Pelvic Floor Therapy and Central Sensitization in Endometriosis
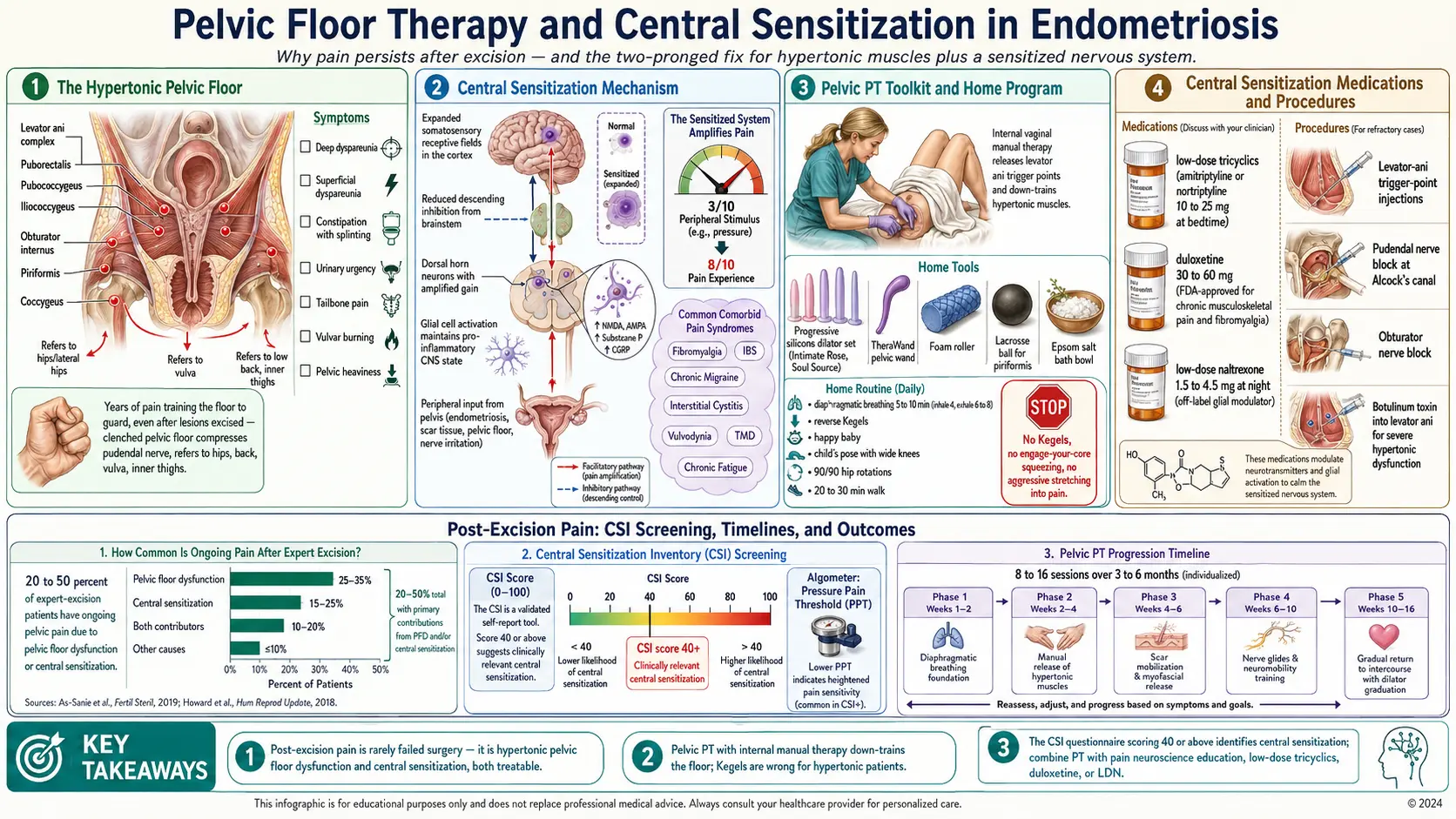
Table of Contents
- The Post-Excision Disappointment
- Two Overlapping Drivers
- Pelvic Floor Dysfunction — What It Is
- Symptoms of a Hypertonic Pelvic Floor
- Central Sensitization — What It Is
- Screening — CSI and Pressure Pain Thresholds
- Pelvic PT — What It Actually Is
- Finding a Qualified Pelvic PT
- What the First Session Looks Like
- Manual Techniques
- Home Tools
- Home Exercises
- What NOT to Do
- Central Sensitization Management
- Nerve Blocks and Trigger Point Injections
- Timeline Expectations
- When to Escalate
- Key Research Papers
- Connections
- Featured Videos
The Post-Excision Disappointment
You spent years convincing doctors your pain was real. You finally found a skilled excision surgeon, recovered from laparoscopy, and expected the curtain to lift. Then, somewhere between weeks six and twelve post-op, you realized the pain was still there. The crushing period pain may be genuinely gone — but the deep dyspareunia, the burning in your lower pelvis, the ache behind the pubic bone, the feeling of a clenched fist inside you: those survived the surgery.
If that is where you are, hear this clearly: you are not broken and your surgery did not "fail." Roughly 20–50% of patients who undergo expert excision have meaningful ongoing pelvic pain afterward. The lesions are gone, the pathology report is clean, and yet the symptoms continue. This is not a sign the disease was missed or the surgeon was incompetent. It is a sign endometriosis does something cutting out tissue cannot reverse — it trains the muscles of your pelvis and the wiring of your nervous system to generate pain on their own.
Two mechanisms produce this residual pain, and both are treatable.
Two Overlapping Drivers
Post-excision pelvic pain is almost never one thing. The two engines that keep it running are pelvic floor dysfunction — chronic involuntary tightening of the muscles of your pelvis — and central sensitization, a rewiring of the brain and spinal cord that amplifies incoming signals. The two feed each other. Tight muscles send a low-level pain signal upstream, which trains the CNS to expect pain. The sensitized CNS then interprets ordinary sensations — a tampon, a bowel movement, a full bladder, intercourse — as painful, which triggers reflexive guarding, which tightens the floor further.
You cannot escape this loop by cutting out lesions. You have to interrupt it at both ends: muscle and nerve, body and brain.
Pelvic Floor Dysfunction — What It Is
Your pelvic floor is a hammock of muscles slung between the pubic bone and the tailbone. The main layers are the levator ani complex (puborectalis, pubococcygeus, iliococcygeus), the obturator internus along the inner hip, the piriformis deep in the buttock, and the coccygeus near the tailbone. They support the bladder, uterus, and rectum, close the urethra and anus, and reflexively guard whenever something hurts in the abdomen or pelvis.
That reflexive guarding is the problem. Every flare, every painful period, every painful bowel movement, every painful attempt at intercourse tells your pelvic floor to clench. Multiply that by years — often decades, because endometriosis is diagnosed on average seven to ten years late — and the muscles forget how to let go. What started as a protective response becomes hypertonic pelvic floor dysfunction: a floor stuck in the "on" position, even after the lesions are gone.
Hypertonic floors do not just ache. They compress nerves (the pudendal nerve runs directly through the floor), trap blood flow, pull on the pubic symphysis, and refer pain out to the hips, low back, tailbone, vulva, and inner thighs. Many patients describe it as "a clenched fist I can't unclench."
Symptoms of a Hypertonic Pelvic Floor
A hypertonic pelvic floor has a recognizable fingerprint. You may have some or all of:
- Deep dyspareunia — pain with deep penetration during intercourse, often described as "hitting a wall" or "running into something bruised."
- Superficial dyspareunia — burning or tearing at the vaginal opening with initial penetration.
- Constipation and painful bowel movements, a feeling of incomplete emptying, or the need to "splint" with a hand on the perineum.
- Urinary urgency, frequency, or hesitancy — the sensation of needing to go without being able to start, or feeling like you never fully empty.
- Tailbone (coccyx) pain, especially sitting on hard surfaces.
- Hip pain, groin pain, low back pain that moves and never quite localizes.
- Burning vulvar pain or generalized vestibule tenderness.
- Pain with tampon insertion, pelvic exams, or cervical cancer screening.
- A baseline feeling of heaviness, pressure, or fullness in the pelvis that does not correlate with your cycle.
If you recognized more than three of those, the floor is almost certainly part of what is still hurting.
Central Sensitization — What It Is
Central sensitization (CS) is what happens when your nervous system turns up the gain on pain. Under normal conditions, a 3/10 stimulus produces a 3/10 signal. In a sensitized system, the dorsal horn of the spinal cord amplifies that same signal so it arrives at the brain as an 8/10. The threshold for pain drops, pain lingers longer after a stimulus ends, and sensations that should not hurt — light touch, warm water, clothing pressure — begin to.
The mechanism is real biology, not imagination or weakness. Repeated nociceptive input produces measurable changes: increased excitability of spinal cord neurons, decreased descending inhibition from the brainstem, expansion of receptive fields in the somatosensory cortex, and glial cell activation that maintains a pro-inflammatory state in the CNS. These changes outlive the original tissue injury — which is why patients who had endometriosis excised cleanly can still hurt for months or years afterward.
CS also explains why endometriosis travels with a cluster of comorbid pain syndromes: fibromyalgia, IBS, chronic migraine, interstitial cystitis, vulvodynia, temporomandibular disorder, chronic fatigue. They share the same amplification mechanism. If you have endometriosis plus two or three of those, you almost certainly have central sensitization on top of whatever peripheral pathology remains.
Screening — CSI and Pressure Pain Thresholds
There is a validated self-administered questionnaire for this called the Central Sensitization Inventory (CSI). It has 25 items scored 0–4. A total score of 40 or above suggests clinically relevant central sensitization. It is free, takes five minutes, and is available through most pain-management clinics or online. Bring the completed form to your next appointment.
A trained pelvic PT or pain physician can also measure pressure pain thresholds with a handheld algometer at standardized body points. Lowered thresholds at sites far from the pelvis (the forearm, the shin) — not just at the pelvic floor itself — indicate that the amplification is central, not local.
Pelvic PT — What It Actually Is
"Pelvic physical therapy" sounds like it might mean Kegels in a gym. It is nothing like that. Pelvic PT is a subspecialty practiced by clinicians with advanced post-graduate training in pelvic anatomy, internal manual techniques, and pain science. A qualified pelvic PT treats you with external hands-on work (hips, abdomen, diaphragm, low back) plus internal vaginal work — and in some cases internal rectal work — to reach the floor directly.
If that sounds intense, it is. It is also the single most effective intervention for hypertonic pelvic floor dysfunction. For endometriosis patients with ongoing pain, pelvic PT is not optional adjunct therapy — it is first-line treatment.
Finding a Qualified Pelvic PT
Not every PT clinic with a "pelvic health" banner on the website does this work at the depth you need. Look for these markers:
- APTA Pelvic Health directory. The American Physical Therapy Association maintains a searchable directory of members of its Academy of Pelvic Health Physical Therapy (
aptapelvichealth.org). - Herman & Wallace-trained practitioners. The Herman & Wallace Pelvic Rehabilitation Institute is the gold-standard training pathway; their practitioner directory is searchable by zip code.
- Internal-release certified. Ask directly: "Do you perform internal vaginal manual therapy?" If the answer is no, you are in the wrong clinic.
- Endometriosis experience. Ask how many endometriosis patients they see per week. A PT who sees endo patients weekly thinks differently than one who sees incontinence and postpartum clients.
- Trauma-informed. A good pelvic PT moves at your pace, explains every technique before performing it, and stops instantly when asked. Trauma-informed practice is a trained skill, not a marketing term.
What the First Session Looks Like
The first visit is usually 60–90 minutes and is mostly conversation and external assessment. Expect an extensive intake covering medical, surgical, and menstrual history, bowel and bladder habits, sexual function, and pain map. The PT will watch you breathe, walk, and move. External palpation of the hips, abdomen, and low back comes next.
The internal exam — if you consent and are ready — happens at the end of the first visit or at the second. You are draped, knees up, and the PT inserts one gloved, lubricated finger to assess tone, tenderness, and trigger points in each major pelvic floor muscle. It is not a gynecologic exam: no speculum, no cervical contact. You can stop at any point. Many patients report it is far less uncomfortable than a pap smear.
You will leave with a short home program — usually diaphragmatic breathing, a hip mobility drill, and one or two stretches. Session one is orientation, not heroics.
Manual Techniques
Once treatment begins, expect a rotating toolkit:
- Myofascial release — sustained pressure on tight fascial bands along the abdomen, hip flexors, inner thighs, and superficial pelvic floor.
- Trigger point release — focused pressure on hyperirritable muscle knots, both external (obturator, piriformis) and internal (levator ani).
- Scar mobilization — massage across laparoscopy port sites. Scars that look fine on the surface can tether deeper fascia and refer pain for years.
- Visceral mobilization — gentle manipulation of the abdominal viscera to restore glide between the uterus, bladder, bowel, and peritoneum. Especially relevant for adhesion-prone endo patients.
- Nerve glides — movements that gently slide the pudendal and obturator nerves through their sheaths, reducing entrapment pain.
Home Tools
Between sessions, the work continues at home with a small equipment list:
- Silicone dilators (progressive set of four to seven sizes). Intimate Rose and Soul Source are well-reviewed brands. Use 10–15 minutes daily with water-based lube, starting at the largest size you can tolerate without pain.
- Pelvic wand — a curved silicone tool for trigger points out of finger reach. The TheraWand and Intimate Rose Pelvic Wand are the two common choices.
- Foam roller for external work on hip flexors, glutes, and mid-back.
- Lacrosse ball for piriformis and obturator trigger points against a wall or floor.
- Epsom salt baths — 20 minutes in warm water with 1–2 cups of Epsom salts, three to five evenings a week. Heat and quiet are both nervous-system medicine.
Home Exercises
For a hypertonic floor, the goal of exercise is down-training — teaching the muscles to let go — not strengthening. A typical daily routine:
- Diaphragmatic breathing — the pelvic floor moves in sync with the diaphragm. On a deep belly breath, both descend and lengthen. Five to ten minutes of slow belly breathing (inhale 4, exhale 6–8) is the foundation of the entire program.
- Reverse Kegels — the intentional opposite of a Kegel. Gently bulge or release the floor downward, as if starting to urinate. Pair with the exhale.
- Happy baby, child's pose (wide knees), butterfly stretch — passive openers for the pelvic outlet; breathe into the pelvis for 2–3 minutes each.
- Hip mobility work — 90/90 hip rotations, pigeon, figure-four — to unload obturator and piriformis.
- Walking — 20–30 minutes daily at an easy pace. Down-regulates arousal and promotes pelvic blood flow without loading the floor.
What NOT to Do
Most generic "pelvic health" advice on the internet is written for the opposite problem — weak, leaking floors after childbirth — and is actively harmful for a hypertonic floor. Avoid:
- Kegels. Squeezing an already-clenched muscle makes it tighter. Until a qualified pelvic PT has examined you and prescribed Kegels specifically, assume they are wrong for you.
- "Squeeze and hold" protocols — yoga, pilates, or fitness cues to "engage your core" or "lift your pelvic floor" continuously.
- Aggressive stretching that pushes into pain. The floor responds to pain with more guarding. Stay at the edge of sensation, not past it.
- Heavy lifting and high-impact loading during active flares — until the floor has been retrained.
- Holding urine or stool past the urge. Chronic pushback trains the floor to stay contracted.
Central Sensitization Management
Pelvic PT alone is often not enough when the nervous system has been amplifying pain for a decade or more. A parallel track targets the central piece directly:
- Pain neuroscience education. Understanding how pain actually works is, surprisingly, therapeutic. Lorimer Moseley and David Butler's book Explain Pain is the standard text; Moseley's free YouTube talks cover the same material. Patients who grasp that pain is generated by the brain's interpretation of signals — not a direct readout of tissue damage — need less medication and report less disability.
- Graded exercise / graded exposure. Steady increases in activity below the flare threshold — walk 20 minutes today even though you could walk 40 — so the nervous system relearns that movement is safe.
- CBT for chronic pain (CBT-CP). Targets catastrophizing, fear-avoidance, and hypervigilance. Strong evidence base.
- Mindfulness-based stress reduction (MBSR). Eight-week protocols are widely available and produce measurable reductions in pain interference.
- Low-dose tricyclics — amitriptyline or nortriptyline 10–25 mg at bedtime, far below antidepressant doses. Quiet dorsal-horn amplification, improve sleep, cheap.
- SNRIs — duloxetine 30–60 mg, FDA-approved for chronic musculoskeletal pain and fibromyalgia; often effective for pelvic CS.
- Low-dose naltrexone (LDN) — 1.5–4.5 mg at night. Off-label, growing evidence in fibromyalgia, IBS, and chronic pelvic pain via glial modulation. Compounded; $30–$60 per month.
Nerve Blocks and Trigger Point Injections
When PT plus home work plus central-pain medication still leaves you stuck, procedural interventions can unlock progress. Performed by pain specialists, gynecologists with pelvic pain fellowships, or interventional radiologists:
- Trigger point injections — local anesthetic (with or without steroid) into the worst knots in levator ani, obturator internus, or piriformis. Unblocks stuck PT progress.
- Pudendal nerve block — anesthetic around the pudendal nerve at Alcock's canal; both diagnostic and therapeutic for pudendal neuralgia.
- Obturator nerve block — for persistent inner-thigh / deep-groin pain.
- Botulinum toxin injection into levator ani — for severe hypertonic dysfunction unresponsive to manual therapy. Effects last 3–6 months and buy a window for PT to retrain the pattern.
Timeline Expectations
Set realistic expectations up front, because this is where most patients quit. Meaningful change in pelvic floor dysfunction typically takes 3–6 months of weekly PT plus daily home work. Some patients feel 30% better after one or two sessions; others feel worse for several weeks before they feel better, because releasing a long-compensating floor exposes other imbalances.
Rewiring central sensitization takes longer — 6–18 months — and progress is nonlinear. The trend is what matters, not any single day. Consistency, sleep, and steady down-regulation of life stressors predict recovery better than any single drug or procedure.
When to Escalate
If you have done six months of competent pelvic PT, a fair medication trial, and reasonable pacing, and pain is still running your life, it is time to re-examine the peripheral picture. Persistent pain despite all of the above should prompt a careful workup for:
- Missed or recurrent endometriosis — particularly deep infiltrating lesions on the uterosacral ligaments, cul-de-sac, bowel, or diaphragm. A second-opinion consult with a high-volume excision surgeon is reasonable.
- Post-surgical adhesions tethering bowel, ovary, or pelvic sidewall.
- Adenomyosis — often missed on exam and only reliably diagnosed on high-quality pelvic MRI. See the adenomyosis overlap page.
- Interstitial cystitis / bladder pain syndrome — a frequent endo comorbid; hydrodistention under anesthesia can confirm.
- Vulvodynia — localized or generalized vulvar burning, often comorbid and treatable with specific topical and oral therapies.
- Pudendal neuralgia — sharp burning in a pudendal distribution, worse sitting and relieved standing. Diagnostic block confirms.
The core message: if your pain did not go away after excision, it is not because you are broken or the surgery "didn't work." Endometriosis trains the nervous system and the muscles of the pelvis in ways that cutting out lesions alone does not undo. The tools to undo that training exist and they work.
Key Research Papers
- Aredo JV, Heyrana KJ, Karp BI, Shah JP, Stratton P. Relating chronic pelvic pain and endometriosis to signs of sensitization and myofascial pain and dysfunction. Semin Reprod Med. 2017.
- Woolf CJ. Central sensitization: implications for the diagnosis and treatment of pain. Pain. 2011.
- Wurn BF, Wurn LJ, King CR, Heuer MA, Roscow AS, Scharf ES, Shuster JJ. Treating female infertility and improving IVF pregnancy rates with a manual physical therapy technique. MedGenMed. 2004;6(2):51. (Pelvic PT in endometriosis outcomes.)
- Becker CM, et al. ESHRE guideline: endometriosis. Hum Reprod Open. 2022.
Live PubMed Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on pelvic floor dysfunction, central sensitization, and endometriosis pain:
- Pelvic floor dysfunction and endometriosis
- Central sensitization and chronic pelvic pain
- Pelvic physical therapy and dyspareunia
- Myofascial release for pelvic pain
- Central Sensitization Inventory validation
- Low-dose naltrexone in chronic pain
- Pudendal neuralgia diagnosis and treatment
- Botulinum toxin for pelvic floor dysfunction
Connections
- Reproductive Medicine
- Adenomyosis Overlap
- Endometriosis
- Laparoscopy: Excision vs Ablation
- Fibromyalgia
- Chronic Pain
- Interstitial Cystitis
- Migraine
- Diagnosis Delay and Imaging
- Hormonal Therapy Options
- Fertility and Endometriosis
- Endo Belly and Gut Connection
- Diet and Lifestyle
- Bladder and Bowel Endometriosis
- Irritable Bowel Syndrome
- Infertility
- Central Sensitization Explained
- Chronic Fatigue Syndrome
- Uterine Fibroids