Laparoscopy: Excision vs. Ablation for Endometriosis
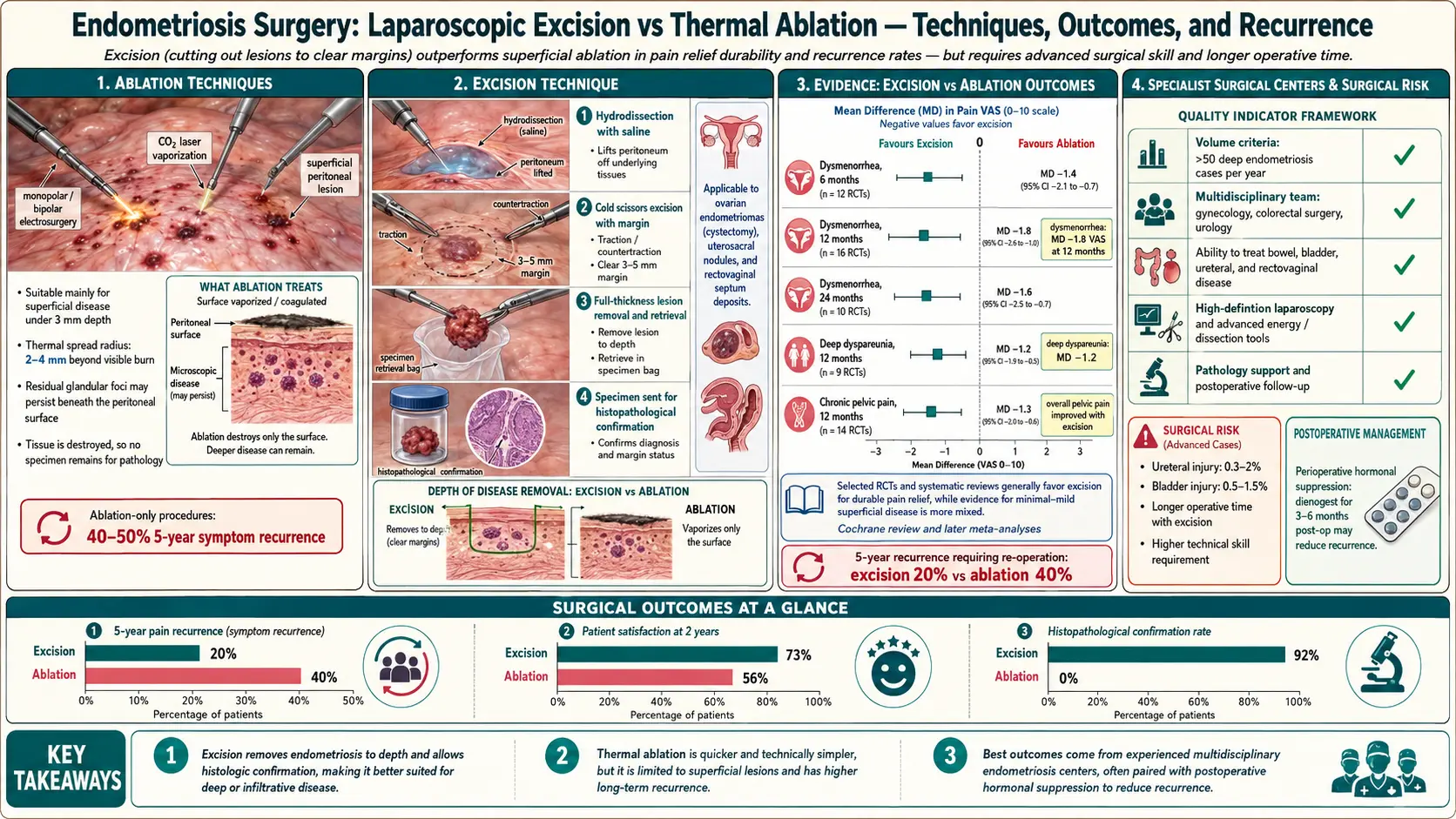
Table of Contents
- The Distinction — Excision vs. Ablation
- Why the Difference Matters
- The Evidence
- Recurrence Rates
- The “Generalist Gyn” Problem
- Finding an Excision Surgeon
- The “See and Treat” Approach
- Surgical Approach — Laparoscopy, Robotic, Multi-Disciplinary
- Pre-Op Preparation
- What Happens in Surgery
- Recovery
- After Excision — Pain, Suppression, Expectations
- When Recurrence Happens
- Hysterectomy — When It Is Actually Indicated
- Risks of Excision
- Costs and Insurance
- Key Research Papers
- Connections
- Featured Videos
The Distinction — Excision vs. Ablation
Two operations share the name “laparoscopy for endometriosis,” and they are not the same surgery. Understanding the difference is the single most important decision you will make about your treatment.
Excision — sometimes called LAPEX (laparoscopic excision), wide excision, or deep excision — means the surgeon cuts the endometriosis lesion out. Using scissors, a CO2 laser in cutting mode, a harmonic scalpel, or a plasma-energy device, the surgeon traces around the lesion, slices beneath it, and removes the diseased tissue along with a margin of normal-looking tissue underneath. The specimen is placed in a bag and sent to pathology for confirmation. What is left behind is a clean defect in the peritoneum or organ surface, which is usually left to heal by secondary intention.
Ablation — also called fulguration, coagulation, or vaporization — means the surgeon destroys the surface of the lesion with heat. The tools are monopolar or bipolar cautery, argon beam, laser in vaporization mode, or a helium plasma device. The visible dark spot turns white, brown, or charred. Nothing is removed; nothing is sent to pathology. The surgery is faster, technically easier, and carries a lower intra-operative risk profile — which is exactly why it is still the most common procedure performed for endometriosis in the United States.
Both operations are done through the same 5–12 mm trocar ports. From the outside you cannot tell which one you received. From the inside, the distinction decides whether your disease is actually gone or just painted over.
Why the Difference Matters
Endometriosis is not a skin disease. Lesions extend below the visible surface. Pathology studies that serially section excised specimens find endometrial glands and stroma reaching 2 to 5 millimeters below what the eye sees on the peritoneum, and more than a centimeter deep in classic deep-infiltrating endometriosis (DIE) of the cul-de-sac, uterosacral ligaments, bowel, or bladder.
Ablation energy penetrates a tiny fraction of that. Superficial cautery destroys roughly 0.5 to 1 millimeter of tissue; even aggressive vaporization reaches 2–3 millimeters at best, and doing so on a bowel serosa or ureter invites injury. Burning the top of a deep lesion leaves the bulk of the disease alive underneath, where it continues to bleed, scar, and produce inflammatory cytokines each cycle. The visible “powder-burn” marking vanishes. The pain does not.
This is the mechanical reason so many women report that a laparoscopy “helped for a few months and then the pain came back worse.” The disease never left. It regrew from a base that was never removed.
The Evidence
The evidence base for excision over ablation has been building for two decades. The key landmarks:
Healey 2010 RCT. Melbourne-based surgeon Martin Healey randomized 178 women with stage II–IV endometriosis to laparoscopic excision or ablation. At 12 months, pain scores improved in both groups, but at five-year follow-up excision produced significantly better relief of dysmenorrhea, dyspareunia, and dyschezia. This remains the most-cited head-to-head trial.
Pundir / Wright updates. A 2017 Cochrane-style meta-analysis of excision versus ablation confirmed superiority of excision for deep-infiltrating disease, with weaker differences for peritoneal-only stage I disease.
Yeung systematic reviews. St. Louis excision specialist Patrick Yeung published systematic reviews in 2014 and a broader update arguing that excision by an expert can achieve long-term recurrence rates under 20%, compared with 40–60% historically reported for mixed or ablation-based cohorts.
AAGL 2021 Practice Guideline. The American Association of Gynecologic Laparoscopists published a formal guideline on endometriosis recommending excision as the preferred surgical approach for deep-infiltrating endometriosis, with ablation considered acceptable only for isolated superficial peritoneal disease by experienced surgeons.
ESHRE 2022 Guideline. The European Society of Human Reproduction and Embryology updated its endometriosis guideline to explicitly prefer excision for deep disease, reduce reflex use of post-operative GnRH agonists, and emphasize multidisciplinary centers for complex cases.
The direction of every major guideline over the past decade has been the same: toward excision, toward expert centers, and away from repeat diagnostic laparoscopies that treat nothing.
Recurrence Rates
Recurrence is the honest metric. It is also the one generalist practices do not quote you pre-operatively.
- Ablation, generalist surgeon: roughly 20% symptomatic recurrence within the first year and 40–50% within five years. Repeat surgery rates in large cohorts reach 30–60% at ten years.
- Excision, high-volume specialist: published long-term series report under 20% recurrence at five to seven years, and about half of those recurrences are de novo disease in new locations rather than true regrowth of incompletely excised lesions.
- Excision, low-volume generalist: intermediate outcomes that blur into the ablation numbers. “Excision” on the op note does not guarantee an expert technique.
The surgeon’s experience predicts the result far more than the brand of the instrument in their hand.
The “Generalist Gyn” Problem
Most obstetrician-gynecologists finish residency comfortable with hysterectomy, tubal ligation, ovarian cystectomy, and superficial ablation of visible endometriosis spots. They have not been trained to dissect a ureter free of fibrotic endo, shave an implant off the rectal serosa, or resect a segment of bladder. Those skills require a post-residency minimally invasive gynecologic surgery (MIGS) fellowship or years of high-volume endometriosis practice.
That training gap is the real reason ablation is still so common. A generalist faced with stage III or IV disease at the time of surgery has three options: abort and refer, do a superficial burn and close, or attempt a dissection beyond their comfort level. Many choose option two. The operative report reads “endometriosis identified and ablated.” The patient wakes up told the surgery was a success. The disease sits intact underneath the char.
This is not an accusation of bad faith. It is the predictable result of a specialty where true endometriosis surgeons are rare and referral networks are weak. The burden of finding the right surgeon falls on the patient.
Finding an Excision Surgeon
There are a small number of reliable ways to identify surgeons whose practice is dedicated to endometriosis excision:
- Nancy’s Nook Endometriosis Education (a large private Facebook group) maintains a vetted list of excision surgeons worldwide. Inclusion requires submitting operative reports and patient outcome data for review. The list is the single most-used patient-community resource in the United States.
- iCareBetter.com is a surgeon-directory platform that requires blind video review of excision surgeries by other specialists before listing. It is newer and smaller than the Nook list but overlaps heavily.
- AAGL Fellowship directory. The AAGL (aagl.org) maintains a list of MIGS fellowship graduates. Not all MIGS fellows specialize in endometriosis, but the baseline training is appropriate.
- Academic endometriosis centers. Institutions such as the Center for Endometriosis Care (Atlanta), Seckin Endometriosis Center (NYC), UCSF, Mayo, and the Cleveland Clinic run high-volume excision programs with multidisciplinary teams.
The single best screening question you can ask a prospective surgeon at a consult is: “What percentage of your surgical practice is endometriosis excision?” You want a number above 75%. A general gynecologist who does four endo cases a year among hundreds of hysterectomies is not who you want operating on your ureter. Follow-up questions worth asking: How many excisions do you perform per year? (Target: 100+.) Do you send excised tissue to pathology? (Yes is mandatory.) Do you work with a colorectal surgeon and urologist in the same OR when needed? (Yes for suspected deep disease.) What is your conversion-to-laparotomy rate? (Low single digits.)
The “See and Treat” Approach
Historically, women were sent for a “diagnostic laparoscopy” — the surgeon peeked, confirmed endometriosis, took a biopsy, and closed. The treatment was scheduled as a separate surgery months later. This is now considered obsolete and harmful. Every laparoscopy carries anesthesia and surgical risk; doing two when one would suffice doubles that risk for no benefit.
The modern standard is see and treat: the pre-operative consent authorizes the surgeon to excise any endometriosis found during the same procedure. If you are consenting only to diagnosis, you are consenting to the wrong operation. Insist on combined diagnosis-and-treatment consent, and confirm in writing that the surgeon is prepared to excise (not ablate) whatever they find, up to and including bowel shaving, ureterolysis, and disc resection if the team is qualified.
Surgical Approach — Laparoscopy, Robotic, Multi-Disciplinary
Standard laparoscopy uses three to five small incisions: a 10–12 mm umbilical port for the camera and 5 mm working ports in the lower abdomen. It is the default for nearly all endometriosis surgery. Pain, recovery time, and cosmetic outcome are all better than open surgery (laparotomy), and exposure of the pelvis is arguably superior because of the magnified camera view.
Robotic laparoscopy (da Vinci system) is marketed aggressively but is not inherently better for endometriosis. It offers the surgeon wristed instruments and 3D vision, which some find helpful for fine suturing, but it also removes tactile feedback and costs more per case. Outcomes in head-to-head series are similar to standard laparoscopy in experienced hands. Pick the surgeon, not the robot.
Laparotomy (a single larger incision) is now reserved for rare catastrophic cases — massive frozen pelvis, hemorrhage, or extensive bowel involvement where minimally invasive dissection is unsafe. A surgeon who defaults to laparotomy for routine endometriosis is behind the standard of care.
Multi-disciplinary teams are the differentiator at expert centers. Deep disease frequently involves the bowel, bladder, or ureter, and a gynecologist operating solo is not the right person to resect a segment of rectum or reimplant a ureter. High-volume endo programs schedule a colorectal surgeon on standby for bowel involvement and a urologist for bladder or ureteric disease. Asking whether this is arranged pre-operatively is a legitimate and expected question.
Pre-Op Preparation
Pre-operative instructions vary by surgeon, but most include some combination of:
- Mechanical bowel prep (polyethylene glycol solution or similar the day before surgery) when bowel involvement is suspected on imaging or symptoms. An empty bowel is easier to mobilize and reduces contamination if a resection becomes necessary.
- Clear-liquid diet the day before; nothing by mouth after midnight.
- Stop NSAIDs (ibuprofen, naproxen, aspirin) 5–7 days pre-op to reduce bleeding risk. Acetaminophen is allowed.
- Stop anticoagulants on the schedule agreed with the prescribing physician — warfarin, DOACs (apixaban, rivaroxaban), and P2Y12 inhibitors all have specific hold intervals.
- Hormonal pre-treatment is controversial. Some surgeons prescribe a short course of GnRH agonist or continuous progestin pre-op to quiet the disease; others argue this shrinks lesions just enough to make them harder to see and excise completely. Evidence favors not pre-treating when you have an expert excision surgeon; ask them their preference and their reasoning.
- Shower with chlorhexidine the night before and the morning of surgery to reduce skin flora.
What Happens in Surgery
Under general anesthesia, a Foley catheter is placed to keep the bladder empty. The umbilical trocar goes in first, the abdomen is insufflated with CO2, and a 5 or 10 mm camera is introduced. Additional 5 mm working ports are placed in the lower abdomen under direct vision.
The surgeon performs a systematic survey of the peritoneum: anterior and posterior cul-de-sac, uterosacral ligaments, broad ligament, ovarian fossae, bladder dome, appendix, cecum, sigmoid, diaphragm, and upper abdomen. Lesions are mapped and photographed. Ovarian endometriomas are drained and the cyst wall stripped. Deep lesions are dissected out with scissors or laser, with meticulous hemostasis. The ureter is identified and traced along its pelvic course wherever dissection approaches it. Any bowel or bladder disease is handled by the appropriate specialist.
Coexisting fibroids, ovarian cysts, or adhesions are addressed in the same operation when safe. Excised tissue is extracted through the umbilical port in a specimen bag and sent to pathology. Copious irrigation, a final hemostasis check, port closure, and the patient goes to recovery.
Recovery
For straightforward excision without bowel resection, most patients are discharged the same day or after one overnight stay. Bowel-resection cases usually stay two to four nights.
- Days 1–3: shoulder-tip pain from residual CO2 gas, abdominal soreness, sometimes nausea. Walking short distances starts immediately.
- Week 1: fatigue dominates. Most people off work. Bowel function returning.
- Weeks 2–3: most return to desk-based work. Driving resumes once off narcotics and able to brake hard without guarding.
- Weeks 4–6: lifting and vigorous exercise resume gradually. Pelvic rest (no tampons, no penetrative intercourse) is standard for 4–6 weeks.
- Week 6: post-op visit, review of pathology, discussion of next steps.
Warning signs that need urgent call-back: fever over 101°F, worsening abdominal pain after day 3, unrelenting nausea and vomiting, inability to urinate, or rectal bleeding. Ureteric or bowel injuries sometimes declare themselves 3–7 days post-op and require prompt recognition.
After Excision — Pain, Suppression, Expectations
Most women who have true wide excision by an expert surgeon report significant and durable pain improvement, often dramatic. Published patient-reported outcomes show 60–80% reporting much better pain at one to two years. Dyspareunia, dyschezia, and cyclic pain all respond.
A minority do not get the relief they expected, and this is important to understand before surgery so you are not devastated after. Reasons include:
- Coexisting adenomyosis (see the Adenomyosis Overlap article) — excision of external endometriosis does nothing for disease inside the uterine wall.
- Pelvic floor dysfunction and central sensitization — the nervous system has been in a pain loop for years and the pain pattern persists after the peripheral disease is gone. This is the major reason some patients feel let down post-op. See the Pelvic Floor & Central Sensitization article.
- Incomplete excision — the surgeon was not expert enough, or disease was microscopic and missed.
- Irritable bowel or interstitial cystitis overlap, which share the same pelvic-nerve distribution.
Whether to continue hormonal suppression after a complete excision is debated. Purist excisionists argue that if the surgery was truly complete, no medical suppression is needed and none should be pushed. Others prescribe continuous combined hormonal contraception or progestins to reduce the chance of de novo disease. A reasonable compromise: monitor symptoms for three to six months post-op, and add suppression only if pain recurs or imaging shows new lesions.
When Recurrence Happens
Persistent or recurrent pain after excision demands a careful re-evaluation rather than a reflex second surgery. Steps in order:
- Review the prior operative report and pathology. Was it truly excision or was ablation done under the label “excision”?
- Assess pelvic floor, adenomyosis, bladder, and bowel as alternative pain drivers.
- Consider medical management escalation — GnRH antagonists (elagolix, relugolix), progestins, or continuous combined hormonal contraception.
- If imaging or symptoms point to a clear surgical target, a second excision by a high-volume specialist is reasonable. Outcomes in expert second-look surgery are generally good.
What is rarely reasonable is a third or fourth ablation by a generalist. Each repeat surgery adds adhesions without treating the underlying disease.
Hysterectomy — When It Is Actually Indicated
Hysterectomy is widely and incorrectly sold as a “cure” for endometriosis. It is not. Endometriosis is, by definition, tissue that grows outside the uterus — removing the uterus does not remove the disease. Women who have had hysterectomies without proper excision routinely continue to have pain, sometimes worse.
Hysterectomy is appropriately indicated when:
- There is coexisting adenomyosis causing severe dysmenorrhea and menorrhagia that has failed other treatment. Hysterectomy is definitive for adenomyosis.
- The patient has completed childbearing and has fibroids, abnormal bleeding, or other uterine pathology in addition to endometriosis.
- Cervical or uterine pathology in its own right warrants removal.
Even then, a hysterectomy for endometriosis should be combined with thorough excision of all extrauterine disease. Ovaries should usually be preserved in women under 50 unless they are diseased themselves; bilateral oophorectomy drops endogenous estrogen to menopausal levels and brings its own long-term bone, cardiovascular, and cognitive consequences. Ovary-sparing hysterectomy plus excision is the modern standard for women in whom hysterectomy is appropriate.
Risks of Excision
All abdominal surgery carries risk, and endometriosis excision in particular dissects near structures that are expensive to injure. Honest risks:
- Bowel injury — serosal tear, enterotomy, or delayed perforation. Roughly 1–2% in high-volume centers, higher in low-volume practices.
- Ureteric injury — transection, thermal damage, or stricture. Under 1% in expert hands; higher when disease is dense on the pelvic sidewall.
- Bladder injury — cystotomy, usually recognized and repaired intra-operatively.
- Bleeding requiring transfusion — uncommon but not rare in extensive dissection.
- Adhesion formation — probably lower with excision than with cautery because the raw surfaces are clean, but adhesions still occur.
- Persistent pain — not truly a surgical complication, but the most emotionally difficult outcome when it happens.
- Anesthesia risks — standard and low in healthy patients.
All of these rates are lower — often several-fold lower — when the operating surgeon does hundreds of these cases a year. Volume is protective.
Costs and Insurance
Here is where the system breaks down. Excision specialists have long exit ramps from insurance networks because reimbursement for a complex 6-hour excision is often set by insurers at the same rate as a 45-minute ablation. Going out-of-network is a rational business response but leaves patients paying significant out-of-pocket costs — often $15,000 to $40,000 for surgeon fees alone, with facility and anesthesia billed separately and often in-network.
Practical strategies:
- Request a single-case agreement (SCA) from your insurer. If you can document that no in-network surgeon in your area is qualified to excise deep endometriosis, many insurers will agree to pay the out-of-network surgeon at in-network rates. The surgeon’s billing office usually has templates and experience with this process.
- Get a superbill and submit for out-of-network reimbursement. Even when not paid in full, this applies to your out-of-network deductible and maximum.
- Use HSA/FSA funds for eligible expenses. Surgery and anesthesia are qualifying expenses.
- Financing: Care Credit and similar medical-financing products offer deferred-interest plans. Read the terms carefully — if you miss the deferred period, interest is often retroactive to day one.
- Payment plans: most specialty practices will structure 12–24-month direct payment plans for self-pay patients.
- Compare facility fees: the same surgeon operating at an ambulatory surgery center rather than a hospital can save 30–50% on facility charges.
None of this should be normalized. It is unjust that appropriate surgical care for a disease affecting roughly one in ten women is priced out of reach for most families. Patient-advocacy groups (EndoFound, Endometriosis Association) continue to push for parity coverage. In the meantime, knowing the tactics above is the difference between getting the right surgery and settling for the wrong one.
Key Research Papers
- Healey M, Ang WC, Cheng C. Surgical treatment of endometriosis: a prospective randomized double-blinded trial comparing excision and ablation. Fertil Steril. 2010;94(7):2536–2540.
- Yeung P Jr. The laparoscopic management of endometriosis in patients with pelvic pain. J Minim Invasive Gynecol. 2014.
- AAGL Practice Committee. AAGL Practice Report: Practice Guidelines for the Diagnosis and Management of Endometriosis. J Minim Invasive Gynecol. 2021.
- Becker CM, Bokor A, Heikinheimo O, et al. ESHRE guideline: endometriosis. Hum Reprod Open. 2022;2022(2):hoac009.
Live PubMed Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on surgical management of endometriosis:
- Excision versus ablation for endometriosis
- Laparoscopic excision of deep infiltrating endometriosis
- Endometriosis recurrence after excision
- Bowel endometriosis and colorectal surgery
- Ureteral endometriosis and laparoscopic management
- Robotic versus conventional laparoscopy for endometriosis
- Hysterectomy outcomes in endometriosis
- Surgeon volume and outcomes in endometriosis surgery
Connections
- Adenomyosis Overlap
- Pelvic Floor Therapy and Central Sensitization
- Endometriosis
- Diagnosis Delay and Imaging
- Hormonal Therapy Options
- Endo Belly and Gut Connection
- Fertility and Endometriosis
- Diet and Lifestyle
- Bladder and Bowel Endometriosis
- Infertility
- Uterine Fibroids
- Chronic Pain
- Ovarian Cysts
- Interstitial Cystitis
- Full Body MRI
- Polycystic Ovary Syndrome
- Vitamin D3
- Magnesium