Pellagra: The Disease of the Four D's
Pellagra is a systemic disease caused by severe deficiency of niacin (vitamin B3) or its amino acid precursor tryptophan. The name derives from the Italian "pelle agra," meaning "rough skin," reflecting the characteristic dermatitis that is often the first visible sign. Pellagra has shaped public health history, devastated entire populations, and remains relevant in clinical practice today, particularly among vulnerable groups including people with alcoholism, malabsorptive conditions, and those taking certain medications.
Table of Contents
- Key Points at a Glance
- The Four D's of Pellagra
- Dermatitis
- Diarrhea
- Dementia
- Death
- Historical Context: Corn-Dependent Diets
- The Tryptophan-Niacin Conversion Pathway
- Hartnup Disease
- Alcoholism-Related Pellagra
- Drug-Induced Pellagra
- Carcinoid Syndrome
- Diagnosis and Treatment
- Endemic vs. Sporadic Pellagra
- Research Papers
- Connections
- Featured Videos
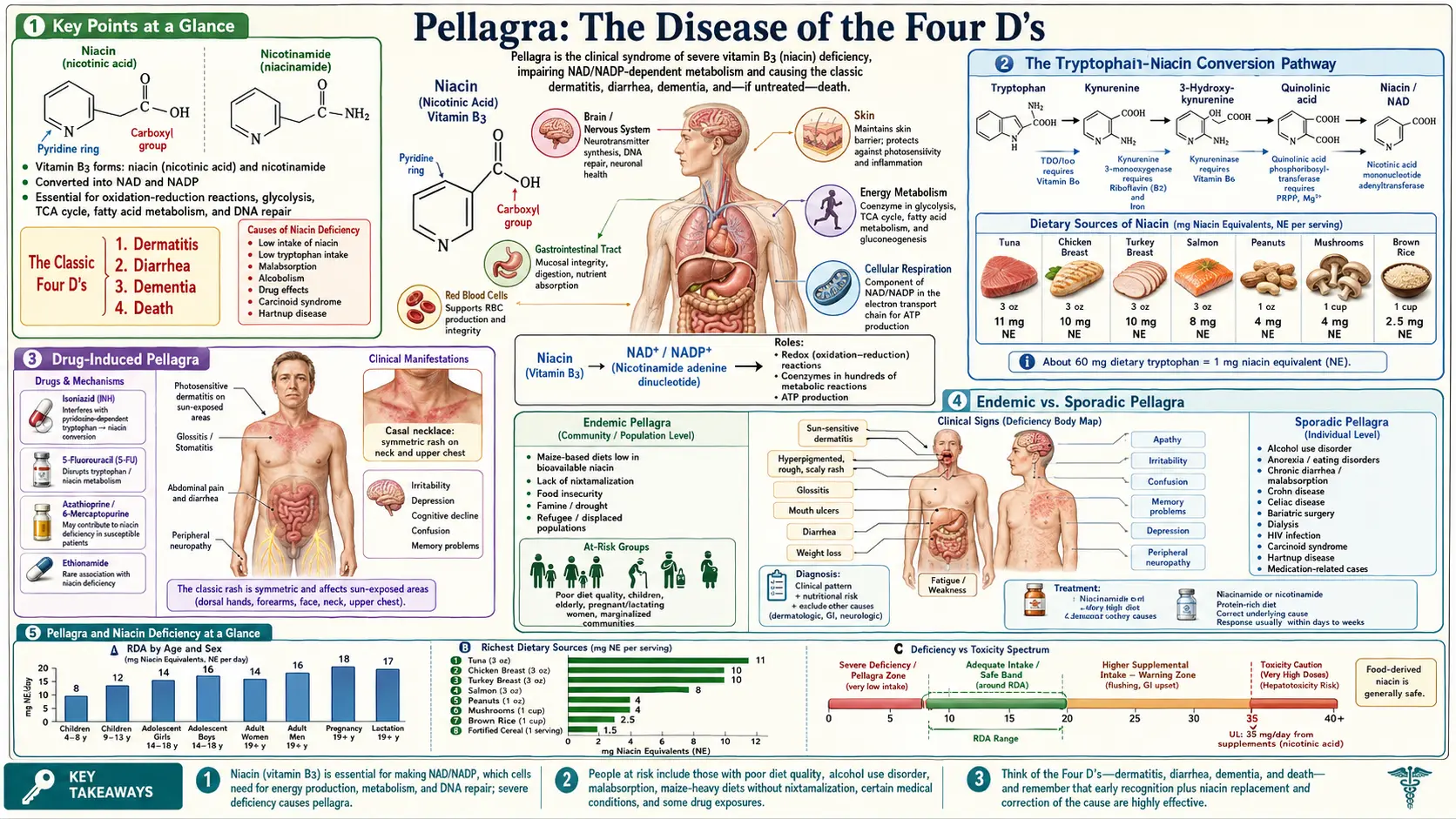
Key Points at a Glance
- Caused by severe niacin (B3) or tryptophan deficiency — without treatment, pellagra is uniformly fatal.
- Classic tetrad: dermatitis, diarrhea, dementia, death (the "Four D's").
- Casal's necklace — pathognomonic collar of hyperpigmented dermatitis on sun-exposed skin of the neck.
- Historically associated with corn-dominant diets lacking nixtamalization; devastated the American South (3 million cases, 100,000 deaths, 1906–1940).
- Modern cases arise from chronic alcoholism, malabsorption, eating disorders, isoniazid therapy, carcinoid syndrome, and Hartnup disease.
- Tryptophan conversion yields approximately 1 mg niacin per 60 mg tryptophan (requires B2, B6, iron).
- Nicotinamide (100–300 mg/day) is the treatment of choice — dermatitis and diarrhea resolve in 24–48 hours.
- Grain fortification has virtually eliminated endemic pellagra in developed nations.
The Four D's of Pellagra
The clinical presentation of pellagra is classically summarized by the mnemonic of the "Four D's," which describe the progressive stages of untreated niacin deficiency:
Dermatitis
The dermatological manifestations of pellagra are among the most distinctive of any nutritional deficiency:
- Photosensitive distribution — the rash appears symmetrically on sun-exposed areas, including the dorsum of the hands, forearms, face, neck, and feet. The sharp demarcation between affected and unaffected skin follows sun exposure lines rather than dermatomes.
- Progression of skin changes — initially resembling a sunburn with erythema and edema, the rash evolves through vesiculation, crusting, and desquamation to produce thickened, hyperpigmented, rough, and scaly skin.
- Casal's necklace — a broad band of dermatitis encircling the neck in a collar-like distribution, named after the Spanish physician Gaspar Casal who first described pellagra in 1735. This sign is considered pathognomonic for pellagra and may extend to the upper chest in a butterfly or bib pattern.
- Pellagrous glove and boot — symmetric dermatitis on the dorsal surfaces of the hands and feet, often with sharp cutoffs at the wrists and ankles, resembling gloves and boots.
- Mucosal involvement — glossitis (bright red, swollen, painful tongue), angular stomatitis, and cheilitis are common. The tongue may progress from red and edematous to smooth, atrophic, and "beefy" in appearance.
Diarrhea
Gastrointestinal symptoms reflect the high turnover rate of intestinal epithelial cells, which are particularly sensitive to NAD+ depletion:
- Watery diarrhea — caused by inflammation and atrophy of the intestinal mucosa, leading to malabsorption that further exacerbates the nutritional deficiency in a vicious cycle.
- Nausea, vomiting, and abdominal pain — these symptoms often precede diarrhea and may be misattributed to other gastrointestinal disorders.
- Achlorhydria — reduced gastric acid secretion occurs due to atrophy of the gastric mucosa, impairing digestion and nutrient absorption.
- Esophagitis and proctitis — inflammation may extend throughout the gastrointestinal tract, causing dysphagia and rectal discomfort.
Dementia
Neuropsychiatric manifestations can range from subtle cognitive changes to severe encephalopathy:
- Early symptoms — insomnia, anxiety, irritability, apathy, poor concentration, and fatigue. These nonspecific complaints are easily overlooked or attributed to other causes.
- Progressive encephalopathy — confusion, disorientation, memory loss, hallucinations, delusions, and psychosis. Pellagra was historically a major cause of admissions to psychiatric institutions.
- Motor disturbances — tremor, rigidity, spastic paraparesis, and peripheral neuropathy may occur. The combination of neuropsychiatric and motor symptoms can mimic other neurological diseases.
- Mechanism — NAD+ depletion impairs energy production in neurons, disrupts serotonin synthesis (tryptophan is diverted away from serotonin toward niacin production), and compromises DNA repair in the central nervous system.
Death
If left untreated, pellagra is uniformly fatal. Death typically results from multi-organ failure, secondary infections facilitated by immune dysfunction, or complications of severe malnutrition. The progression from early symptoms to death can occur over months to years, depending on the severity of the deficiency and the presence of complicating factors.
Historical Context: Corn-Dependent Diets
Pellagra became epidemic in populations that relied heavily on corn (maize) as a dietary staple:
- European epidemics — after maize was introduced from the Americas in the 16th century, pellagra became endemic in Mediterranean countries, particularly in northern Italy, Spain, and southern France, where corn polenta replaced more diverse grains.
- American South — pellagra reached epidemic proportions in the early 20th century, with an estimated 3 million cases and 100,000 deaths between 1906 and 1940. Sharecroppers and mill workers subsisting on the "three M" diet of meat (fatback), meal (cornmeal), and molasses were most affected.
- The corn paradox — maize contains niacin, but in a bound form (niacytin) that is not bioavailable without alkaline processing. Mesoamerican peoples traditionally treated corn with lime (calcium hydroxide) in a process called nixtamalization, which liberates bound niacin. This knowledge was not transferred when corn was adopted in Europe and the American South.
- Joseph Goldberger's contribution — in the 1910s and 1920s, U.S. Public Health Service physician Joseph Goldberger proved through prison experiments and epidemiological studies that pellagra was a nutritional deficiency, not an infectious disease as was widely believed. His work eventually led to niacin fortification of flour and cereal products.
The Tryptophan-Niacin Conversion Pathway
The body can synthesize niacin from the essential amino acid tryptophan through the kynurenine pathway:
- Conversion ratio — approximately 60 mg of dietary tryptophan yields 1 mg of niacin (1 niacin equivalent). This conversion is inefficient and requires adequate status of vitamin B6, vitamin B2, and iron as cofactors.
- Pathway enzymes — tryptophan is first oxidized by tryptophan 2,3-dioxygenase (TDO) or indoleamine 2,3-dioxygenase (IDO) to N-formylkynurenine, then converted through several intermediate steps to quinolinic acid, and finally to nicotinic acid mononucleotide, which enters the NAD+ biosynthetic pathway.
- Competition with serotonin — tryptophan is also the precursor for serotonin synthesis. When niacin status is low, more tryptophan is diverted toward NAD+ production, potentially reducing serotonin availability and contributing to the neuropsychiatric symptoms of pellagra.
- Clinical significance — conditions that reduce tryptophan availability or impair the kynurenine pathway can precipitate pellagra even when dietary niacin intake appears adequate.
Hartnup Disease
Hartnup disease is an autosomal recessive disorder affecting the transport of neutral amino acids, including tryptophan:
- Molecular basis — mutations in the SLC6A19 gene impair the neutral amino acid transporter B0AT1 in the intestinal epithelium and renal proximal tubule, leading to tryptophan malabsorption and renal wasting.
- Pellagra-like presentation — affected individuals develop photosensitive dermatitis, cerebellar ataxia, and psychiatric symptoms that are clinically indistinguishable from nutritional pellagra.
- Diagnosis — characterized by massive neutral aminoaciduria detected on urine amino acid analysis. Symptoms are often episodic and triggered by poor diet, illness, or stress.
- Treatment — high-dose oral nicotinamide supplementation (50 to 200 mg daily) effectively prevents and treats symptoms by bypassing the tryptophan dependency.
Alcoholism-Related Pellagra
Chronic alcohol use disorder is the most common cause of pellagra in developed countries today:
- Multiple contributing factors — poor dietary intake, impaired intestinal absorption, increased metabolic demand, hepatic dysfunction reducing NAD+ synthesis, and direct toxic effects of alcohol on niacin metabolism all converge.
- Diagnostic challenges — pellagra in alcoholic patients is frequently misdiagnosed as alcoholic dementia, Wernicke encephalopathy (thiamine deficiency), or alcohol-related dermatitis. The classic triad may not be fully present.
- Pellagrous encephalopathy — may present acutely with confusion, clouding of consciousness, and cog-wheel rigidity, sometimes called "alcoholic pellagra encephalopathy." This condition carries significant mortality if not recognized and treated promptly.
Drug-Induced Pellagra
Isoniazid
Isoniazid, a cornerstone of tuberculosis treatment, is a structural analog of nicotinamide that interferes with niacin metabolism. It inhibits the enzyme kynureninase in the tryptophan-to-niacin conversion pathway and may also directly compete with niacin for incorporation into NAD+. Pyridoxine (vitamin B6) supplementation is routinely co-administered with isoniazid, partly to mitigate this effect.
Other Medications
- 6-Mercaptopurine and 5-fluorouracil — these chemotherapeutic agents can cause pellagra through interference with NAD+ synthesis.
- Pyrazinamide — another anti-tuberculosis drug that is a structural analog of nicotinamide and can deplete niacin stores.
- Ethionamide — used in multidrug-resistant tuberculosis regimens, can contribute to niacin depletion.
- Phenobarbital and other anticonvulsants — may increase the catabolism of tryptophan through induction of hepatic enzymes.
Carcinoid Syndrome
Carcinoid tumors can divert up to 60 percent of dietary tryptophan toward serotonin synthesis, leaving insufficient substrate for niacin production:
- Mechanism — carcinoid tumors express tryptophan hydroxylase, which converts tryptophan to 5-hydroxytryptophan and then to serotonin (5-HT). This massive diversion of tryptophan away from the kynurenine pathway precipitates niacin deficiency.
- Clinical presentation — patients with metastatic carcinoid syndrome may develop classic pellagra superimposed on carcinoid symptoms (flushing, diarrhea, bronchospasm). The overlap of flushing and diarrhea between the two conditions can delay recognition of concurrent pellagra.
- Management — niacin supplementation is an important component of supportive care in carcinoid syndrome alongside somatostatin analogs.
Diagnosis and Treatment
Diagnosis
- Clinical diagnosis — pellagra is primarily a clinical diagnosis based on the characteristic triad of dermatitis, diarrhea, and dementia in the setting of risk factors for niacin deficiency.
- Urinary metabolites — measurement of N1-methylnicotinamide and its pyridone metabolite (2-pyridone) in a 24-hour urine collection can confirm niacin deficiency. A ratio of 2-pyridone to N1-methylnicotinamide below 1.0 suggests deficiency.
- NAD/NADP ratio — erythrocyte NAD levels and the NAD-to-NADP ratio can serve as biomarkers, with values below 1.0 indicating deficiency.
- Therapeutic trial — rapid clinical improvement following niacin supplementation serves as both diagnostic confirmation and treatment.
Treatment
- Nicotinamide (niacinamide) — preferred over nicotinic acid for treatment because it does not cause flushing. Typical dose is 100 mg orally three times daily for mild to moderate cases.
- Severe or acute pellagra — 300 mg daily in divided doses, with improvement in dermatitis and diarrhea expected within 24 to 48 hours. Neuropsychiatric symptoms may take weeks to months to resolve and may not fully reverse if treatment is delayed.
- Comprehensive nutritional rehabilitation — patients with pellagra typically have multiple concurrent nutritional deficiencies. A balanced diet rich in protein, along with a B-complex supplement, should accompany specific niacin therapy.
- Address underlying causes — treatment of alcoholism, discontinuation or adjustment of offending medications, management of malabsorptive conditions, and dietary counseling are essential for sustained recovery.
Endemic vs. Sporadic Pellagra
- Endemic pellagra — occurs in populations where niacin-poor staples (corn, sorghum, millet) dominate the diet without adequate protein sources. It remains a public health concern in parts of sub-Saharan Africa, India, and China, particularly during famine or food insecurity. Grain fortification programs have dramatically reduced endemic pellagra in developed nations.
- Sporadic pellagra — occurs in individuals within populations where niacin deficiency is otherwise uncommon. Risk groups include people with chronic alcoholism, homeless individuals, patients with eating disorders (particularly anorexia nervosa), those with inflammatory bowel disease or other malabsorptive conditions, patients on multiple interacting medications, and individuals on highly restrictive diets. Sporadic cases are easily missed because clinicians may not consider pellagra in their differential diagnosis.
Research Papers
- PubMed — Pellagra and niacin deficiency (topic search)
- PubMed — Hartnup disease tryptophan transport (topic search)
- PubMed — Goldberger pellagra epidemiology (topic search)
- PubMed — Alcoholic pellagra encephalopathy (topic search)
- PubMed — Isoniazid-induced pellagra (topic search)
- PubMed — Carcinoid syndrome and niacin deficiency (topic search)
- PubMed — Nixtamalization and niacin bioavailability (topic search)
- PubMed — Nicotinamide treatment of pellagra (topic search)
- NIH Office of Dietary Supplements — Niacin Fact Sheet for Health Professionals
- Linus Pauling Institute — Niacin
- Harvard T.H. Chan School of Public Health — Niacin (Vitamin B3)
Connections
- All Vitamins
- Vitamin B3
- Niacin and Cholesterol
- Vitamin B6
- Vitamin B12
- Riboflavin and Energy Production
- Thiamine and Beriberi
- Tryptophan
- Depression
- Anxiety
- Dementia
- Tuberculosis
- Eating Disorders
- Iron
- Fatigue
- Inflammatory Bowel Disease
- Niacin Vitamin B3