Loss of Appetite
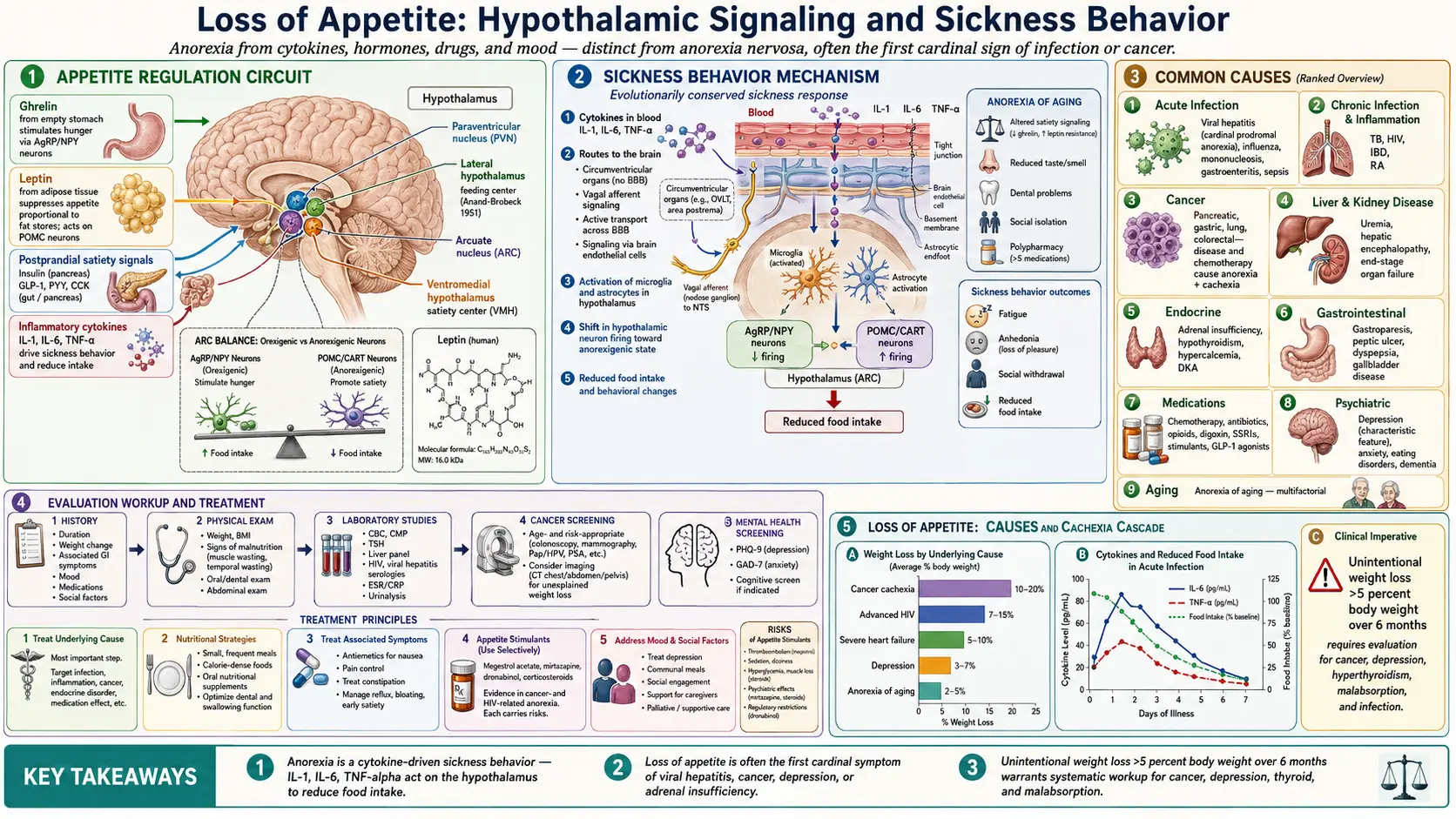
Table of Contents
- Overview
- Appetite Regulation
- Common Causes
- Evaluation
- Management
- When to Seek Medical Care
- Connections
- References & Research
- Featured Videos
Overview
Loss of appetite, medically termed anorexia, is a reduced desire to eat. It is distinct from anorexia nervosa, which is a psychiatric eating disorder. Anorexia is one of the cardinal symptoms of viral hepatitis and accompanies many infectious, inflammatory, malignant, neurologic, and psychiatric conditions. When prolonged, it leads to unintentional weight loss, malnutrition, and muscle wasting.
Appetite Regulation
Appetite is controlled by an interplay of peripheral signals and central circuits in the hypothalamus. Key players include:
- Ghrelin — secreted by the stomach when empty; stimulates hunger.
- Leptin — secreted by adipose tissue; suppresses appetite proportional to fat stores.
- Insulin, GLP-1, PYY, CCK — postprandial satiety signals.
- Inflammatory cytokines (IL-1, IL-6, TNF-alpha) — drive sickness behavior, including reduced appetite, during infection and chronic illness.
- Hypothalamic AgRP/NPY and POMC neurons — integrate these signals to control food intake.
Common Causes
- Acute infection — viral hepatitis, influenza, mononucleosis, gastroenteritis, sepsis.
- Chronic infection and inflammation — tuberculosis, HIV, inflammatory bowel disease, rheumatoid arthritis.
- Cancer — both the disease and treatments cause anorexia and cachexia, particularly in pancreatic, gastric, lung, and colorectal cancers.
- Liver and kidney disease — uremia, hepatic encephalopathy, end-stage organ failure.
- Endocrine — adrenal insufficiency, hypothyroidism, hypercalcemia, diabetic ketoacidosis.
- Gastrointestinal — gastroparesis, peptic ulcer disease, dyspepsia, gallbladder disease.
- Medications — chemotherapy, antibiotics, opioids, digoxin, SSRIs, stimulants, GLP-1 agonists.
- Psychiatric — depression, anxiety, eating disorders, dementia.
- Aging — the "anorexia of aging" reflects altered satiety signaling, reduced taste and smell, dental problems, social isolation, and medications.
Evaluation
- History — duration, weight change, associated GI symptoms, mood, medications, social factors.
- Physical exam — weight, BMI, signs of malnutrition, oral and dental exam, abdominal exam.
- Labs — CBC, CMP, TSH, liver panel, HIV, viral hepatitis serologies, ESR/CRP, urinalysis.
- Cancer screening — age- and risk-appropriate; consider imaging if unexplained weight loss.
- Mental health screening — PHQ-9, GAD-7.
Management
- Treat the underlying cause — most important step.
- Nutritional strategies — small frequent meals, calorie-dense foods, oral nutritional supplements, addressing dental and swallowing issues.
- Treat associated symptoms — antiemetics for nausea, pain control, treatment of constipation.
- Appetite stimulants — used selectively. Megestrol acetate, mirtazapine, dronabinol, and corticosteroids have evidence in cancer- and HIV-related anorexia, but each carries risks.
- Address mood and social factors — depression treatment, communal meals, support for caregivers.
When to Seek Medical Care
- Unintentional weight loss greater than 5% of body weight over six months.
- Loss of appetite with jaundice, dark urine, or abdominal pain.
- Inability to maintain adequate hydration.
- Associated fever, night sweats, blood in stool, or persistent vomiting.
- New depression, suicidal thoughts, or marked functional decline.
Connections
- Depression
- Cancer
- Hepatitis
- Kidney Disease
- Nausea and Vomiting
- Thyroid Disorders
- Fatigue
- Peptic Ulcer Disease
- Gallbladder Disease
- Anxiety
- Dementia
- Jaundice
- Dark Urine
- Abdominal Pain
- Sepsis
- Tuberculosis
- Metastatic Cancers
- Eating Disorders
- Stomach Cancer
References & Research
Historical Background
The dual-center hypothalamic model of appetite — a "feeding center" in the lateral hypothalamus and a "satiety center" in the ventromedial hypothalamus — was proposed by Anand and Brobeck in 1951 based on lesion studies. The discovery of leptin in 1994 by Jeffrey Friedman's group revolutionized appetite research by identifying a hormone secreted by adipose tissue that signals long-term energy stores to the brain. Subsequent work has uncovered a complex network of orexigenic and anorexigenic peptides that integrate metabolic, sensory, and emotional cues.
Key Research Papers
- Zhang Y, Proenca R, Maffei M, Barone M, Leopold L, Friedman JM. Positional cloning of the mouse obese gene and its human homologue. Nature. 1994;372(6505):425-432.
- Müller TD, Nogueiras R, Andermann ML, et al. Ghrelin. Molecular Metabolism. 2015;4(6):437-460.
- Bray GA. Obesity, a disorder of nutrient partitioning: the MONA LISA hypothesis. Journal of Nutrition. 1991;121(8):1146-1162.
- Morley JE. Anorexia of aging: physiologic and pathologic. American Journal of Clinical Nutrition. 1997;66(4):760-773.
- Fearon K, Strasser F, Anker SD, et al. Definition and classification of cancer cachexia: an international consensus. The Lancet Oncology. 2011;12(5):489-495.
- Dantzer R, Kelley KW. Twenty years of research on cytokine-induced sickness behavior. Brain, Behavior, and Immunity. 2007;21(2):153-160.
- Yeh SS, Schuster MW. Geriatric cachexia: the role of cytokines. American Journal of Clinical Nutrition. 1999;70(2):183-197.