Endometriosis Diagnosis Delay and Imaging
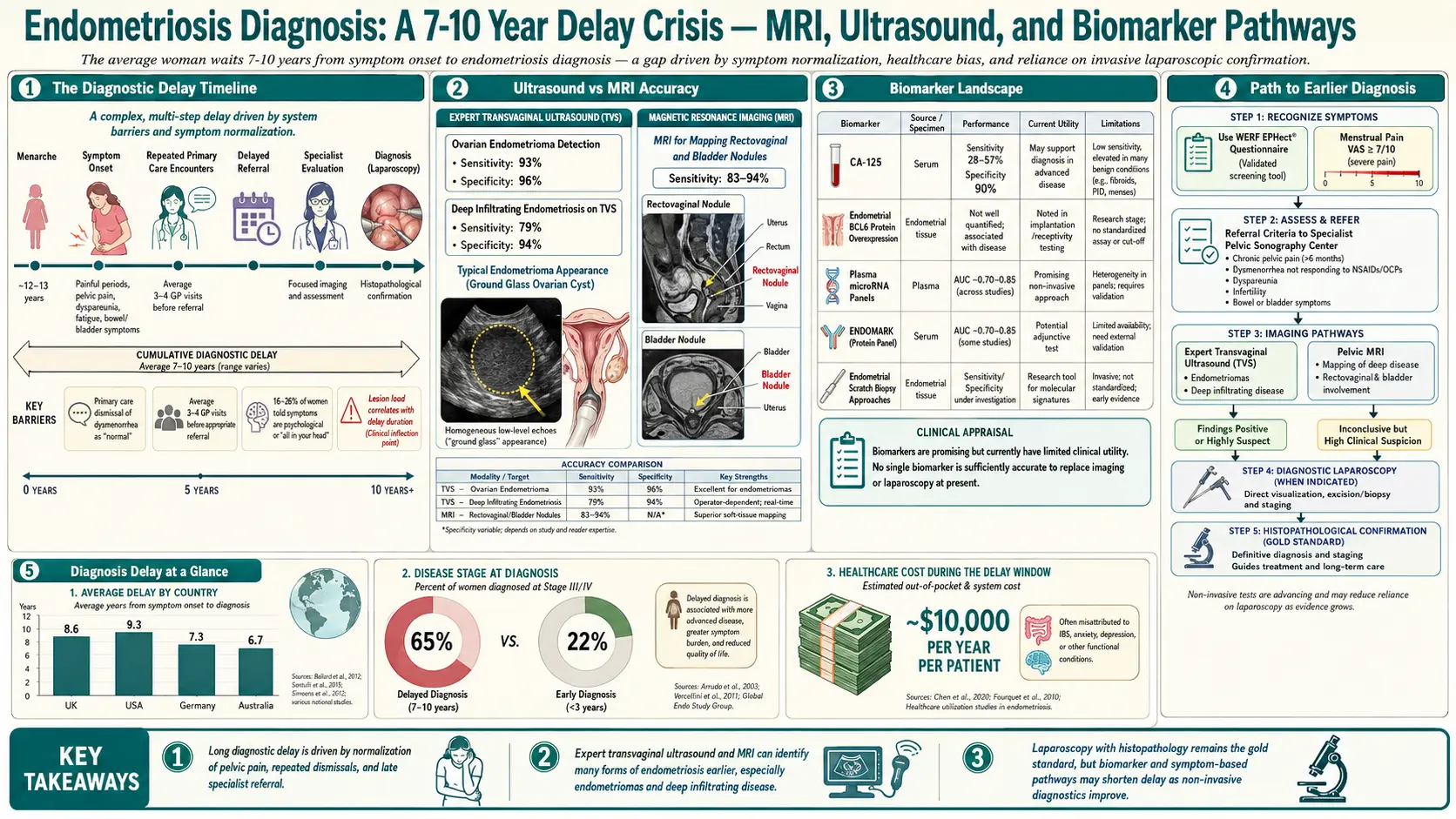
Table of Contents
- The 7–10 Year Diagnostic Delay — Why It Happens
- What Endometriosis Is — In Plain Language
- Clinical Diagnosis and Empirical Treatment
- Transvaginal Ultrasound
- Dynamic "Sliding Sign" Ultrasound
- MRI with Pelvic/Endo Protocol
- Diagnostic Laparoscopy — the Gold Standard
- CA-125 — Why It Is Not a Screening Test
- Emerging Biomarkers
- Scripts for Your Gyn Appointment
- Finding an Excision Specialist
- Symptom Tracking to Build Your Case
- When to Push Harder
- What to Expect After Diagnosis
- Red Flags for Urgent Workup
- Key Research Papers
- Connections
- Featured Videos
If your pain has been dismissed for years, you are not alone — and you are not exaggerating. The average patient with endometriosis waits seven to ten years for a diagnosis, not because the disease is rare but because the system normalizes menstrual pain and because the tools to see endometriosis require specialist training. This article is a practical map through the diagnostic process.
The 7–10 Year Diagnostic Delay — Why It Happens
Study after study puts the average delay between symptom onset and confirmed endometriosis diagnosis at 7 to 10 years. Some cohorts report longer. The delay has four compounding causes, and understanding them is the first step in cutting yours short.
Symptoms are dismissed as "normal period pain." Dysmenorrhea is framed as something to tolerate. Pain that keeps you home from school or work is not normal; pain that makes you vomit is not normal; pain that pain medication does not touch is not normal. Each of those is a reason for imaging and referral, not reassurance.
Pain normalization inside the patient. If you have hurt since your first period, you have no baseline for a pain-free cycle. Patients routinely under-report on a 1–10 scale because their personal 5 is what most people would call a 9.
The primary care gap. Most pelvic pain first lands in front of a general practitioner. Endometriosis is barely covered in medical school. The symptom pattern gets rerouted to ibuprofen, birth control pills, and "come back if it gets worse." Worse is rarely defined.
Multiple mis-diagnoses before the right one. The symptom map of endometriosis overlaps with several common conditions, and patients are often told they have one of them first:
- Irritable bowel syndrome (IBS) — because bowel symptoms flare with the cycle, especially if bowel endometriosis is present.
- Interstitial cystitis / painful bladder syndrome — because bladder endometriosis or referred pelvic pain causes urinary urgency.
- Pelvic inflammatory disease (PID) — because the pain is deep and cyclic, and clinicians default to infection.
- Anxiety, depression, or "somatization" — the oldest and most damaging misdiagnosis. Pain plus female plus negative imaging often produces a psychiatric referral instead of a surgical one.
- Ovarian cysts of unclear origin — endometriomas get drained or watched without anyone naming the underlying disease.
You may have been told several of these. None of them rule out endometriosis, and several (especially IBS and interstitial cystitis) commonly coexist with it.
What Endometriosis Is — In Plain Language
Endometriosis is tissue that behaves like the lining of the uterus but grows outside it — on the ovaries, fallopian tubes, bowel, bladder, peritoneum (the sheet that lines the pelvic cavity), and, less commonly, the diaphragm, lungs, or surgical scars. With every menstrual cycle, these deposits respond to the same hormonal signals as the uterine lining: they inflame, bleed, and provoke scarring in tissues that have no way to shed blood. Over years, the inflammation produces adhesions (bands of scar tissue gluing organs together) and deep infiltrating lesions that invade the bowel wall, ureters, or rectovaginal space.
Two ideas about endometriosis still circulate in clinics and among relatives, and both are wrong.
"Just get pregnant — that cures it." Pregnancy sometimes pauses symptoms because ovulation stops and estrogen patterns shift, but the disease does not disappear. Many patients flare harder postpartum. Endometriosis is also a leading cause of infertility, so "get pregnant" is often not an option without reproductive assistance — and no one should have a child to treat a disease.
"Just have a hysterectomy." Endometriosis is, by definition, tissue outside the uterus. Removing the uterus does not remove the disease. Hysterectomy with ovary removal can help if adenomyosis (a separate condition involving the uterine muscle) is also present, but it does not cure endometriosis and is not an appropriate first-line treatment, especially for young patients. The correct surgery is excision of the implants themselves.
Clinical Diagnosis and Empirical Treatment
Modern guidelines, including the ESHRE 2022 Endometriosis Guideline, no longer require surgical confirmation before starting treatment. If your symptom pattern fits — severe dysmenorrhea, cyclic pelvic pain, dyspareunia (pain with sex), cyclic bowel or bladder pain, infertility — a clinician can make a clinical diagnosis and begin empirical treatment with NSAIDs and hormonal therapy. This is a legitimate starting point and it shortens the delay.
What clinical diagnosis is not: a reason to refuse imaging or surgery when symptoms fail to respond. If three to six months of a first-line hormonal regimen does not improve your pain, the next step is advanced imaging and a surgical referral — not another brand of pill.
Transvaginal Ultrasound
Transvaginal ultrasound (TVUS) is the first-line imaging study. It is cheap, widely available, and safe. What it sees depends almost entirely on who is doing the scan.
What a standard TVUS can show:
- Endometriomas (ovarian "chocolate cysts") — highly characteristic homogeneous low-level echoes, often called the "ground-glass" appearance. Sensitivity is excellent, above 90%.
- Hydrosalpinx (fluid-filled fallopian tubes) — a common coexisting finding.
- Adenomyosis features in the uterine wall (asymmetric thickening, myometrial cysts, linear striations).
What a standard TVUS cannot show:
- Peritoneal (superficial) endometriosis — these flat implants on the pelvic sidewalls are invisible on routine imaging. A negative ultrasound does not rule out endometriosis. Full stop.
- Small deep infiltrating lesions outside the routine scan zones.
A specialist endometriosis sonographer performing a targeted scan can see much more: deep infiltrating lesions in the rectovaginal septum, uterosacral ligament nodules, bladder-wall disease, and bowel involvement. These scans take 30–60 minutes and follow the IDEA consensus protocol. Most general radiology practices do not offer this. Ask for "advanced pelvic ultrasound for endometriosis" or "IDEA-protocol transvaginal ultrasound" and expect to travel for it.
Dynamic "Sliding Sign" Ultrasound
The sliding sign is a real-time maneuver performed during a specialist ultrasound. The sonographer uses gentle pressure with the probe to watch whether the anterior rectal wall slides freely against the back of the uterus and cervix. In a normal pelvis, the two surfaces glide apart. In a pelvis with deep infiltrating endometriosis, adhesions fix them together — the sliding sign is negative, meaning the organs are stuck.
A negative sliding sign is a strong predictor of pouch of Douglas obliteration, the frozen-pelvis pattern surgeons need to know about before they operate. It also correlates with bowel involvement and predicts more complex surgery. In skilled hands this single maneuver maps the geography of your disease before anyone opens you up — and is the best argument for traveling to a specialist center.
MRI with Pelvic/Endo Protocol
Pelvic MRI is the second imaging tool. It is ordered when ultrasound is suggestive but incomplete, when deep infiltrating disease is suspected, or when surgical planning requires a roadmap. A generic pelvic MRI is not the same as a dedicated endometriosis protocol. Ask for a pelvic MRI with endometriosis protocol, which includes:
- Thin-section T2-weighted sequences through the entire pelvis.
- Fat-suppressed T1 sequences to detect blood products in implants.
- Vaginal and rectal opacification gel in some centers to improve contrast at the cul-de-sac and rectovaginal septum.
- A radiologist with endometriosis-specific experience reading the study.
What MRI shows well: deep infiltrating endometriosis, rectovaginal and uterosacral nodules, bladder-wall lesions, bowel involvement (with measurement of depth of invasion), endometriomas, adenomyosis, and adhesion patterns. It is especially valuable for surgical planning because it shows the ureters and can flag hydronephrosis from ureteral compression.
What MRI does not reliably show: superficial peritoneal endometriosis — the same blind spot as ultrasound. A clean MRI in a patient with classic symptoms still does not rule out disease. Surgery remains necessary when imaging is negative but symptoms persist.
Diagnostic Laparoscopy — the Gold Standard
Laparoscopy is minimally invasive surgery in which a camera is inserted through a small incision near the navel and the pelvis is inspected directly. It is the only test that can definitively diagnose endometriosis and the only test that can see superficial peritoneal disease. Visual appearance is confirmed by biopsy of representative lesions.
Modern practice follows a "see and treat" approach: at the same surgery that confirms the diagnosis, a trained surgeon excises the implants. This is not a quick look-and-close procedure — it is therapeutic as well as diagnostic. For this reason, the surgeon you choose for your diagnostic laparoscopy should be someone qualified to do the excision. Being diagnosed by a general gynecologist, closed back up, and then referred on means going through two surgeries. See Excision vs Ablation for why the surgeon's technique matters as much as the fact of surgery.
Laparoscopy is not risk-free — it is a general-anesthesia operation with the usual surgical risks — but in experienced hands it is same-day or overnight, and recovery is measured in weeks, not months.
CA-125 — Why It Is Not a Screening Test
CA-125 is a serum protein elevated in about half of moderate-to-severe endometriosis cases — but also in normal menstruation, ovulation, pregnancy, fibroids, PID, and ovarian cancer. Its specificity is too low for screening: a positive does not confirm endometriosis, and a negative does not rule it out. Its proper use is narrow — tracking a known endometrioma or evaluating an ovarian mass for cancer risk. "Your CA-125 is normal so you probably do not have endometriosis" is a wrong statement.
Emerging Biomarkers
Several blood and menstrual-effluent tests are in development and marketed directly to patients. They remain investigational.
- Menstrual effluent cell diagnostics (DotLab and similar) — cells and molecular markers from menstrual blood. Promising; sensitivity and specificity still being established.
- MicroRNA panels — plasma miRNA signatures with reasonable accuracy in research cohorts; commercial versions exist.
- Proteomic panels — combinations of inflammatory markers under study.
A positive emerging biomarker is useful evidence to push for further workup, but cannot replace imaging or laparoscopy. A negative result is not reassurance if symptoms fit.
Scripts for Your Gyn Appointment
Walking into an appointment with specific, unambiguous language changes the conversation. Clinicians hear "painful periods" dozens of times a week. They do not dismiss it on purpose — they triage. You want to land in the high-acuity pile.
Opening lines that work:
- "My pain is a seven out of ten or higher during my period, and pain medication does not touch it."
- "I have tried [ibuprofen 800 mg around the clock / combined oral contraceptives / progestin-only pill] for [X] months with no meaningful improvement."
- "I am missing [X] days of work or school per month because of this pain. That is not sustainable."
- "Pain with intercourse has become a regular problem. So has cyclic bowel pain / urinary pain / pain radiating to my leg or rectum."
- "I want to be evaluated for endometriosis. I would like a pelvic ultrasound and, if that is inconclusive, a referral to a gynecologic surgeon who performs laparoscopic excision of endometriosis."
When a clinician pushes back:
- "Can you document in my chart that you declined to order imaging / refer me, and your reasoning?" — This is your legal right. It almost always changes the answer.
- "What else could explain this symptom pattern? I want to understand why you are ruling endometriosis out."
- "I would like a second opinion. Please provide a referral."
Bring a written symptom log (see section 12). Bring a partner, parent, or friend if that helps. Your request is reasonable and consistent with current guidelines.
Finding an Excision Specialist
The difference between a general gynecologist and a trained endometriosis excision surgeon is enormous — disease recurrence and reoperation rates differ by orders of magnitude. There is no single certifying body that identifies qualified surgeons, so patients have built informal registries.
- Nancy's Nook Endometriosis Education — a private Facebook group that maintains a crowdsourced, vetted list of surgeons. Joining requires answering a short screening. Their list is the single most-used resource in the patient community.
- iCareBetter — a directory where surgeons submit surgical videos for peer review by endometriosis specialists. The vetting is formal, the surgeon list is public.
- AAGL (American Association of Gynecologic Laparoscopists) — maintains a certification in minimally invasive gynecologic surgery. Not endometriosis-specific but a useful starting filter.
- Insurance and travel. Many excision specialists are out-of-network. A "single case agreement" with your insurer can sometimes bring costs down. Travel is common, the cost is real, but so is the difference in outcome.
Symptom Tracking to Build Your Case
A two- or three-cycle journal turns a vague complaint into a data set. Track by date, not by memory:
- Phase of cycle (day 1 = first day of bleeding).
- Pain scale 0–10, at morning, midday, evening.
- Location — pelvic, low back, rectal, leg, shoulder (diaphragmatic endo), chest.
- Bowel symptoms — diarrhea, constipation, pain with bowel movement, rectal bleeding (any blood is a red flag, see section 15).
- Bladder symptoms — urgency, pain with urination, blood in urine (especially if cyclic).
- Sex — pain with deep penetration, pain after.
- Missed work or school days, ER visits, unscheduled urgent-care visits.
- Medications tried and whether they helped.
A phone app works; a paper notebook works. What matters is showing up with dates and numbers. "I had pain" is easy to dismiss. "Pain scored 8/10 on days 24–28 of five consecutive cycles, unresponsive to 800 mg ibuprofen every six hours, causing three ER visits since January" is not.
When to Push Harder
There are moments when the right move is to stop trying to win over the current clinician and start over with a new one:
- Repeat misdiagnoses without resolution. If you have been told "IBS" or "anxiety" by two clinicians and nothing has improved, those labels are not working.
- Dismissive language. "All women have cramps," "you are too young to have real pain," "you just need to relax" — these are signals to move on, not persuade.
- Refusal to order imaging or refer despite a clearly documented failure of first-line therapy.
- No plan for reassessment after empirical treatment — if no one has told you when to come back or what success would look like, you are being managed by inertia.
Second and third opinions are not rude. They are the standard of care for any complex diagnosis. A good gynecologist will welcome a fresh set of eyes on a difficult case.
What to Expect After Diagnosis
Diagnosis is a milestone, not an endpoint. Endometriosis is a chronic illness. Even after successful excision, many patients need ongoing care: hormonal suppression to slow recurrence, pelvic floor physical therapy for the central sensitization untreated pain produces, mental-health support, and sometimes a second surgery years later.
What changes at diagnosis is that you finally have a name, a community, a care team that knows what they are looking at, and a plan. The pain may not disappear in a week, but the gaslighting stops. See Pelvic Floor Therapy and Hormonal Therapy Options for the next stage.
Red Flags for Urgent Workup
Most endometriosis symptoms evolve slowly and can be worked up over weeks. A small set of findings warrants immediate evaluation, not a scheduled appointment weeks out.
- Acute severe pelvic pain different from your usual pattern — could signal endometrioma rupture, ovarian torsion, or ectopic pregnancy. Emergency department.
- Rectal bleeding, especially cyclic — bowel endometriosis invading the mucosa, or a separate GI problem. Either way, needs evaluation this week.
- Cyclic hematuria (blood in urine timed with the period) — classic for bladder endometriosis. Needs urology and imaging.
- New-onset severe dyspareunia after previously tolerable intercourse — new lesion growth, especially in the rectovaginal space.
- Flank pain with decreased urine output — rare but serious; may indicate ureteral obstruction from deep infiltrating disease. Needs urgent imaging.
- Cyclic shoulder pain or shortness of breath — diaphragmatic or thoracic endometriosis. Less common but real.
Key Research Papers
- Agarwal SK, et al. Clinical diagnosis of endometriosis: a call to action. Am J Obstet Gynecol. 2019. (Systematic review of diagnostic delay and empirical diagnosis.)
- Bazot M, Daraï E. Diagnosis of deep endometriosis: clinical examination, ultrasonography, magnetic resonance imaging, and other techniques. Fertil Steril. 2017.
- Chapron C, et al. Oral contraceptives and endometriosis: the past use of oral contraceptives for treating severe primary dysmenorrhea is associated with endometriosis, especially deep infiltrating endometriosis. Hum Reprod. 2011.
- Becker CM, et al. ESHRE guideline: endometriosis. Hum Reprod Open. 2022.
Live PubMed Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on endometriosis diagnosis, imaging, and clinical delay:
- Endometriosis diagnostic delay
- Transvaginal ultrasound for endometriosis
- MRI of deep infiltrating endometriosis
- Laparoscopy and endometriosis diagnosis
- Sliding sign and pouch of Douglas obliteration
- CA-125 and endometriosis screening limits
- Endometriosis microRNA biomarkers
- Endometriosis excision versus ablation outcomes
Connections
- Laparoscopy: Excision vs Ablation
- Hormonal Therapy Options
- Pelvic Floor Therapy and Central Sensitization
- Endometriosis
- Infertility
- Ovarian Cysts
- Endo Belly and Gut Connection
- Fertility and Endometriosis
- Diet and Lifestyle
- Adenomyosis Overlap
- Bladder and Bowel Endometriosis
- Polycystic Ovary Syndrome
- Uterine Fibroids
- Chronic Pain
- Interstitial Cystitis
- Full Body MRI
- Inflammatory Markers
- Irritable Bowel Syndrome