Eating Disorders
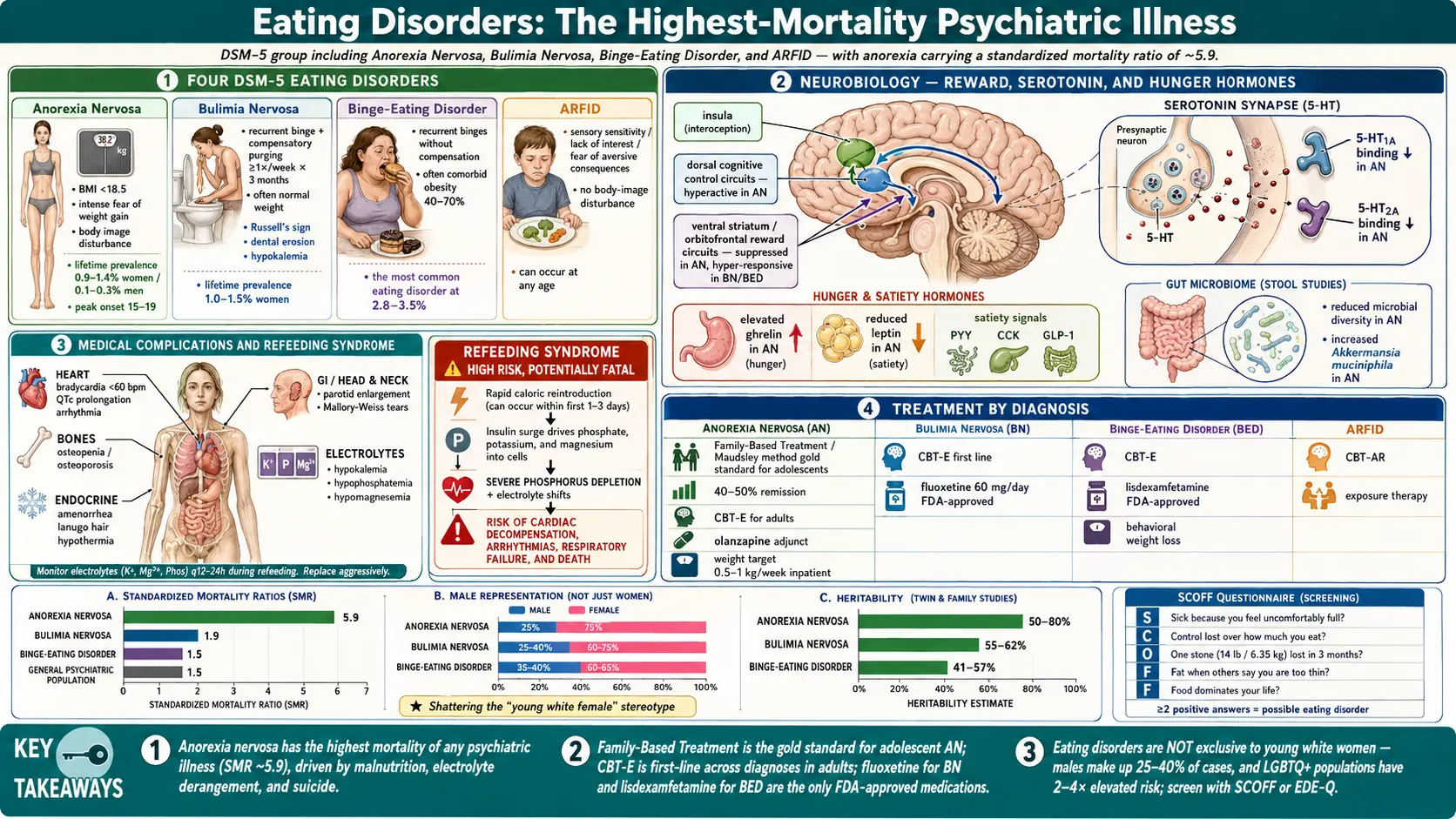
Table of Contents
- Overview
- Epidemiology
- Pathophysiology
- Etiology and Risk Factors
- Clinical Presentation
- Diagnosis
- Treatment
- Complications
- Prognosis
- Prevention
- Recent Research and Advances
- References & Research
- Featured Videos
1. Overview
Eating disorders are a group of serious psychiatric conditions characterized by persistent disturbances in eating behavior and the associated distressing thoughts and emotions. The DSM-5 recognizes several distinct eating disorder diagnoses, the most prominent being Anorexia Nervosa (AN), Bulimia Nervosa (BN), Binge-Eating Disorder (BED), Avoidant/Restrictive Food Intake Disorder (ARFID), Pica, and Rumination Disorder. These conditions involve complex interactions between psychological, biological, and sociocultural factors, resulting in behaviors that severely compromise physical health, psychosocial functioning, and quality of life.
Eating disorders carry the highest mortality rate of any psychiatric illness. Anorexia nervosa has a standardized mortality ratio (SMR) of approximately 5.9, meaning affected individuals are nearly six times more likely to die prematurely compared to the general population. Deaths result from medical complications of malnutrition, purging behaviors, and suicide. Despite their severity, eating disorders remain significantly underdiagnosed and undertreated, with only approximately 20-30% of affected individuals receiving adequate treatment.
The DSM-5 (2013) brought significant changes to eating disorder classification, including the addition of Binge-Eating Disorder as a formal diagnosis (previously in the appendix), the removal of the amenorrhea criterion for anorexia nervosa, the reduction of binge/purge frequency threshold for bulimia nervosa from twice to once per week, and the introduction of ARFID as a new diagnosis replacing the childhood-limited "feeding disorder of infancy and early childhood." These changes improved diagnostic sensitivity and better captured the full spectrum of eating pathology.
2. Epidemiology
Anorexia Nervosa has a lifetime prevalence of approximately 0.9-1.4% in women and 0.1-0.3% in men. Peak age of onset is 15-19 years. AN is more common in industrialized countries and among Caucasian populations, though recent evidence suggests it occurs across all racial and ethnic groups. Incidence has remained relatively stable over the past several decades.
Bulimia Nervosa has a lifetime prevalence of approximately 1.0-1.5% in women and 0.1-0.5% in men. Mean age of onset is 18-21 years. BN incidence peaked in the 1980s-1990s and has subsequently declined in some Western countries, possibly reflecting a shift toward binge-eating disorder diagnoses.
Binge-Eating Disorder is the most common eating disorder, with a lifetime prevalence of approximately 2.8-3.5% in women and 1.0-2.0% in men. The gender ratio is more balanced than for AN or BN. Mean age of onset is 21-25 years, and BED is significantly more prevalent among individuals seeking obesity treatment (30-50%).
Eating disorders are increasingly recognized in males (accounting for approximately 25% of AN cases, 25-40% of BN cases, and 35-40% of BED cases), LGBTQ+ populations (2-4 fold elevated risk), athletes (particularly in aesthetic and weight-class sports), and across all racial and ethnic groups. The misconception that eating disorders primarily affect young, White, affluent women continues to contribute to diagnostic disparities.
3. Pathophysiology
Neurotransmitter Systems
Serotonergic dysfunction plays a central role in eating disorder pathophysiology. Individuals with AN show elevated 5-HT1A receptor binding and reduced 5-HT2A receptor binding in cortical regions, patterns that persist after weight restoration and may represent trait markers. Serotonin dysregulation contributes to the characteristic anxiety, perfectionism, obsessionality, and harm avoidance seen in AN. In BN, altered serotonergic function is linked to impulsivity and impaired satiety signaling. Dopaminergic dysfunction is also implicated, with AN patients showing altered striatal dopamine release contributing to anhedonia, aberrant reward processing, and paradoxical reward from starvation. BED is associated with reduced striatal dopamine D2 receptor availability, resembling patterns seen in substance addiction.
Appetite and Energy Homeostasis
Eating disorders involve profound disruption of the hormonal systems regulating hunger, satiety, and energy balance. In AN, ghrelin (the "hunger hormone") is paradoxically elevated while leptin (the satiety hormone) is markedly reduced, reflecting the body's attempt to counteract energy deficit. Peptide YY, cholecystokinin, and GLP-1 (satiety signals) show variable alterations. These hormonal changes contribute to the peculiar absence of hunger drive in chronic AN despite severe caloric restriction. In BED, impaired postprandial satiety signaling and blunted ghrelin suppression after eating may contribute to binge episodes.
Brain Structure and Function
Neuroimaging reveals characteristic patterns across eating disorders. AN is associated with global gray matter volume reduction (partially reversible with weight restoration), altered insula function (interoceptive processing), and hyperactive dorsal cognitive control circuits with reduced ventral reward circuits, consistent with the ability to override hunger signals. BN and BED show impaired prefrontal inhibitory control and enhanced reward region activation to food cues, particularly in the ventral striatum and orbitofrontal cortex, paralleling neural patterns in addiction. Default mode network alterations across eating disorders correlate with body image disturbance and self-referential processing abnormalities.
Gut Microbiome
Emerging research demonstrates significant gut microbiome alterations in eating disorders. AN patients show reduced microbial diversity, increased representation of mucin-degrading bacteria (e.g., Akkermansia muciniphila), and altered short-chain fatty acid production. These changes may influence mood, appetite regulation, and immune function through the gut-brain axis. Microbiome composition partially normalizes with weight restoration but may not fully recover, potentially contributing to relapse vulnerability.
4. Etiology and Risk Factors
Genetic Factors
- Heritability estimated at 50-80% for AN, 55-62% for BN, and 41-57% for BED
- GWAS studies have identified 8 genome-wide significant loci for AN, including associations near genes involved in metabolism, lipid biology, and physical activity
- AN shows significant positive genetic correlations with OCD, major depression, anxiety, and schizophrenia, and negative genetic correlations with BMI, obesity, and type 2 diabetes — suggesting metabolic factors are intrinsic to the disorder
- First-degree relatives of AN probands have a 10-12 fold increased risk
Psychological Factors
- Perfectionism — one of the most robust personality risk factors, particularly for AN
- Low self-esteem and negative self-evaluation
- Cognitive rigidity and detail-focused processing style (weak central coherence)
- Interoceptive deficits — difficulty identifying and responding to internal body signals
- Emotion regulation difficulties — bingeing and purging often function as maladaptive emotion regulation strategies
- Body dissatisfaction — a consistent and potent risk factor across eating disorders
Sociocultural Factors
- Thin ideal internalization — media-promoted beauty standards emphasizing thinness
- Social media exposure — appearance-focused content, fitspiration, pro-eating disorder communities
- Dieting behavior — restrictive dieting is a significant proximal risk factor for all eating disorders
- Weight stigma and fat phobia — societal discrimination based on body weight
- Athletic and professional pressures — sports emphasizing leanness (gymnastics, ballet, wrestling, distance running)
- Peer influences — weight-related teasing, social comparison, peer dieting behaviors
Trauma and Adversity
- Childhood sexual abuse — associated with approximately 3-fold increased risk of developing an eating disorder
- Physical and emotional abuse
- Bullying, particularly weight-related bullying
- Adverse childhood experiences (ACEs) — dose-response relationship with eating disorder risk
5. Clinical Presentation
Anorexia Nervosa
Restricting type: weight loss achieved primarily through dieting, fasting, and/or excessive exercise. Binge-eating/purging type: recurrent episodes of bingeing and/or purging (self-induced vomiting, laxative misuse). Clinical features include:
- Significantly low body weight (BMI <18.5 kg/m2 in adults; below expected growth trajectory in children/adolescents)
- Intense fear of gaining weight or persistent behavior interfering with weight gain
- Body image disturbance — distorted perception of body size and shape; undue influence of weight on self-evaluation; denial of seriousness of low weight
- Physical signs: lanugo hair, acrocyanosis, bradycardia (heart rate <60 bpm), hypotension, hypothermia, edema, dry skin, hair loss, parotid gland enlargement (in purging subtype)
- Medical consequences: amenorrhea, osteoporosis, cardiac arrhythmias (QTc prolongation), renal impairment, hepatic dysfunction, pancytopenia
Bulimia Nervosa
- Recurrent binge eating episodes — eating an objectively large amount of food with a sense of loss of control, occurring at least once per week for 3 months
- Compensatory behaviors — self-induced vomiting (80-90% of cases), laxative abuse (approximately 60%), diuretic misuse, fasting, excessive exercise
- Self-evaluation unduly influenced by body shape and weight
- Often normal weight or slightly overweight
- Physical signs: Russell's sign (calluses on knuckles from induced vomiting), dental erosion (perimolysis), parotid enlargement (chipmunk facies), Mallory-Weiss tears
- Electrolyte disturbances: hypokalemia (most dangerous), metabolic alkalosis from vomiting, metabolic acidosis from laxative abuse
Binge-Eating Disorder
- Recurrent binge eating episodes (at least once per week for 3 months) characterized by eating rapidly, eating until uncomfortably full, eating large amounts when not hungry, eating alone due to embarrassment, feeling disgusted/depressed/guilty afterward
- Marked distress regarding binge eating
- Absence of regular compensatory behaviors (distinguishing BED from BN)
- Strong association with obesity — approximately 40-70% of BED patients are obese
- Binge episodes are often triggered by negative emotions, interpersonal stress, dietary restriction, or boredom
ARFID (Avoidant/Restrictive Food Intake Disorder)
- Significant failure to meet nutritional needs not explained by lack of food availability, cultural practice, or another medical/psychiatric condition
- No body image disturbance or fear of weight gain (distinguishing from AN)
- Three common presentations: sensory sensitivity (avoidance based on taste, texture, smell), lack of interest in eating, and concern about aversive consequences of eating (choking, vomiting, pain)
- Can occur at any age; increasingly recognized in adults
6. Diagnosis
DSM-5 Diagnostic Criteria for Anorexia Nervosa
- A: Restriction of energy intake relative to requirements, leading to significantly low body weight
- B: Intense fear of gaining weight or becoming fat, or persistent behavior that interferes with weight gain
- C: Disturbance in the way body weight or shape is experienced, undue influence of weight on self-evaluation, or persistent lack of recognition of the seriousness of low body weight
- Subtypes: Restricting type vs. Binge-eating/Purging type
- Severity based on BMI: Mild (≥17), Moderate (16-16.99), Severe (15-15.99), Extreme (<15)
Screening Tools
- SCOFF Questionnaire — 5-item screen (Sick, Control, One stone, Fat, Food); score ≥2 indicates probable eating disorder; sensitivity 78-100%, specificity 72-90%
- Eating Disorder Examination Questionnaire (EDE-Q) — 28-item self-report; global score ≥4.0 suggests clinical significance
- Eating Disorder Examination (EDE) — gold standard semi-structured clinical interview; 36 items across 4 subscales (restraint, eating concern, shape concern, weight concern)
- Eating Attitudes Test (EAT-26) — 26-item self-report; widely used for screening; score ≥20 indicates significant eating pathology
Medical Evaluation
Comprehensive medical assessment is essential and should include:
- Basic metabolic panel — electrolytes (especially potassium, sodium, phosphorus, magnesium), glucose, renal function
- Complete blood count — leukopenia, anemia, thrombocytopenia in severe AN
- Thyroid function tests — sick euthyroid syndrome common in AN
- Electrocardiogram — QTc prolongation, bradycardia, ST-T wave changes
- DEXA scan — bone mineral density assessment (osteopenia/osteoporosis in AN)
- Liver function tests, amylase/lipase, phosphorus levels
7. Treatment
Treatment of Anorexia Nervosa
Nutritional rehabilitation and weight restoration are the foundation of AN treatment. Target weight gain of 0.5-1.0 kg/week for inpatient and 0.25-0.5 kg/week for outpatient settings. Monitoring for refeeding syndrome is critical during early weight restoration — characterized by hypophosphatemia, hypokalemia, hypomagnesemia, fluid shifts, and cardiac complications. Phosphorus supplementation is routinely provided.
Psychotherapy for AN:
- Family-Based Treatment (FBT / Maudsley method) — gold standard for adolescent AN; parents take temporary charge of their child's eating; typically 15-20 sessions over 12 months; remission rates of 40-50% at end of treatment
- Cognitive Behavioral Therapy for Eating Disorders (CBT-E) — enhanced transdiagnostic CBT; 40 sessions for underweight patients; addresses overvaluation of shape/weight, dietary restraint, and maintaining mechanisms
- Specialist Supportive Clinical Management (SSCM) — combines clinical management (nutritional counseling, weight monitoring) with supportive psychotherapy
- Maudsley Model of Anorexia Nervosa Treatment for Adults (MANTRA) — addresses cognitive-interpersonal maintaining factors including cognitive rigidity, emotional avoidance, and pro-anorexia beliefs
Pharmacotherapy for AN: No medication has demonstrated robust efficacy for the core symptoms of AN or weight restoration. Olanzapine (2.5-10 mg/day) has modest evidence for weight gain and anxiety reduction. SSRIs are generally ineffective during the underweight state (likely due to tryptophan depletion) but may help prevent relapse after weight restoration. Fluoxetine (20-60 mg/day) has limited evidence for relapse prevention post-weight restoration.
Treatment of Bulimia Nervosa
- CBT for Bulimia Nervosa (CBT-BN) — first-line treatment; typically 16-20 sessions; achieves abstinence from bingeing/purging in 30-50% of patients; addresses dietary restraint, body image disturbance, and triggers
- Interpersonal Psychotherapy (IPT) — comparable long-term efficacy to CBT though slower onset of action
- Fluoxetine (Prozac) 60 mg/day — the only FDA-approved medication for BN; reduces binge/purge frequency by approximately 50-70%; often combined with CBT for optimal results
- Topiramate (25-400 mg/day) — reduces binge frequency and promotes weight loss; useful when comorbid obesity is present
Treatment of Binge-Eating Disorder
- CBT (individual or group) — first-line psychotherapy; reduces binge frequency but may not produce significant weight loss
- Lisdexamfetamine (Vyvanse) 50-70 mg/day — FDA-approved for moderate-to-severe BED; reduces binge days per week by approximately 3-4 days versus placebo; the only medication with FDA approval specifically for BED
- Topiramate (25-400 mg/day) — reduces binge frequency and body weight; significant side effect burden limits use
- SSRIs — moderate efficacy for binge reduction (fluoxetine, sertraline, fluvoxamine at standard antidepressant doses)
- Behavioral weight loss (BWL) — addresses comorbid obesity; comparable binge reduction to CBT in some studies
Levels of Care
- Outpatient — appropriate for medically stable patients with adequate motivation
- Intensive outpatient (IOP) — 3-5 days/week, 3-4 hours/day
- Partial hospitalization (PHP) — 5 days/week, 6-10 hours/day with supervised meals
- Residential treatment — 24-hour care in a non-hospital setting; typically 30-90 days
- Inpatient medical/psychiatric hospitalization — for acute medical instability (heart rate <40 bpm, blood pressure <90/60, temperature <36C, severe electrolyte abnormalities, suicidality)
8. Complications
- Cardiac complications — bradycardia, QTc prolongation, mitral valve prolapse, pericardial effusion, congestive heart failure (during refeeding), sudden cardiac death
- Electrolyte abnormalities — hypokalemia (risk of fatal cardiac arrhythmia), hypophosphatemia (refeeding syndrome), hyponatremia, hypomagnesemia
- Endocrine disruption — hypothalamic amenorrhea, low estrogen/testosterone, hypothyroidism (sick euthyroid), elevated cortisol, growth hormone resistance
- Skeletal complications — osteopenia and osteoporosis (affecting up to 85% of AN patients); increased fracture risk; may be irreversible even after weight restoration
- Gastrointestinal — delayed gastric emptying, constipation, superior mesenteric artery syndrome, esophageal tears (Mallory-Weiss), Barrett's esophagus, pancreatitis
- Dental — perimolysis (enamel erosion from repeated vomiting), dental caries, parotid gland hypertrophy
- Neurological — cerebral atrophy (partially reversible), peripheral neuropathy, seizures (electrolyte-related)
- Renal — chronic dehydration, hypokalemic nephropathy, renal failure
- Hematological — pancytopenia, immunosuppression, impaired wound healing
- Psychiatric — major depression, anxiety disorders, substance use disorders, self-harm, suicide (AN has the highest suicide rate of any psychiatric disorder after adjusting for mortality)
- Fertility and pregnancy — infertility, increased risk of miscarriage, low birth weight infants, postpartum depression
9. Prognosis
Anorexia Nervosa: Long-term outcome studies (10-20 year follow-up) indicate that approximately 46% of patients achieve full recovery, 33% show improvement but remain symptomatic, and 21% develop a chronic course. The crude mortality rate is approximately 5-6% per decade of illness, with deaths due to medical complications (approximately 50%), suicide (approximately 25-30%), and other causes. The standardized mortality ratio of 5.9 is the highest of any psychiatric disorder. Median time to recovery is approximately 7 years. Predictors of better outcome include younger age at onset, shorter duration of illness, and higher BMI at presentation. Onset after age 25 and very low BMI at presentation predict poorer outcomes.
Bulimia Nervosa: Approximately 55-70% of patients achieve full or partial remission over 5-10 years. The crude mortality rate is approximately 2% per decade. Crossover to AN occurs in approximately 10-15% of cases. Early treatment response (within the first 4-6 weeks of CBT) is a strong predictor of eventual outcome.
Binge-Eating Disorder: BED has the most favorable prognosis among eating disorders, with remission rates of approximately 50-80% over 4-5 years. However, weight management remains a significant challenge, and many patients continue to struggle with obesity-related medical complications even after binge cessation.
10. Prevention
- Media literacy programs — teaching critical evaluation of appearance-focused media messages; programs like Media Smart and Body Project have demonstrated efficacy in reducing eating disorder risk factors
- The Body Project (dissonance-based prevention) — participants critique the thin ideal through verbal, written, and behavioral exercises; reduces eating disorder onset by 60% over 3-year follow-up in randomized trials
- School-based prevention programs — targeting body image, self-esteem, and healthy eating behaviors; most effective when interactive and delivered over multiple sessions
- Screening in high-risk populations — athletes, dancers, models, military personnel, individuals with type 1 diabetes
- Anti-weight stigma initiatives — reducing weight-based discrimination and bullying in schools and workplaces
- Social media regulation — age-appropriate content filters, warning labels on digitally altered images, bans on pro-eating disorder content
- Training healthcare providers — improving early detection in primary care, pediatrics, and dental settings
- Family-based approaches — positive family meal environments, avoiding diet talk and weight commentary, modeling healthy relationships with food
- Addressing dieting culture — promoting Health at Every Size (HAES) and intuitive eating principles
11. Recent Research and Advances
Genomic and metabolomic discoveries have fundamentally reframed our understanding of anorexia nervosa. The Eating Disorders Working Group of the Psychiatric Genomics Consortium published landmark GWAS findings demonstrating that AN has significant metabo-psychiatric underpinnings — genetic risk factors overlap with metabolic traits (low BMI, low insulin resistance) in addition to psychiatric disorders. This suggests AN should be reconceptualized as a metabo-psychiatric disorder rather than a purely psychological condition, with implications for treatment development targeting metabolic pathways.
Psilocybin-assisted therapy is being investigated for AN in Phase II trials, with the rationale that psychedelic-induced cognitive flexibility and emotional processing may help overcome the rigid thinking patterns characteristic of AN. Preliminary results from open-label studies suggest improvements in eating disorder psychopathology and psychological well-being following psilocybin sessions combined with psychotherapy.
Gut microbiome-targeted interventions represent a novel treatment frontier. Fecal microbiota transplantation (FMT) is being studied in clinical trials for AN, with the hypothesis that restoring healthy gut microbial communities may improve appetite regulation, reduce gastrointestinal symptoms, and modulate brain function through the gut-brain axis. Probiotic supplementation trials are also underway.
Digital interventions are expanding treatment access. Internet-based CBT programs (such as Overcoming Bulimia Online and Recovery Record) have shown efficacy comparable to guided self-help in reducing binge/purge symptoms. AI-powered chatbots for eating disorder support (such as Woebot) are being evaluated in clinical trials. Smartphone-based ecological momentary interventions deliver personalized support at moments of vulnerability identified through real-time symptom monitoring.
Neuroimaging-guided treatments are advancing toward precision medicine. Real-time fMRI neurofeedback training patients to modulate activation in brain regions involved in self-referential processing and body image has shown promising preliminary results in AN. Repetitive TMS targeting the left dorsolateral prefrontal cortex has demonstrated efficacy in reducing binge eating in BN and BED in multiple randomized controlled trials.
12. Research Papers
Historical Background
The earliest medical descriptions of self-starvation date to the medieval period, with accounts of "holy fasting" among female saints. Richard Morton provided the first medical case report of anorexia nervosa in 1689, describing a patient with "nervous consumption." The condition was independently described and named by Sir William Gull in London ("anorexia nervosa," 1873) and Charles Lasegue in Paris ("anorexie hysterique," 1873). Gerald Russell defined bulimia nervosa as a distinct syndrome in his landmark 1979 paper, describing an "ominous variant of anorexia nervosa." Binge-Eating Disorder was first described by Albert Stunkard in 1959 as "night eating syndrome" and later refined. Hilde Bruch's influential 1973 book Eating Disorders: Obesity, Anorexia Nervosa, and the Person Within transformed clinical understanding by emphasizing body image disturbance and deficits in interoceptive awareness as core psychopathology.
Key Research Papers
- Arcelus J, Mitchell AJ, Wales J, Nielsen S. Mortality rates in patients with anorexia nervosa and other eating disorders: a meta-analysis of 36 studies. Arch Gen Psychiatry. 2011;68(7):724-731.
- Watson HJ, Yilmaz Z, Thornton LM, et al. Genome-wide association study identifies eight risk loci and implicates metabo-psychiatric origins for anorexia nervosa. Nat Genet. 2019;51(8):1207-1214.
- Fairburn CG, Cooper Z, Doll HA, et al. Transdiagnostic cognitive-behavioral therapy for patients with eating disorders: a two-site trial with 60-week follow-up. Am J Psychiatry. 2009;166(3):311-319.
- Lock J, Le Grange D, Agras WS, et al. Randomized clinical trial comparing family-based treatment with adolescent-focused individual therapy for adolescents with anorexia nervosa. Arch Gen Psychiatry. 2010;67(10):1025-1032.
- Kessler RC, Berglund PA, Chiu WT, et al. The prevalence and correlates of binge eating disorder in the World Health Organization World Mental Health Surveys. Biol Psychiatry. 2013;73(9):904-914.
- Russell G. Bulimia nervosa: an ominous variant of anorexia nervosa. Psychol Med. 1979;9(3):429-448.
- McElroy SL, Hudson JI, Mitchell JE, et al. Efficacy and safety of lisdexamfetamine for treatment of adults with moderate to severe binge-eating disorder: a randomized clinical trial. JAMA Psychiatry. 2015;72(3):235-246.
- Zipfel S, Giel KE, Bulik CM, et al. Anorexia nervosa: aetiology, assessment, and treatment. Lancet Psychiatry. 2015;2(12):1099-1111.
- Steinglass J, Foerde K, Kostro K, et al. Restrictive food intake as a choice — a paradigm for study. Int J Eat Disord. 2015;48(1):59-66.
- Frank GKW, Shott ME, DeGuzman MC. The neurobiology of eating disorders. Child Adolesc Psychiatr Clin N Am. 2019;28(4):629-640.
- Treasure J, Duarte TA, Schmidt U. Eating disorders. Lancet. 2020;395(10227):899-911.
- Stice E, Marti CN, Spoor S, et al. Dissonance and healthy weight eating disorder prevention programs: long-term effects from a randomized efficacy trial. J Consult Clin Psychol. 2008;76(2):329-340.
- Mack I, Cuntz U, Gramer C, et al. Weight gain in anorexia nervosa does not ameliorate the faecal microbiota, branched chain fatty acid profiles, and gastrointestinal complaints. Sci Rep. 2016;6:26752.
- Bulik CM, Sullivan PF, Tozzi F, et al. Prevalence, heritability, and prospective risk factors for anorexia nervosa. Arch Gen Psychiatry. 2006;63(3):305-312.
PubMed Topic Searches
- PubMed: anorexia nervosa treatment
- PubMed: bulimia nervosa CBT
- PubMed: binge eating disorder
- PubMed: eating disorder family based therapy
- PubMed: eating disorder epidemiology
- PubMed: eating disorder mortality
- PubMed: refeeding syndrome
- PubMed: eating disorder genetics
- PubMed: ARFID avoidant restrictive
- PubMed: eating disorder gut microbiome
- PubMed: eating disorder adolescents
- PubMed: eating disorder comorbidity
Connections
- Hunger, Leptin & Why Diets Fight Back — interactive animation
- Anxiety
- Depression
- OCD
- Obesity
- Magnesium
- Zinc
- Iron
- Vitamin B12
- Vitamin D3
- Stress Management
- Loss of Appetite
- Gut Microbiome
- Gut-Brain Axis
- Tryptophan
- Fasting
- Osteoporosis
- Pellagra and Niacin Deficiency