have at least one.
Endometriomas matter for fertility in two ways. First, their mere presence lowers ovarian reserve. Multiple studies show that ovaries with endometriomas have lower anti-Müllerian hormone (AMH), lower antral follicle counts (AFC), and yield fewer mature eggs per IVF retrieval compared with the contralateral unaffected ovary in the same patient. The inflammatory cyst environment appears to accelerate loss of primordial follicles.
Second, surgery on endometriomas drops reserve further. The standard excision technique — cystectomy, where the cyst wall is stripped away from the ovarian tissue — inevitably removes healthy follicles trapped in or adjacent to the cyst capsule. Post-operative AMH typically falls by 25–50% after unilateral cystectomy and even more sharply after bilateral surgery. For someone already in their late thirties or with borderline reserve, a bilateral endometrioma stripping can be fertility-ending.
This single fact drives most of the modern controversy about endometriosis management in people who want children. You cannot undo a cystectomy.
ASRM Stages I–IV and Fertility
The American Society for Reproductive Medicine staging system assigns points based on lesion depth, location, and adhesions:
- Stage I (minimal) — a few superficial implants. Spontaneous conception rates only modestly reduced. Many people conceive without intervention.
- Stage II (mild) — more implants, some shallow infiltration, minor adhesions. Cumulative two-year conception rate roughly 60–70% of normal.
- Stage III (moderate) — multiple deep implants, small endometriomas, noticeable adhesions. Spontaneous conception rate roughly half of normal.
- Stage IV (severe) — large endometriomas, dense adhesions, obliteration of the cul-de-sac, deep bowel or bladder involvement. Spontaneous conception is rare without surgical or IVF help.
A hard-earned lesson in the field: the ASRM score predicts pain and surgical complexity better than it predicts fertility. Plenty of stage I patients have unexplained subfertility. Plenty of stage IV patients conceive on the first IVF cycle once the right protocol is used. Use the stage as a rough planning tool, not a verdict.
When to See a Reproductive Endocrinologist
The standard infertility thresholds shift earlier when endometriosis is in the picture. General guidance:
- Age under 35, no known endo — see an REI after 12 months of well-timed attempts.
- Age 35–40 — see an REI after 6 months.
- Age 40 or older — see an REI after 3 months, or immediately.
- Known moderate-to-severe endo, bilateral endometriomas, or prior ovarian surgery — see an REI before you start trying, regardless of age. This is not paranoia. Your biological timeline may be shorter than the calendar suggests.
- Very low AMH for age — see an REI now, even if you are not ready to conceive, to discuss egg freezing.
An REI is a gynecologist with three additional years of fellowship training in fertility. A general OB-GYN is not the right person for this workup, no matter how kind or competent. Ask for a referral by name.
The Fertility Workup
Expect the following on your first two or three REI visits:
- AMH — blood test of ovarian reserve; can be drawn any day of the cycle.
- FSH and estradiol — drawn on cycle day 2 or 3.
- Antral follicle count (AFC) — transvaginal ultrasound counting small resting follicles in each ovary, ideally early in the cycle.
- HSG (hysterosalpingogram) — X-ray with dye to confirm tubal patency. Can be uncomfortable; ask about pre-medication.
- Saline sonohysterogram — ultrasound with saline to evaluate the uterine cavity for polyps, fibroids, or adhesions.
- Semen analysis — do not skip this. Male factor contributes to roughly 40% of fertility problems and is cheap to rule out.
- Thyroid, prolactin, hemoglobin A1c, vitamin D — correctable baseline issues.
If an endometrioma is present on ultrasound, your REI will measure it, note which ovary, and factor it into the plan — not always by removing it.
Excision Before IVF — The Debate
This is the single most-argued question in endometriosis fertility care. There is no one right answer, and anyone who tells you otherwise is selling something.
The case for excision first:
- Complete excision of all disease can restore spontaneous conception in a substantial minority of patients — roughly 40–60% conceive naturally within 12 months after expert excision of moderate-to-severe disease.
- For deep-infiltrating endometriosis (DIE) involving the bowel, bladder, or uterosacral ligaments, excision improves IVF outcomes and relieves severe pain that would make pregnancy itself miserable.
- Large endometriomas (>4 cm) can mechanically block follicle access during egg retrieval and occasionally rupture during stimulation.
- Excision addresses symptoms. IVF does not cure endo; you still have the disease after a baby.
The case against excision first:
- Ovarian surgery reduces reserve, sometimes dramatically, and the loss is permanent.
- Surgery delays conception attempts by 3–6 months (recovery plus suppression) — time that matters after 35.
- Post-surgical adhesions can make future egg retrievals harder.
- For mild-to-moderate disease without deep infiltration and without large endometriomas, IVF success rates are similar whether surgery is done first or not.
Current consensus (ESHRE 2022 and most expert excision centers): excise if there is significant pain, deep-infiltrating disease, or endometriomas larger than about 4 cm causing mechanical problems. Go directly to IVF if the disease is superficial, reserve is already low, age is pressing, or the patient has tolerable pain and wants the shortest path to a pregnancy.
Get a second opinion from a skilled excision surgeon and an REI before deciding. They often disagree, and the tension between their views is exactly the information you need.
IVF Protocols for Endometriosis
Not every IVF cycle looks the same, and endometriosis patients often need a tailored approach.
Ultra-long GnRH agonist protocol. The best-studied endo-specific protocol. The patient receives a GnRH agonist (leuprolide/Lupron) for 3 to 6 months before ovarian stimulation. This prolonged suppression shrinks active disease, calms inflammation, and allows the endometrium to reset. A landmark Cochrane review (Sallam 2006 and subsequent updates) found pregnancy rates roughly four times higher with ultra-long agonist compared with short protocols in endometriosis patients. The cost is real: three to six months of menopausal-like symptoms before you even start stims.
GnRH antagonist protocol. The shorter, modern standard. Stimulation starts on cycle day 2–3; an antagonist (cetrorelix, ganirelix) is added mid-cycle to prevent premature ovulation. Less suppression, faster, cheaper, and adequate for many endo patients — particularly those with mild disease or diminished reserve who cannot afford the time cost of a long protocol.
Letrozole-primed stimulation. For patients with low reserve or estrogen-sensitive disease, letrozole (an aromatase inhibitor) added during stim keeps estradiol levels lower, potentially reducing endo flare. Useful in oncofertility overlap and in patients who get severe pain with high estrogen.
DuoStim (double stimulation). Two egg retrievals in the same menstrual cycle — one follicular, one luteal. Built for patients with very low reserve who need to bank as many eggs or embryos as possible as quickly as possible. Endometriosis patients with rapidly declining AMH are candidates.
Frozen embryo transfer with endometrial preparation. Many clinics now separate retrieval from transfer for endo patients: retrieve embryos, freeze them, then do a medicated or natural transfer cycle later when the endometrium is calmer. Transfer outcomes in endo often improve with this approach, sometimes combined with a short course of pre-transfer GnRH agonist suppression.
Egg Freezing — When to Consider It
Egg freezing is the single most underused tool in endometriosis care. Consider it if you:
- Have known moderate or severe endometriosis and are not yet ready to conceive.
- Are facing bilateral endometrioma surgery.
- Have an AMH already lower than age-expected.
- Are approaching 35 without a partner or a clear parenthood plan.
A freezing cycle is biologically identical to the first half of an IVF cycle: stimulation, retrieval, vitrification of mature oocytes. U.S. costs typically run $12,000–$20,000 per cycle plus $500–$1,000 per year of storage. Some employers now cover it. Frozen eggs have no expiration date, and survival thaw rates at modern labs exceed 90%.
Natural Conception After Excision
For patients with moderate-to-severe disease, complete excision by a high-volume surgeon restores spontaneous conception in a meaningful share of cases: roughly 40–60% conceive within 12 months of full excision, with the highest rates in younger patients with normal reserve. Outcomes drop sharply after age 38 and after repeat surgery.
The practical implication: if excision is planned and you want a biological child, the 6–12 month window after surgery is your best spontaneous-conception window. Disease recurs over time; so does adhesion formation. Most excision surgeons advise not delaying attempts.
Ovarian Reserve Monitoring
If you have endometriosis and want to keep your options open, ask for serial AMH testing every 6–12 months. AMH trajectories matter as much as the absolute number. A sharp drop — even from a "normal" value into the lower-normal range — is a signal to accelerate plans.
Before any planned ovarian surgery, document AMH, AFC, and discuss fertility preservation explicitly with the surgeon. "I may want to freeze eggs before this cystectomy" is a legitimate request and should pause the surgical calendar, not the conversation.
Adenomyosis and Fertility
Adenomyosis — endometrial tissue within the uterine muscle — commonly coexists with endometriosis and has its own independent fertility impact. It reduces implantation rates, increases miscarriage risk, and is associated with worse IVF outcomes. The same ultra-long GnRH agonist suppression that helps endo also helps adenomyosis before IVF transfer, with several studies showing implantation rates climbing by 10–15 percentage points after 2–3 months of pre-transfer suppression.
If your MRI or ultrasound shows adenomyosis features — diffuse myometrial thickening, junctional zone changes, cystic spaces — make sure your REI is planning for it, not just the endo.
Pregnancy With Endometriosis
One persistent myth deserves a direct contradiction: pregnancy does not cure endometriosis. Many patients experience a temporary reprieve from pain during the pregnancy itself (thanks to the high, steady progesterone state), but the disease returns — often within a few months of delivery or after breastfeeding ends.
Pregnancy with endo also carries real obstetric risks:
- Miscarriage — modest but consistent increase in first-trimester loss.
- Preterm birth — roughly 1.5–2 times the baseline risk.
- Placenta previa — roughly 2–4 times the baseline risk, likely from altered uterine vasculature.
- Pre-eclampsia and small-for-gestational-age babies — small but real increase.
- Rare but serious: spontaneous hemoperitoneum of pregnancy from a bleeding endometriotic vessel.
Most of these risks are managed by co-management with a maternal-fetal medicine specialist. Your obstetrician should know about your endometriosis history in the first prenatal visit.
Breastfeeding and Endo
Exclusive breastfeeding often suppresses ovulation for months, and the associated lactational amenorrhea is frequently a pain-free window for endo patients. Many patients describe the postpartum breastfeeding phase as the most comfortable stretch they have had since menarche.
When menstrual cycles resume, symptoms typically resume with them. This is not a failure of breastfeeding or a sign that something new has happened — it is the disease coming back online with your hormones. Plan for it rather than being ambushed by it.
The Emotional Journey
No amount of protocol detail captures what it feels like to try to build a family against this disease. Month after month of negative tests. Procedures scheduled around work. Injections in a car before a meeting. Marriages that strain and sometimes crack. Friendships that quietly thin because you cannot stand another baby shower. Financial decisions that would look insane on paper if you were not desperate.
Grief belongs here. The grief of a body that will not cooperate. The grief of a timeline rewritten without your consent. The grief, often, of watching someone younger and healthier conceive on the first try while your third IVF fails. These feelings are not weakness; they are the appropriate response to accumulated loss.
Practical supports that help: a therapist who specializes in reproductive grief, a peer group (Resolve, local endo groups, online communities), honest conversations with your partner about what you can and cannot sustain, and written limits — how many cycles, how much money, how long — agreed on in calm moments and revisited before each decision. Guardrails protect you from the sunk-cost spiral that fertility treatment can become.
Alternative Paths to Parenthood
IVF is not the only path, and it is not always the right one. All of the following are legitimate, full forms of parenthood:
- Donor eggs. If ovarian reserve is very low or multiple IVF cycles have failed, a younger donor's eggs with your partner's (or donor) sperm and carried in your own uterus yields some of the highest pregnancy rates in reproductive medicine. Many patients initially resist the idea and, after time, find the genetic-versus-gestational distinction matters less than they expected.
- Gestational carrier (surrogate). If the uterus cannot safely carry a pregnancy — severe adenomyosis, repeat loss, extensive uterine scarring, or medical contraindications — a gestational carrier using your embryo is an option. Legally and financially complex; work with a fertility-experienced attorney.
- Embryo donation and adoption (domestic, foster, international) — each with their own timelines, costs, and emotional textures.
- Child-free by choice or by acceptance. Some people arrive, after much grief, at a life that is not built around a child. That life can be full. The cultural script that insists otherwise is wrong.
Whichever road you take, it is yours. Endometriosis may narrow the options, but it does not get to choose for you.
Key Research Papers
- Sallam HN, et al. Long-term pituitary down-regulation before in vitro fertilization (IVF) for women with endometriosis. Cochrane Database Syst Rev. 2006.
- Somigliana E, et al. Surgical excision of endometriomas and ovarian reserve: a systematic review on serum antimüllerian hormone level modifications. Fertil Steril / Hum Reprod Update. 2012.
- Vercellini P, et al. Endometriosis: pathogenesis and treatment — surgery and ART for endometriosis-associated infertility. Nat Rev Endocrinol. 2014.
- ESHRE Endometriosis Guideline Development Group. ESHRE guideline: endometriosis. Hum Reprod Open. 2022.
Live PubMed Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on endometriosis and fertility:
- Endometriosis and IVF outcomes
- Ultra-long GnRH agonist protocol in endometriosis IVF
- Endometrioma and ovarian reserve (AMH)
- Endometrioma cystectomy and fertility outcomes
- Deep-infiltrating endometriosis and fertility
- Adenomyosis and IVF outcomes
- Endometriosis and pregnancy complications
- Endometriosis, progesterone resistance, and implantation
Connections
- Endometriosis
- Infertility
- Ovarian Cysts
- Laparoscopy: Excision vs Ablation
- Diagnosis Delay and Imaging
- Hormonal Therapy Options
- Pelvic Floor Therapy and Central Sensitization
- Endo Belly and Gut Connection
- Diet and Lifestyle
- Adenomyosis Overlap
- Bladder and Bowel Endometriosis
- Polycystic Ovary Syndrome
- Perimenopause
- Uterine Fibroids
- Menopause and HRT
- Magnesium
- Vitamin D3
- Ultra Processed Foods