Obsessive-Compulsive Disorder (OCD)
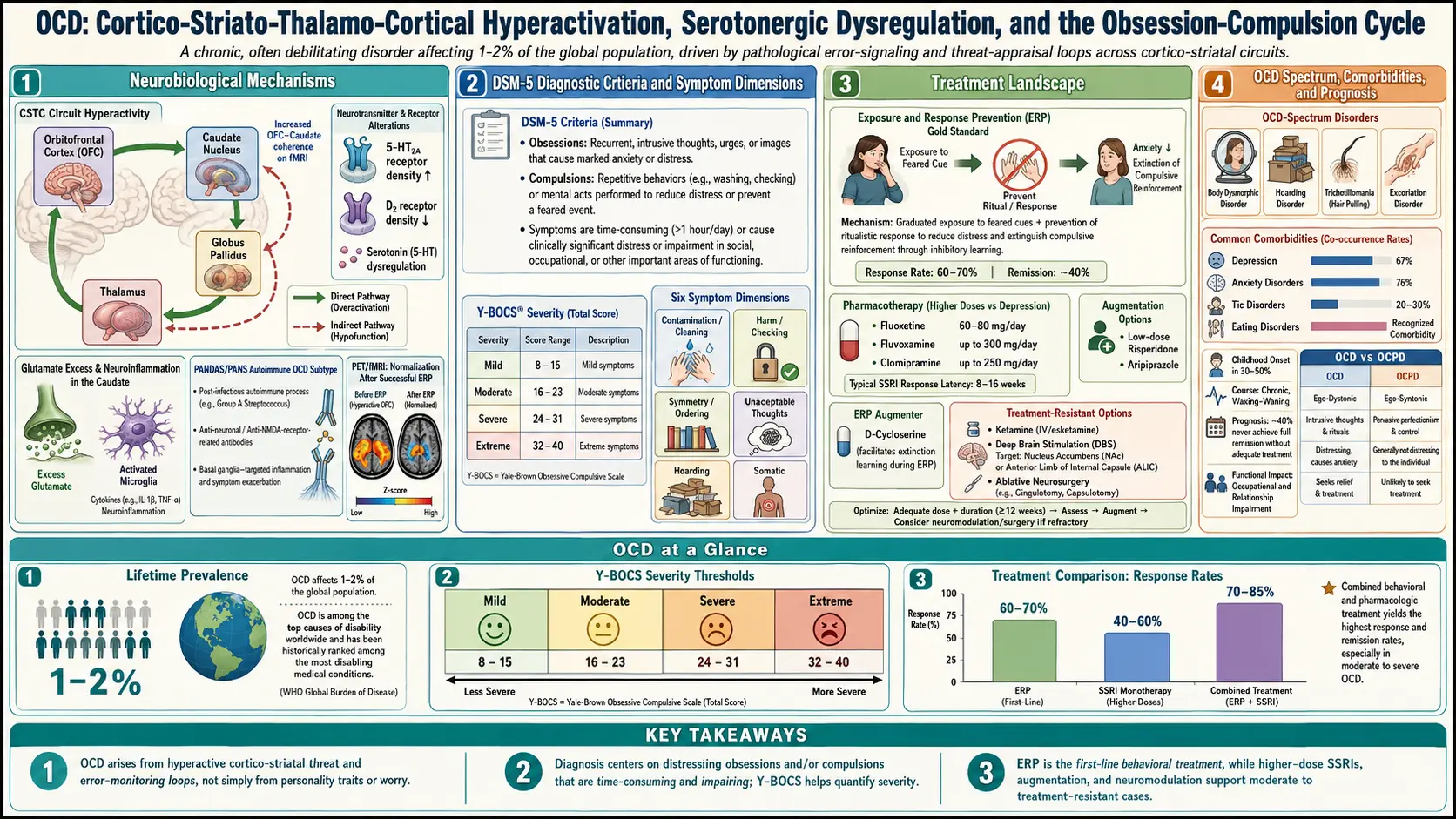
Table of Contents
- Overview
- Epidemiology
- Pathophysiology
- Etiology and Risk Factors
- Clinical Presentation
- Diagnosis
- Treatment
- Complications
- Prognosis
- Prevention
- Recent Research and Advances
- References & Research
- Featured Videos
1. Overview
Obsessive-Compulsive Disorder (OCD) is a chronic neuropsychiatric disorder characterized by the presence of obsessions (recurrent, intrusive, and unwanted thoughts, images, or urges that cause marked anxiety or distress) and/or compulsions (repetitive behaviors or mental acts that the individual feels driven to perform in response to an obsession or according to rigid rules). OCD was reclassified in the DSM-5 (2013) from the anxiety disorders category into its own chapter, Obsessive-Compulsive and Related Disorders, reflecting its distinct neurobiological profile and clinical phenomenology.
OCD is recognized by the World Health Organization as one of the top 10 most disabling illnesses worldwide in terms of lost income and diminished quality of life. The disorder typically follows a waxing and waning course, with symptom severity fluctuating in response to stress, life changes, and other factors. OCD symptoms are ego-dystonic, meaning patients generally recognize that their obsessions are irrational or excessive, although insight varies considerably and the DSM-5 includes specifiers for good or fair insight, poor insight, and absent insight/delusional beliefs.
The disorder is closely related to several conditions now grouped in the OCD spectrum, including body dysmorphic disorder, hoarding disorder, trichotillomania (hair-pulling disorder), and excoriation (skin-picking) disorder. OCD also has significant overlap with tic disorders, and a tic-related specifier is included in the DSM-5. Understanding OCD as a disorder of the cortico-striato-thalamo-cortical (CSTC) circuit has been one of the most successful examples of translational neuroscience in psychiatry.
2. Epidemiology
OCD has a lifetime prevalence of approximately 2.0-3.0% globally, making it one of the most common psychiatric disorders. The 12-month prevalence in the United States is approximately 1.0-1.2%. OCD affects males and females approximately equally in adulthood, though males predominate in childhood-onset cases (2:1 male-to-female ratio for onset before age 10). The mean age of onset is 19.5 years, with approximately 25% of cases beginning by age 14. There is a bimodal distribution of onset, with peaks in pre-adolescence (ages 10-12) and early adulthood (ages 20-22).
The average delay from symptom onset to diagnosis and treatment is disturbingly long, estimated at 7-10 years in most studies. This treatment gap is attributed to shame, poor recognition, and the secretive nature of many obsessions. OCD has been identified across all cultures studied, though symptom content varies culturally — religious obsessions are more common in highly religious societies, while contamination fears show relative consistency across cultures.
Comorbidity rates are high: 76% of OCD patients have at least one comorbid psychiatric disorder. The most common comorbidities include major depressive disorder (63%), anxiety disorders (76%), tic disorders (30% in childhood-onset cases), and ADHD. Approximately 25-30% of individuals with Tourette syndrome also meet criteria for OCD.
3. Pathophysiology
Cortico-Striato-Thalamo-Cortical (CSTC) Circuit
The most well-established neurobiological model of OCD involves dysfunction in the CSTC circuit, a series of parallel loops connecting cortical regions to the basal ganglia and thalamus. In OCD, there is hyperactivity in the "direct" (excitatory) pathway through the basal ganglia, which normally facilitates cortical activation, and relative underactivity of the "indirect" (inhibitory) pathway, which normally suppresses unwanted motor and cognitive programs. This imbalance results in a failure to inhibit intrusive thoughts and repetitive behaviors. Neuroimaging studies consistently demonstrate hyperactivation of the orbitofrontal cortex (OFC), anterior cingulate cortex (ACC), and caudate nucleus at rest and during symptom provocation, with normalization following successful treatment.
Serotonergic System
The serotonin hypothesis of OCD is supported by the selective efficacy of serotonin reuptake inhibitors (SRIs) in treating OCD, while noradrenergic reuptake inhibitors are generally ineffective. Evidence includes altered serotonin transporter (SERT) binding in the midbrain and thalamus, abnormal responses to serotonergic challenge agents (such as m-chlorophenylpiperazine, which exacerbates OCD symptoms), and genetic associations with serotonin system genes. However, the serotonin hypothesis alone is insufficient, as SRIs produce only partial response in many patients.
Glutamatergic and Dopaminergic Systems
Glutamate, the primary excitatory neurotransmitter, has emerged as a critical player in OCD neurobiology. Elevated glutamate levels have been detected in the caudate nucleus and orbitofrontal cortex of OCD patients using magnetic resonance spectroscopy. Glutamatergic hyperactivity in cortico-striatal projections may drive the circuit hyperactivation observed in OCD. The dopaminergic system is particularly relevant in OCD with comorbid tics, where dopamine D2 receptor blockade with antipsychotics can augment SRI response. Altered dopamine transporter and D2 receptor binding has been demonstrated in the basal ganglia of OCD patients.
Immune and Inflammatory Mechanisms
Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal infections (PANDAS) and the broader concept of Pediatric Acute-onset Neuropsychiatric Syndrome (PANS) represent an immune-mediated subtype of OCD. In this model, molecular mimicry between streptococcal antigens and basal ganglia proteins triggers autoimmune inflammation, producing acute-onset OCD and/or tic symptoms. Elevated anti-basal ganglia antibodies, pro-inflammatory cytokines, and microglial activation have been observed in broader OCD populations, suggesting immune dysregulation may contribute beyond the PANDAS subtype.
4. Etiology and Risk Factors
Genetic Factors
- Heritability estimated at 40-65% from twin studies, higher for childhood-onset OCD
- First-degree relatives of OCD patients have a 4-8 fold increased risk
- Candidate genes: SLC6A4 (serotonin transporter), SLC1A1 (glutamate transporter), DLGAP1, PTPRD, and GRIK2 (glutamate receptor)
- Genome-wide association studies (GWAS) have identified common variants of small effect, with polygenic architecture similar to other psychiatric disorders
Neuroanatomical Factors
- Reduced gray matter volume in the orbitofrontal cortex, anterior cingulate cortex, and caudate
- White matter abnormalities in the cingulum bundle and corpus callosum
- Increased caudate volume in pediatric OCD, potentially normalizing with treatment
Environmental Factors
- Perinatal complications — birth trauma, prematurity, and maternal stress during pregnancy
- Childhood trauma — physical and sexual abuse, emotional neglect
- Streptococcal infections — PANDAS/PANS mechanism for acute-onset OCD
- Stressful life events — often precipitate onset or exacerbations in predisposed individuals
- Cognitive style — inflated sense of responsibility, overestimation of threat, perfectionism, intolerance of uncertainty
Developmental Factors
- Early-onset OCD (before age 10) is more familial, more prevalent in males, more commonly associated with tics, and often has a different treatment response profile
- Postpartum onset — OCD can emerge or dramatically worsen in the peripartum period, with obsessions typically centered on harm to the infant
5. Clinical Presentation
Common Obsession Themes
- Contamination — fear of dirt, germs, bodily fluids, environmental toxins, or illness (approximately 50% of patients)
- Harm — intrusive images or thoughts of harming oneself or others (stabbing, pushing someone into traffic)
- Symmetry and exactness — need for things to be arranged, aligned, or balanced in a particular way
- Forbidden or taboo thoughts — unwanted sexual, religious, or violent intrusions (pedophilic OCD, scrupulosity)
- Doubt — persistent uncertainty about whether one has completed an action correctly (locked the door, turned off the stove)
- Somatic obsessions — excessive preoccupation with bodily functions (breathing, swallowing, heartbeat)
Common Compulsion Types
- Washing and cleaning — excessive handwashing, showering, cleaning rituals (often causing dermatitis)
- Checking — repeated verification of locks, appliances, safety measures
- Ordering and arranging — symmetrical arrangement of objects, counting, repeating actions a specific number of times
- Mental compulsions — silent counting, praying, mentally reviewing events, thought neutralization
- Reassurance seeking — repeatedly asking others for confirmation of safety or correctness
- Avoidance — avoiding triggers (knives, bridges, children) — considered a compulsive behavior in OCD
Symptom Dimensions
Factor analytic studies consistently identify four major symptom dimensions that tend to cluster together and may have distinct neurobiological underpinnings:
- Contamination/washing
- Symmetry/ordering/counting/repeating
- Forbidden thoughts (aggressive, sexual, religious)
- Hoarding (now a separate disorder in DSM-5 but still commonly co-occurs)
Insight Variability
The DSM-5 includes an insight specifier recognizing that OCD exists on a continuum of insight. Approximately 4% of OCD patients have absent insight/delusional beliefs about their obsessions, presenting diagnostic challenges and overlap with psychotic disorders. Poor insight is associated with worse treatment outcomes and higher rates of comorbidity.
6. Diagnosis
DSM-5 Diagnostic Criteria
- Criterion A: Presence of obsessions, compulsions, or both
- Criterion B: The obsessions or compulsions are time-consuming (e.g., take more than 1 hour per day) or cause clinically significant distress or impairment in social, occupational, or other important areas of functioning
- Criterion C: Symptoms are not attributable to the physiological effects of a substance or another medical condition
- Criterion D: Symptoms are not better explained by another mental disorder
Specifiers: tic-related; insight level (good/fair, poor, absent/delusional)
Clinical Assessment Tools
- Yale-Brown Obsessive Compulsive Scale (Y-BOCS) — gold standard clinician-administered rating; 10 items scored 0-4 each; total score range 0-40; severity categories: mild (8-15), moderate (16-23), severe (24-31), extreme (32-40)
- Y-BOCS-II — updated version with improved severity ratings and avoidance assessment
- Obsessive-Compulsive Inventory-Revised (OCI-R) — 18-item self-report; cutoff score of 21 suggests clinical OCD
- Dimensional Obsessive-Compulsive Scale (DOCS) — 20-item self-report measuring four symptom dimensions
- Children's Yale-Brown Obsessive Compulsive Scale (CY-BOCS) — for pediatric assessment
Differential Diagnosis
OCD must be differentiated from generalized anxiety disorder (worry about real-life concerns rather than ego-dystonic intrusions), body dysmorphic disorder (preoccupation limited to perceived appearance flaws), hoarding disorder, illness anxiety disorder, obsessive-compulsive personality disorder (ego-syntonic traits rather than ego-dystonic symptoms), tic disorders, psychotic disorders (particularly in patients with poor insight), autism spectrum disorder (restricted interests and repetitive behaviors), and eating disorders (food-related rituals).
7. Treatment
First-Line Psychotherapy: Exposure and Response Prevention (ERP)
Exposure and Response Prevention (ERP) is the gold standard psychotherapy for OCD and is effective in approximately 60-70% of patients who complete treatment. ERP involves systematic, graduated exposure to feared obsessional triggers while voluntarily refraining from compulsive rituals. Treatment typically consists of 13-20 sessions over 3-5 months. Mean Y-BOCS reductions of 10-15 points (approximately 50-60% symptom reduction) are typical. ERP can be delivered individually, in group format, or via intensive (daily) programs for severe cases. Key elements include:
- Hierarchy development — constructing a ranked list of feared situations (SUDS ratings 0-100)
- In vivo exposure — direct confrontation with feared stimuli
- Imaginal exposure — for obsessions that cannot be directly confronted (e.g., harm thoughts)
- Ritual prevention — voluntary abstention from compulsive behaviors during and after exposures
Other Evidence-Based Psychotherapies
- Acceptance and Commitment Therapy (ACT) — emphasis on psychological flexibility, acceptance of intrusive thoughts, and values-based action
- Inference-Based CBT (I-CBT) — targets the reasoning process underlying obsessional doubts rather than the content of obsessions; emerging evidence suggests comparable efficacy to ERP
- Metacognitive therapy — addresses beliefs about thinking (e.g., thought-action fusion, importance of controlling thoughts)
Pharmacotherapy
First-line: Serotonin Reuptake Inhibitors (SRIs)
- Fluvoxamine (Luvox) — 100-300 mg/day; FDA-approved for OCD
- Fluoxetine (Prozac) — 40-80 mg/day; FDA-approved for OCD (note: higher doses than for depression)
- Sertraline (Zoloft) — 50-200 mg/day; FDA-approved for OCD
- Paroxetine (Paxil) — 40-60 mg/day; FDA-approved for OCD
- Clomipramine (Anafranil) — tricyclic SRI; 100-250 mg/day; FDA-approved; often the most potent SRI for OCD but with greater side effect burden (anticholinergic effects, seizure risk at high doses, cardiac conduction changes)
Key pharmacotherapy principles for OCD:
- OCD requires higher SSRI doses than depression (e.g., fluoxetine 60-80 mg versus 20 mg for depression)
- Longer trial duration required: minimum 8-12 weeks at adequate dose before judging response (versus 4-6 weeks for depression)
- Response rates to first SSRI trial: approximately 40-60% (defined as ≥25-35% Y-BOCS reduction)
Augmentation strategies for SRI partial responders:
- Low-dose antipsychotic augmentation — risperidone (0.5-2 mg/day), aripiprazole (2-15 mg/day), or haloperidol; most evidence for tic-related OCD
- Glutamate modulators — memantine (5-20 mg/day), N-acetylcysteine (2400-3000 mg/day); emerging evidence
- Combination SRI + ERP — combining medication with psychotherapy generally produces better outcomes than either alone
Neurosurgical and Neuromodulation Treatments
- Deep Brain Stimulation (DBS) — FDA-approved under Humanitarian Device Exemption for treatment-refractory OCD; targets the ventral capsule/ventral striatum (VC/VS) or subthalamic nucleus; response rates approximately 50-60%
- Transcranial Magnetic Stimulation (TMS) — FDA-cleared for OCD (2018); deep TMS targeting the medial prefrontal cortex and anterior cingulate; response rates approximately 38%
- Anterior capsulotomy and cingulotomy — ablative neurosurgery reserved for the most severe, treatment-refractory cases after exhaustive pharmacological and psychotherapeutic trials
8. Complications
- Severe functional impairment — some patients spend 8+ hours per day on rituals, rendering work and social functioning impossible
- Major depressive disorder — comorbid in approximately 63% of OCD patients; often secondary to the burden of OCD symptoms
- Suicidality — suicide attempt rates of 10-15%; suicidal ideation in up to 50% of OCD patients, particularly those with unacceptable/taboo obsessions
- Dermatological damage — contact dermatitis, eczema, and skin breakdown from excessive washing and cleaning compulsions
- Social isolation — shame and secrecy about symptoms lead to avoidance of relationships and social situations
- Academic and occupational failure — concentration difficulties, time consumed by rituals, avoidance behaviors
- Substance use disorders — self-medication with alcohol, cannabis, or benzodiazepines
- Family burden — family accommodation (modifying routines to accommodate OCD) occurs in 60-97% of families and paradoxically maintains symptoms
- Financial costs — estimated annual healthcare costs 2-3 times higher than general population
9. Prognosis
OCD is generally a chronic condition with a waxing and waning course. Without treatment, spontaneous remission rates are low, with only approximately 20% of untreated patients experiencing full remission over 40 years of follow-up. Among those receiving adequate treatment, the trajectory is more favorable: approximately 60-70% of patients show clinically meaningful response to first-line treatments (ERP and/or SRIs), though full remission is achieved in only approximately 25-30% of treated patients.
Predictors of better outcome include shorter duration of untreated illness, good insight, absence of comorbid depression or personality disorders, predominantly compulsive symptoms (rather than predominantly obsessional), and availability of family support without excessive accommodation. Predictors of poorer outcome include childhood onset with tics, hoarding symptoms, poor insight, severe comorbid depression, and high family accommodation.
Long-term studies suggest that treatment-refractory OCD (failure to respond to multiple adequate SRI trials plus ERP) affects approximately 10-15% of patients. For these individuals, neuromodulation and neurosurgical options (DBS, TMS, capsulotomy) offer additional avenues of treatment with meaningful response rates. Importantly, maintenance treatment with SRIs is generally recommended for 1-2 years minimum after acute response, with high relapse rates (approximately 50-90%) observed upon medication discontinuation.
10. Prevention
- Early identification and intervention — reducing the diagnostic delay (currently averaging 7-10 years) through public education, school-based screening, and primary care clinician training
- Addressing subclinical obsessive-compulsive symptoms — cognitive-behavioral strategies for individuals with elevated but subthreshold symptoms may prevent progression to full OCD
- Prompt treatment of streptococcal infections in children with sudden-onset OCD or tic symptoms (PANDAS/PANS evaluation)
- Postpartum screening — monitoring for OCD onset in the peripartum period, particularly in women with personal or family history
- Family psychoeducation — educating families about accommodation behaviors and their role in maintaining OCD symptoms
- Stress management and resilience building — stress reduction techniques for at-risk individuals with family histories or subclinical symptoms
- Relapse prevention — booster ERP sessions and maintenance pharmacotherapy to prevent symptom recurrence after initial treatment response
- Anti-stigma campaigns — reducing shame and misconceptions about OCD to encourage earlier help-seeking
11. Recent Research and Advances
Psilocybin-assisted therapy for OCD has generated significant interest based on early clinical data. A pilot study at Yale University demonstrated rapid and substantial Y-BOCS reductions following psilocybin administration, with effects potentially mediated through 5-HT2A receptor agonism and disruption of rigid, repetitive thought patterns. Phase II trials are underway as of 2025-2026, exploring both single-dose and repeated-dose protocols in treatment-resistant OCD.
Glutamate-targeted therapies represent a major new pharmacological direction. Troriluzole (a prodrug of riluzole, a glutamate-modulating agent) showed promise in Phase II/III trials for OCD augmentation. Rapastinel and other NMDA receptor modulators are being investigated for their ability to enhance extinction learning during ERP. Ketamine has shown rapid but transient anti-obsessional effects in small studies, with intravenous infusions producing rapid Y-BOCS reductions within hours.
Digital and technology-enhanced treatments are expanding access to ERP. Smartphone-based ERP delivery platforms (such as NOCD and GGtude) have demonstrated non-inferiority to in-person treatment in preliminary trials. Virtual reality exposure therapy (VRET) for contamination-type OCD is under active investigation. Machine learning algorithms analyzing behavioral data from smartphone sensors may enable real-time symptom monitoring and intervention delivery.
Transcranial magnetic stimulation (TMS) protocols continue to evolve, with accelerated (multiple sessions per day) and theta-burst stimulation paradigms showing enhanced efficacy and reduced treatment duration compared to standard protocols. Personalized targeting using neuroimaging-guided coil placement based on individual functional connectivity maps is an emerging approach.
Immunological research is clarifying the role of neuroinflammation in OCD beyond PANDAS. Studies using PET imaging with TSPO radioligands have demonstrated elevated microglial activation in the CSTC circuit of adult OCD patients, opening the possibility of anti-inflammatory treatment strategies including minocycline and celecoxib as adjunctive agents.
12. Research Papers
Historical Background
Obsessive-compulsive phenomena were recognized as early as the 17th century, with descriptions by Robert Burton in The Anatomy of Melancholy (1621) of individuals plagued by intrusive blasphemous thoughts. The French psychiatrist Jean-Etienne Dominique Esquirol provided detailed clinical descriptions of obsessional illness in the 1830s, terming it "monomanie raisonnante." Karl Westphal coined the German term "Zwangsvorstellung" (obsessional idea) in 1877, and the concept of "obsessional neurosis" was elaborated by Sigmund Freud in his famous "Rat Man" case (1909). The behavioral conceptualization by Victor Meyer at the Maudsley Hospital in 1966, who introduced exposure with response prevention, revolutionized OCD treatment. Judith Rapoport's 1989 book The Boy Who Couldn't Stop Washing brought public attention to OCD, and neuroimaging studies by Lewis Baxter and colleagues in the late 1980s established the CSTC circuit model.
Key Research Papers
- Ruscio AM, Stein DJ, Chiu WT, Kessler RC. The epidemiology of obsessive-compulsive disorder in the National Comorbidity Survey Replication. Mol Psychiatry. 2010;15(1):53-63.
- Menzies L, Chamberlain SR, Laird AR, et al. Integrating evidence from neuroimaging and neuropsychological studies of obsessive-compulsive disorder: the orbitofronto-striatal model revisited. Neurosci Biobehav Rev. 2008;32(3):525-549.
- Skapinakis P, Caldwell DM, Hollingworth W, et al. Pharmacological and psychotherapeutic interventions for management of obsessive-compulsive disorder in adults: a systematic review and network meta-analysis. Lancet Psychiatry. 2016;3(8):730-739.
- Foa EB, Liebowitz MR, Kozak MJ, et al. Randomized, placebo-controlled trial of exposure and ritual prevention, clomipramine, and their combination in the treatment of obsessive-compulsive disorder. Am J Psychiatry. 2005;162(1):151-161.
- Goodman WK, Price LH, Rasmussen SA, et al. The Yale-Brown Obsessive Compulsive Scale: I. Development, use, and reliability. Arch Gen Psychiatry. 1989;46(11):1006-1011.
- Bloch MH, McGuire J, Landeros-Weisenberger A, et al. Meta-analysis of the dose-response relationship of SSRI in obsessive-compulsive disorder. Mol Psychiatry. 2010;15(8):850-855.
- Leckman JF, Denys D, Simpson HB, et al. Obsessive-compulsive disorder: a review of the diagnostic criteria and possible subtypes and dimensional specifiers for DSM-V. Depress Anxiety. 2010;27(6):507-527.
- Denys D, Mantione M, Figee M, et al. Deep brain stimulation of the nucleus accumbens for treatment-refractory obsessive-compulsive disorder. Arch Gen Psychiatry. 2010;67(10):1061-1068.
- Carmi L, Alyagon U, Barnea-Ygael N, et al. Clinical and electrophysiological outcomes of deep TMS over the medial prefrontal and anterior cingulate cortices in OCD patients. Brain Stimul. 2018;11(1):158-165.
- Moreno FA, Wiegand CB, Taitano EK, Delgado PL. Safety, tolerability, and efficacy of psilocybin in 9 patients with obsessive-compulsive disorder. J Clin Psychiatry. 2006;67(11):1735-1740.
- Pittenger C, Bloch MH, Williams K. Glutamate abnormalities in obsessive compulsive disorder: neurobiology, pathophysiology, and treatment. Pharmacol Ther. 2011;132(3):314-332.
- Abramowitz JS, Taylor S, McKay D. Obsessive-compulsive disorder. Lancet. 2009;374(9688):491-499.
- Stewart SE, Yu D, Scharf JM, et al. Genome-wide association study of obsessive-compulsive disorder. Mol Psychiatry. 2013;18(7):788-798.
- Simpson HB, Foa EB, Liebowitz MR, et al. Cognitive-behavioral therapy vs risperidone for augmenting serotonin reuptake inhibitors in obsessive-compulsive disorder: a randomized clinical trial. JAMA Psychiatry. 2013;70(11):1190-1199.
PubMed Topic Searches
- PubMed: OCD epidemiology prevalence
- PubMed: OCD exposure response prevention
- PubMed: OCD SSRI treatment
- PubMed: OCD clomipramine
- PubMed: OCD deep brain stimulation
- PubMed: OCD CSTC circuit neurobiology
- PubMed: OCD genetics GWAS
- PubMed: OCD children pediatric PANDAS
- PubMed: OCD body dysmorphic disorder
- PubMed: OCD hoarding disorder
- PubMed: OCD glutamate
- PubMed: OCD comorbidity anxiety
Connections
- Serotonin, Mood & SSRIs — interactive animation
- Depression
- Anxiety
- PTSD
- Eating Disorders
- Stress Management
- Magnesium
- Natural Anxiety Relief
- Ashwagandha
- Vitamin B6
- Autism
- ADHD
- Insomnia
- Bipolar Disorder
- Sleep Hygiene
- Schizophrenia
- Inositol
- Mental Health
- Grief
- Postpartum Depression
- Body Dysmorphic Disorder (BDD)
- Trichotillomania
- Hoarding Disorder