Diet and Lifestyle Approaches for Endometriosis
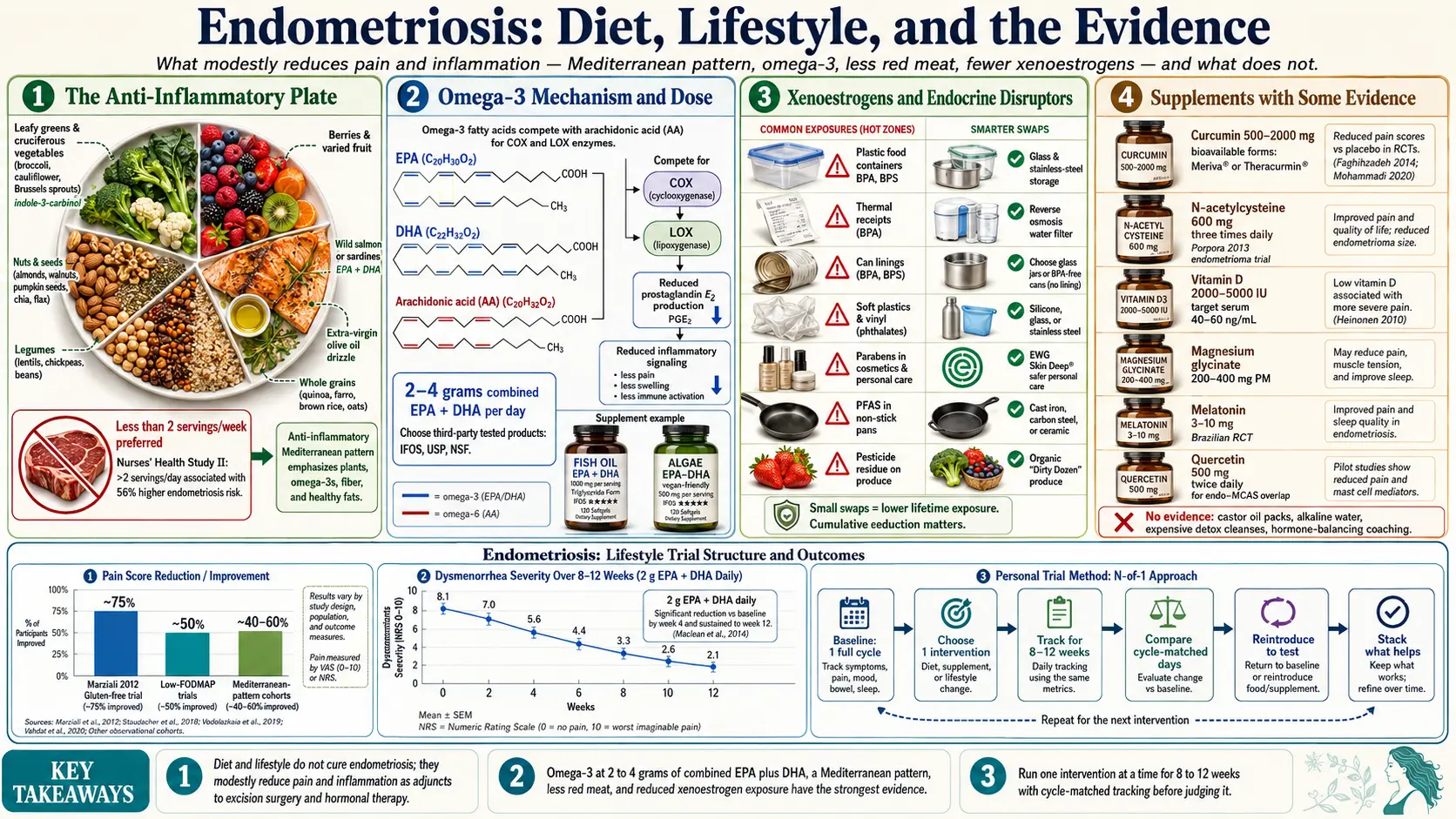
Table of Contents
- What Diet and Lifestyle Can — and Can't — Do
- The Anti-Inflammatory / Mediterranean Framework
- Omega-3 Fatty Acids
- Red Meat and Inflammation
- Dairy
- Gluten
- Xenoestrogens and Endocrine Disruptors
- Alcohol
- Caffeine
- Supplements with Some Evidence
- Exercise
- Yoga and Mind-Body Work
- Sleep
- Stress Reduction
- Environmental Exposures
- What Doesn't Have Evidence
- How to Structure a Personal Lifestyle Trial
- Key Research Papers
- Connections
- Featured Videos
What Diet and Lifestyle Can — and Can't — Do
Start here, because the internet is loud and mostly wrong. Diet and lifestyle changes do not cure endometriosis. They do not dissolve adhesions, shrink deep infiltrating lesions on the bowel or ureter, or remove the need for excision surgery and hormonal therapy in patients who need them. Anyone selling you a protocol that promises to reverse endo is selling you hope, not medicine.
What the evidence actually supports is narrower but worthwhile: in some patients, specific changes modestly reduce pain, dysmenorrhea intensity, and systemic inflammation. They improve general health outcomes that matter across a lifelong condition, and they give you a sense of agency. Think of diet and lifestyle as adjuncts sitting alongside excision surgery, appropriate hormonal suppression, pelvic-floor therapy, and pain management — not replacements.
Plan to trial any intervention for 3 to 12 months before judging it. Endo symptoms fluctuate across cycles; a single good or bad month tells you almost nothing. Track daily pain on a 0–10 scale with cycle phase so you have data, not vibes.
The Anti-Inflammatory / Mediterranean Framework
If you do only one thing, do this. The Mediterranean pattern has the deepest evidence base of any diet studied in endometriosis and inflammatory conditions generally. Core emphases:
- Vegetables — 5+ servings daily, varied colors, with leafy greens featured. Cruciferous vegetables (broccoli, cauliflower, cabbage, Brussels sprouts) contribute indole-3-carbinol and sulforaphane, which support estrogen metabolism.
- Fruit — 2–3 servings daily, berries emphasized for polyphenol density.
- Extra-virgin olive oil as the primary fat, 2–4 tablespoons daily.
- Fatty fish (wild salmon, sardines, mackerel, herring) 2–3 times weekly for EPA and DHA.
- Nuts and seeds — a small handful daily (walnuts, almonds, flax, chia).
- Legumes — lentils, chickpeas, beans several times per week.
- Whole grains if tolerated (oats, quinoa, brown rice, farro).
- Limited red meat, processed meat, refined sugar, and ultra-processed packaged foods.
In cohort studies, women eating closest to this pattern report lower dysmenorrhea scores and lower CRP. Give it 3–12 months. The benefit is cumulative and boring, the way cardiovascular benefit is.
Omega-3 Fatty Acids
Omega-3s are the single most evidence-backed nutrient intervention in painful periods. Marine-sourced EPA and DHA compete with arachidonic acid for the enzymes that produce inflammatory prostaglandins — the same prostaglandins that drive the cramping of dysmenorrhea and the pelvic inflammation of endo.
Practical dosing: 2–4 grams of combined EPA+DHA per day. Read the label carefully — a "1,000 mg fish oil" capsule may contain only 300 mg of actual EPA+DHA. Look for a third-party-tested brand (IFOS, USP, NSF) to minimize oxidation and heavy-metal concerns.
Key trials: Harel et al. 1996 showed fish oil at 1,080 mg EPA + 720 mg DHA daily reduced dysmenorrhea in adolescents. Rahbar et al. 2012 found omega-3 supplementation significantly reduced primary dysmenorrhea severity versus placebo. Multiple subsequent trials have replicated the pain-reduction signal.
If you are vegan or strictly vegetarian, an algae-based EPA/DHA supplement gives you the same end product without fish. Flax, chia, and walnuts provide ALA, which the body converts to EPA/DHA only at about 5–10% efficiency — fine as dietary background but not sufficient as your only omega-3 source if you want a therapeutic dose. Give it 8–12 weeks. If you take anticoagulants, tell your prescriber.
Red Meat and Inflammation
The best prospective data on food and endo risk comes from the Nurses' Health Study II. Analyzing over 81,000 women followed for 22 years, Yamamoto and colleagues (Harris group) found that women eating more than 2 servings of red meat per day had roughly a 56% higher risk of laparoscopically confirmed endometriosis compared to those eating one serving or less per week (Hum Reprod 2018).
Why? Three plausible mechanisms, none definitively proven but all biologically reasonable:
- Arachidonic acid — concentrated in red and processed meat, this omega-6 fatty acid feeds the same prostaglandin pathways that omega-3s dampen.
- Heme iron — abundant in red meat, heme iron is pro-oxidant and may contribute to oxidative stress in peritoneal fluid, which is already iron-heavy in endo patients from retrograde menstruation.
- IGF-1 and insulin response — higher red-meat diets raise IGF-1, a hormone that may promote proliferation of endometrial-like tissue.
Reasonable target: 1–2 small servings of red meat per week, or less, substituting fish, poultry, legumes, and eggs for the remainder. You don't have to go vegetarian. The data show a dose-response, not an all-or-nothing.
Dairy
Dairy is the most over-prescribed elimination in the endo patient community, and the evidence is genuinely mixed. Some cohort studies show a modest protective association between dairy and endo (higher calcium and vitamin D intake), while others show the opposite or nothing.
Separately, there is the A1 vs A2 casein hypothesis: most Western cow milk contains a mix of A1 and A2 beta-casein variants, and A1 digestion releases beta-casomorphin-7 (BCM-7), an opioid-like peptide that can drive gut inflammation in susceptible people. A2-only milk (from certain breeds, sold as "A2 Milk" in some markets), goat milk, and sheep milk largely avoid A1 casein. This is a promising but under-studied area.
Clinically: many patients report real benefit from a 4–6 week dairy elimination followed by structured reintroduction. If endo belly, bloating, or cramping improve off dairy and flare on reintroduction, you have your answer. If nothing changes, put dairy back — cutting it unnecessarily reduces calcium, vitamin D, and protein intake.
Gluten
The most-cited endo-specific gluten study is Marziali et al. 2012, which followed 207 women with severe, painful endometriosis on a 12-month gluten-free diet. About 75% reported significant improvement in pelvic pain versus baseline, with improvements in physical functioning, mental health, and social role domains. The trial was uncontrolled, so expectation effects and concurrent lifestyle changes can't be separated out — but the effect size was large.
The broader debate is about non-celiac gluten sensitivity, a real but fuzzy entity where patients without celiac disease or wheat allergy still respond to gluten removal. Some of that may be wheat fructans (a FODMAP) rather than gluten per se. For practical purposes the mechanism matters less than whether a trial helps you.
Reasonable approach: strict gluten-free for 4–6 weeks, tracking pain and GI symptoms. If clearly better, continue and consider a blinded reintroduction (a family member prepares identical-looking gluten and gluten-free foods). If no change, return to whole-grain gluten foods — they are nutritionally valuable and not intrinsically harmful. Before going gluten-free long-term, rule out celiac first with blood tests while you are still eating gluten, because going gluten-free first invalidates the test.
Xenoestrogens and Endocrine Disruptors
Endometriosis is an estrogen-dependent disease, and a growing body of evidence implicates environmental endocrine disruptors in its pathogenesis. The main offenders:
- BPA and BPS — in polycarbonate plastics, thermal receipts, the linings of most food cans.
- Phthalates — in soft plastics, vinyl shower curtains, synthetic fragrances, many cosmetics.
- Parabens — preservatives in lotions, shampoos, makeup.
- PFAS ("forever chemicals") — non-stick cookware, water-resistant fabrics, fast-food wrappers, contaminated drinking water.
- Pesticide residues — especially organochlorines and certain fungicides on conventional produce.
Practical, non-obsessive steps: store food in glass or stainless steel, especially for hot or fatty foods; never microwave in plastic. Use a reverse-osmosis or activated-carbon water filter certified for PFAS removal. Check personal care products through the EWG Skin Deep database. Buy organic for the Dirty Dozen produce list. Replace non-stick pans with cast iron or stainless steel as they wear out. You cannot achieve zero exposure — the goal is to lower the lifetime dose enough to matter.
Alcohol
Alcohol modestly raises circulating estrogen by reducing liver clearance and may interfere with progesterone production. Meta-analyses show a small positive association with endo risk, strongest at higher intakes.
Reasonable target: under 7 drinks per week, with several alcohol-free days. Many patients do particularly poorly with alcohol during the luteal phase (week before menstruation). Cut alcohol entirely in that window and see if your worst days soften.
Caffeine
Observational evidence on caffeine and endo is inconsistent — some studies show a small risk increase at heavy intake, others nothing. Caffeine does transiently raise cortisol and can worsen anxiety, sleep, and pelvic-floor muscle tension in sensitive patients.
Individualize. If coffee flares your symptoms, cut back or switch to decaf or green tea. If it doesn't, keep enjoying it. The evidence does not support a universal prohibition.
Supplements with Some Evidence
Listed in rough order of evidence strength. Start one at a time — if you begin five on Monday and feel better Friday, you'll never know which one helped.
- Curcumin — 500–2,000 mg daily of a bioavailability-enhanced form (piperine-paired, phospholipid-complex like Meriva, or Theracurmin). Standard turmeric powder absorbs poorly. Small trials show reductions in pelvic pain and inflammatory markers.
- N-acetylcysteine (NAC) — 600 mg three times daily. Porpora et al. 2013 randomized 92 women with ovarian endometriomas to NAC or placebo; the NAC group showed reduced cyst size, reduced pain, and fewer required surgeries.
- Vitamin D — aim for serum 25-OH vitamin D of 40–60 ng/mL. Typical maintenance 2,000–5,000 IU daily, but test and dose to your level. Linked to reduced pelvic pain in several small trials.
- Magnesium glycinate — 200–400 mg evening. Reduces dysmenorrhea in meta-analyses, supports sleep, helps pelvic-floor relaxation. Glycinate is gentle on the gut.
- Melatonin — a 2013 Brazilian RCT at 10 mg nightly showed reductions in pelvic pain, dysmenorrhea, and dyschezia versus placebo. Start at 3 mg and titrate only if needed.
- Quercetin — 500 mg twice daily. Mast-cell stabilizer, useful with the endo–MCAS overlap (histamine flares, flushing, food sensitivities). Pair with bromelain for absorption.
- Resveratrol — 100–500 mg daily. Preliminary evidence; reasonable to try, not essential.
Tell your prescriber about every supplement, especially if you are on hormonal therapy, anticoagulants, or planning surgery. Stop most supplements 10–14 days pre-op.
Exercise
Regular moderate exercise reduces inflammatory prostaglandins, improves insulin sensitivity, and speeds gut transit (which helps the liver excrete conjugated estrogen rather than recirculate it through the enterohepatic pathway). Exercise also down-regulates central pain sensitization over months.
Target: 3–5 sessions per week, 30+ minutes each, mixing cardiovascular work (walking, swimming, cycling) with resistance training (2 sessions weekly of full-body strength work). Intensity should be tolerable, not punishing — high-intensity workouts the week before your period may flare symptoms for some patients. Swap for walking or yoga in your worst days.
If exercise hurts your pelvis, that is not a reason to stop exercising — it is a signal to adjust and to involve a pelvic-floor physical therapist who can modify loading and address the muscle dysfunction driving the pain.
Yoga and Mind-Body Work
A 2017 Brazilian RCT by Gonçalves and colleagues randomized women with endo-associated pelvic pain to a structured yoga program versus a waitlist control and found significant reductions in daily pain scores and improvements in quality of life in the yoga group. The evidence is modest in size but real.
Styles with the best fit: restorative yoga, yin, gentle hatha, and the Saraswati School-style programs developed specifically for pelvic pain. Avoid hot yoga and strongly compressive poses during flares. Slow diaphragmatic breathing (box breathing, 4–7–8 breathing), meditation apps (Insight Timer, Calm, Curable for pain specifically), and progressive muscle relaxation all contribute modestly to pain reduction through the vagal/parasympathetic pathway.
Sleep
Sleep is the cheapest, most effective anti-inflammatory intervention you have. Adults with chronic pain conditions who sleep less than 6 hours report measurably higher pain scores and higher inflammatory markers (CRP, IL-6) than those sleeping 7–9 hours.
Basics that matter:
- Consistent bed and wake times, including weekends.
- Dark, cool bedroom (65–68°F).
- Last caffeine by early afternoon.
- Screens off 60–90 minutes before bed, or use blue-light reduction.
- Magnesium glycinate or melatonin if you need pharmacologic help.
- Treat pain at bedtime — heat, NSAIDs if appropriate, positioning pillows — rather than lying awake with it.
If you have suspected obstructive sleep apnea or restless legs, get evaluated. Untreated sleep disorders will nullify most other interventions.
Stress Reduction
Chronic stress elevates cortisol, which in turn modulates inflammatory cytokines and amplifies pain perception in the central nervous system. Endo patients also carry a heavy load of medical trauma — years of dismissal, delayed diagnosis, failed treatments, painful exams. That trauma is real and deserves direct attention.
Evidence-based approaches:
- Mindfulness-based stress reduction (MBSR) — 8-week structured programs with measurable effects on chronic pelvic pain.
- Cognitive behavioral therapy for chronic illness — not about convincing you the pain isn't real; it's about reducing the amplifying effect of catastrophizing and anxiety on pain signaling.
- Therapy with a clinician experienced in medical trauma or chronic illness — consider EMDR or somatic therapy if medical procedures, pelvic exams, or past dismissals are still dysregulating.
Seeing a therapist does not mean your pain is psychological. It means you are treating the part of the nervous system that turns volume up on every signal.
Environmental Exposures
Beyond the xenoestrogen categories above, a few household-level swaps are worth making gradually:
- Cleaning products — fragrance-free, low-VOC options, or plain vinegar and baking soda.
- Unscented personal care — "fragrance" on a label is an umbrella term for undisclosed chemicals, often including phthalates.
- Avoid BPA-lined cans — use tetra-pak cartons, glass jars, cooked dried beans, and frozen tomatoes when possible.
- Air quality — a HEPA purifier in the bedroom and good kitchen ventilation modestly reduce indoor VOC load.
The largest wins are the kitchen (plastics, cans, water) and personal care. The rest is incremental.
What Doesn't Have Evidence
A candid list of popular recommendations that currently lack good data in endo:
- Expensive "hormone-balancing" coaching protocols. If the pitch includes "reverse endo," walk away.
- DIM (diindolylmethane) without a specific evidence base for endo — mechanistic, not clinical.
- Castor oil packs — zero RCT evidence in endo. Harmless, but not a treatment.
- Homeopathic preparations and alkaline/structured water products.
- Expensive "liver detox" cleanses — your liver already detoxifies; these are typically high-sugar, low-protein.
- "Endometriosis diet" coaching packages for hundreds of dollars monthly. The underlying principles are the Mediterranean pattern, which is free.
Spend your money on an excision surgeon, a pelvic-floor PT, quality fish oil, and groceries — in that order.
How to Structure a Personal Lifestyle Trial
Because endo fluctuates, every intervention looks like it works the first month you try it. To actually learn what helps you:
- Pick one intervention at a time. Not three. One.
- Baseline for one full cycle before changing anything. Track daily pain (0–10), bleeding days, bowel and bladder symptoms, mood, sleep hours.
- Run the intervention for 8–12 weeks — that is roughly two to three full menstrual cycles, enough signal to distinguish from noise.
- Compare cycle-matched days, not weekday averages. Day 1 of your period against day 1 of your period.
- Reintroduce to test for elimination diets. Improvement without a flare on reintroduction may be coincidence.
- Stack gradually. Once you've identified something that works, keep it and add the next candidate.
- Stop what doesn't help. Don't carry dead rules around. If three months of strict gluten-free did nothing and reintroduction flared nothing, gluten is not your issue.
This approach is unglamorous but it is how you separate real personal responders from noise. Over a year or two, most patients assemble a short list of interventions that genuinely move their symptoms — usually some combination of omega-3s, magnesium, vitamin D repletion, a reduced red-meat Mediterranean pattern, regular movement, and attention to sleep and stress. That short list is worth far more than any influencer protocol.
Key Research Papers
- Yamamoto A, Harris HR, et al. A prospective cohort study of meat and fish consumption and endometriosis risk. Human Reproduction. 2018.
- Porpora MG, et al. A promise in the treatment of endometriosis: an observational cohort study on ovarian endometrioma reduction by N-acetylcysteine. Evidence-Based Complementary and Alternative Medicine. 2013.
- Marziali M, et al. Gluten-free diet: a new strategy for management of painful endometriosis related symptoms? Minerva Chirurgica. 2012;67(6):499–504. (PubMed PMID: 23334113)
- ESHRE Endometriosis Guideline Group. ESHRE guideline: endometriosis. Human Reproduction Open. 2022.
Live PubMed Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on diet, supplements, and lifestyle in endometriosis:
- Red meat and endometriosis risk
- Omega-3 fatty acids and dysmenorrhea
- N-acetylcysteine and ovarian endometrioma
- Vitamin D and endometriosis
- Gluten-free diet and endometriosis
- Bisphenol A, phthalates, and endometriosis
- Curcumin and endometriosis
- Melatonin and endometriosis pelvic pain
Connections
- Endometriosis
- Omega-3 Fatty Acids
- Magnesium Glycinate
- Turmeric
- Quercetin
- Laparoscopy: Excision vs Ablation
- Diagnosis Delay and Imaging
- Hormonal Therapy Options
- Pelvic Floor Therapy and Central Sensitization
- Endo Belly and Gut Connection
- Fertility and Endometriosis
- Adenomyosis Overlap
- Vitamin D3
- Gluten-Free Diet Practical Guide
- Iron
- Magnesium
- NAC
- Ultra Processed Foods