Schistosoma — The Cause of Schistosomiasis
Symptoms & Diagnosis
How the disease unfolds from skin entry to chronic organ damage, and how it is found.
Urogenital Schistosomiasis
Blood in the urine, bladder damage, bladder-cancer risk, and female genital schistosomiasis.
Intestinal & Hepatic
Bloody diarrhea, liver fibrosis, and portal hypertension from S. mansoni and S. japonicum.
Acute & Swimmer's Itch
Cercarial dermatitis and Katayama fever — the early reactions, common in travelers.
Treatment & Prevention
The praziquantel-centered approach and how schistosomiasis is controlled.
Praziquantel Treatment
The single drug for all major species — how it works and its limits.
Prevention: Avoiding Freshwater
Why staying out of infested fresh water is the main personal defense.
Mass Drug Administration
School-based deworming, snail control, and the push toward elimination.
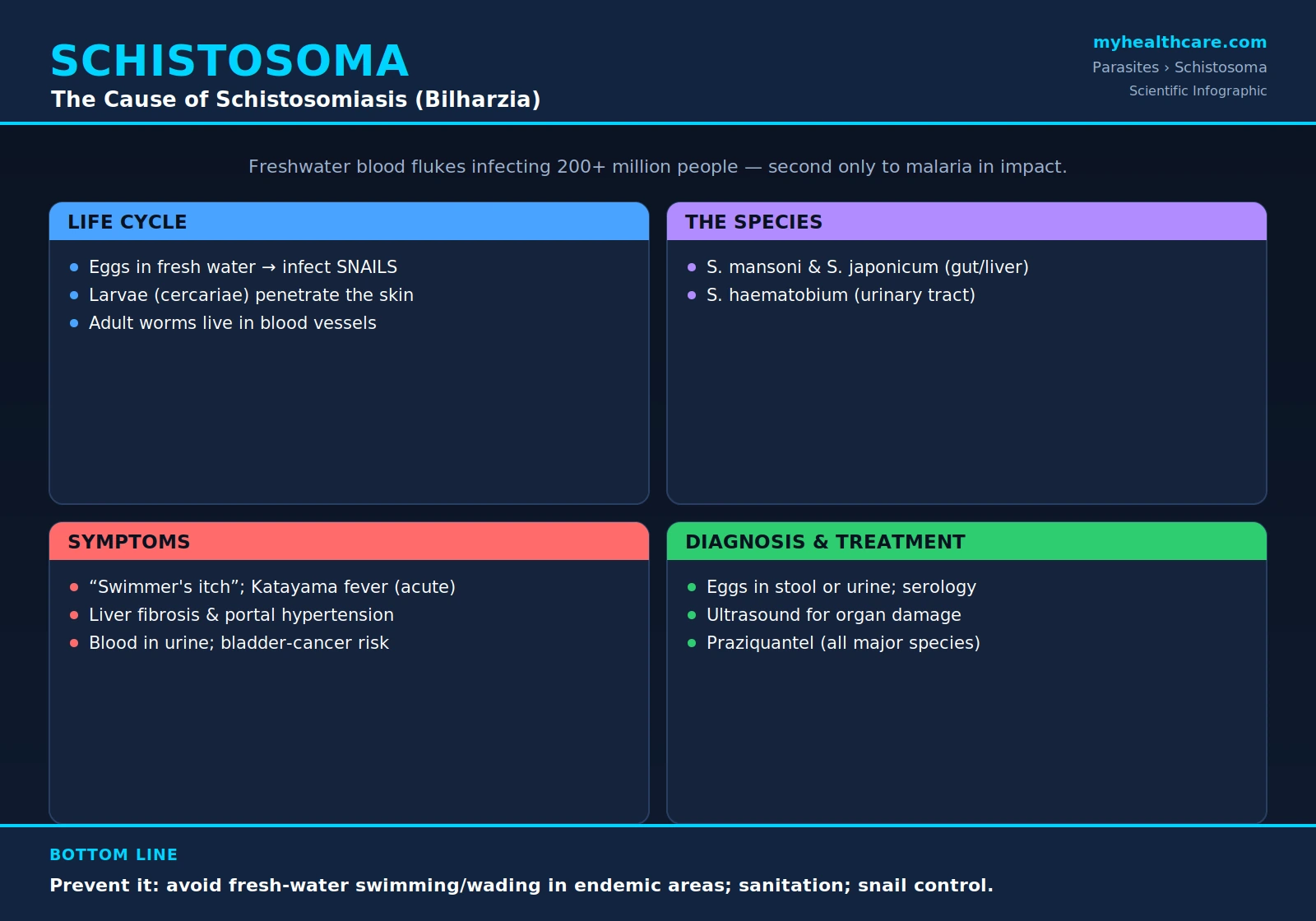
Schistosoma is a genus of parasitic flatworms — commonly called blood flukes — that cause schistosomiasis, also known as bilharzia. The disease affects more than 200 million people worldwide and, after malaria, ranks among the most socioeconomically devastating of all parasitic diseases. The great majority of the burden falls on sub-Saharan Africa, where contact with contaminated fresh water is a part of everyday life. This page explains what these worms are, the remarkable journey their life cycle takes through freshwater snails and back into people, why the disease they cause can quietly damage the intestines, liver, and bladder over many years, and how schistosomiasis is diagnosed, treated, and prevented.
Table of Contents
- What Is Schistosoma?
- Life Cycle
- How It Spreads
- Symptoms
- Diagnosis
- Treatment
- Prevention
- Key Research Papers
- Featured Videos
1. What Is Schistosoma?
Schistosoma are parasitic flatworms known as blood flukes, a type of trematode. Unlike most flukes, in which a single hermaphroditic worm carries both sexes, schistosomes have separate male and female adults that live permanently paired together, the slender female resting in a groove that runs the length of the stockier male's body. They make their home inside the small blood vessels of the human host, and it is from this bloodstream residence that they take their common name.
Several species infect humans, and which one a person carries shapes which organs the disease attacks:
- Schistosoma mansoni and Schistosoma japonicum live in the veins draining the intestine and cause intestinal and liver disease. S. mansoni is found across Africa, the Middle East, and parts of South America and the Caribbean; S. japonicum occurs in China, the Philippines, and Indonesia.
- Schistosoma haematobium lives in the veins around the bladder and causes urinary (urogenital) disease. It is found across Africa and the Middle East and is the species classically associated with blood in the urine.
The illness these worms produce, schistosomiasis (or bilharzia, after Theodor Bilharz, who identified the worm in the nineteenth century), affects more than 200 million people. After malaria, it is considered among the most socioeconomically devastating parasitic diseases on Earth, sapping the strength, growth, and productivity of whole communities. Sub-Saharan Africa carries by far the heaviest share of the global burden.
2. Life Cycle
The life cycle of Schistosoma is one of the more extraordinary in human parasitology, requiring a detour through a tiny freshwater snail before the worm can return to people. Understanding it is the key to understanding everything about how the disease spreads, sickens, and can be stopped.
The journey unfolds in a continuous loop:
- Eggs leave the body. Adult worm pairs living in the human bloodstream lay eggs. Some of these eggs work their way through the vessel and organ walls and are passed out of the body in urine (with S. haematobium) or in stool (with S. mansoni and S. japonicum).
- Eggs hatch in fresh water. If the eggs reach fresh water, they hatch and release a swimming larval form that must quickly find its next host.
- The larvae infect snails. These larvae seek out and infect specific freshwater snails, which serve as the parasite's intermediate host. Each schistosome species depends on its own particular kind of snail, which is why the disease occurs only where those snails live.
- Snails release cercariae. Inside the snail the parasite multiplies and, after several weeks, the snail releases enormous numbers of a different free-swimming larval form called cercariae into the water.
- Cercariae penetrate human skin. When a person enters infested water, the cercariae penetrate the skin directly, shedding their forked tails as they bore in.
- Larvae mature into adult worms. Once inside, the young worms travel through the bloodstream and lungs, then mature into adult males and females that pair up and settle in the blood vessels around the intestine or bladder, where they begin to lay eggs — and the cycle starts again.
The disease itself is driven largely not by the adult worms but by the eggs. Many of the eggs a female lays never escape the body; instead they become trapped in the tissues of the bladder, intestine, liver, and elsewhere. The body's prolonged immune reaction to these lodged eggs — walling them off with inflammation and scarring — is what produces most of the long-term damage of schistosomiasis.
3. How It Spreads
Schistosomiasis spreads through skin contact with fresh water that contains the infective larvae (cercariae). There is no need to swallow the water; the larvae simply burrow through the skin during ordinary contact. The everyday activities that put people at risk are the ordinary business of life near rivers, lakes, ponds, and irrigation canals in affected regions, including:
- Swimming and wading.
- Washing clothes, dishes, and bathing.
- Fishing.
- Farming and other work in irrigated fields and along waterways.
Importantly, schistosomiasis cannot be passed directly from one person to another. An infected person is not contagious by touch. The parasite must always complete its detour through the freshwater snail before it can infect a new host, so the disease can only spread where infected snails and human water contact come together.
What keeps the cycle turning is poor sanitation. When human urine and feces containing schistosome eggs reach the fresh water where the snails live — through open defecation or inadequate latrines — the eggs hatch, infect new snails, and seed the water with the next generation of cercariae. Schistosomiasis is therefore as much a disease of unsafe water and absent sanitation as it is a disease of a worm, and it concentrates in poor rural communities that lack clean water supplies and toilets.
4. Symptoms
The symptoms of schistosomiasis unfold in stages, and they reflect the worm's life cycle — first the larvae entering the skin, then the early growing worms, and finally, over years, the body's reaction to the eggs trapped in its tissues.
Early signs. Where the cercariae penetrate the skin, an itchy rash sometimes appears within hours to days — commonly called "swimmer's itch." Weeks after infection, as the young worms mature and the female begins laying eggs, some people develop an acute illness known as Katayama fever, a systemic reaction marked by fever, hives, cough, and a striking rise in eosinophils (a type of white blood cell that responds to parasites). Katayama fever is most often seen in travelers and others newly exposed to the parasite.
Chronic disease. The long-term harm comes from the body's reaction to eggs that become trapped in tissue, and it depends on which species a person carries:
- Intestinal and liver disease (S. mansoni and S. japonicum): abdominal pain, diarrhea, blood in the stool, and, over years, scarring of the liver. This liver scarring can obstruct blood flow and lead to dangerous portal hypertension — high pressure in the veins feeding the liver, which can cause an enlarged spleen, fluid in the abdomen, and bleeding from swollen veins in the esophagus.
- Urinary disease (S. haematobium): the hallmark is blood in the urine. Over time the parasite causes bladder damage and scarring, an increased risk of bladder cancer, and, in women, female genital schistosomiasis — egg-induced damage to the reproductive tract that can cause symptoms easily mistaken for a sexually transmitted infection and that has been linked to greater susceptibility to HIV.
Because chronic schistosomiasis develops slowly and quietly, many people carry the infection for years before its consequences become apparent, which is part of what makes the disease so insidious and so damaging to long-term health.
5. Diagnosis
Diagnosing schistosomiasis means proving that the parasite is present and gauging how much damage it has done. Several complementary approaches are used:
- Finding eggs under the microscope. The classic and most direct method is to detect the worm's eggs in body samples — in the stool for S. mansoni and S. japonicum, and in the urine for S. haematobium. The eggs of each species have a distinctive shape, so seeing them both confirms the infection and identifies the species.
- Antibody and antigen tests. Blood tests can detect antibodies the immune system makes against the parasite, which is especially useful in travelers and in light infections where eggs may be scarce. Antigen tests — including rapid urine dipsticks that detect schistosome antigens such as circulating cathodic antigen — can indicate an active, ongoing infection.
- Imaging. Ultrasound and other imaging are used to assess the organ damage the worm has caused — the characteristic scarring of the liver, and changes in the bladder and urinary tract — helping to stage the disease and guide care even when the worms themselves cannot be seen.
6. Treatment
The mainstay of treatment for schistosomiasis is praziquantel, an oral antiparasitic medicine that is effective against all of the major human species — S. mansoni, S. haematobium, and S. japonicum — which makes it the single drug at the center of both individual treatment and large-scale control programs.
A few practical points are worth understanding about how the drug works:
- Praziquantel works best against mature adult worms and is less effective against the immature, developing stages. For this reason, a person treated very soon after exposure (before the worms have matured) may still harbor surviving worms.
- Because of this, a second dose is sometimes given — for example, several weeks later to catch worms that were too young to be killed the first time, or as a repeat course in heavily infected individuals.
This information is presented as reported in the medical literature and is for general education; the diagnosis and treatment of schistosomiasis should always be directed by a qualified clinician, who can confirm the species, judge the timing and number of doses, and watch for the reactions that can accompany the death of large numbers of worms.
7. Prevention
Because the parasite depends on the meeting of contaminated water, snails, and human skin, schistosomiasis can be attacked at several points in its cycle. Prevention combines personal precautions with community-wide public-health measures:
- Avoid contact with fresh water — swimming, wading, or bathing — in regions where schistosomiasis occurs. For travelers, steering clear of untreated rivers, lakes, and ponds is the most reliable protection.
- Improve sanitation and safe water supplies. Providing latrines and clean water for washing and bathing keeps human eggs out of the snails' habitat and keeps people out of infested water, breaking the cycle at its source.
- Snail control. Reducing the population of the freshwater snails that host the parasite — through environmental management or molluscicides — removes the intermediate host the worm cannot do without.
- Mass drug administration. In affected communities, public-health programs periodically give preventive praziquantel to whole populations — especially schoolchildren, who tend to carry the heaviest infections — to lower the overall burden of disease and reduce the number of eggs returning to the water.
Together these measures — avoiding risky water, building sanitation and clean-water infrastructure, controlling snails, and treating communities at scale — form the backbone of the global effort to control and, in some places, eliminate schistosomiasis.
Key Research Papers
Peer-reviewed reviews and studies on Schistosoma and the schistosomiasis it causes — covering the biology and life cycle of the parasite, the global burden of disease, transmission and water resources, diagnosis, and the complications of urogenital and intestinal infection. Journal names appear as plain text; the year/volume/pages link opens the full citation via DOI.
- Colley DG, Bustinduy AL, Secor WE, King CH. Human schistosomiasis. The Lancet. 2014;383(9936):2253–2264.
- Gryseels B, Polman K, Clerinx J, Kestens L. Human schistosomiasis. The Lancet. 2006;368(9541):1106–1118.
- Ross AG, Bartley PB, Sleigh AC, Olds GR, et al. Schistosomiasis. New England Journal of Medicine. 2002;346(16):1212–1220.
- Steinmann P, Keiser J, Bos R, Tanner M, Utzinger J. Schistosomiasis and Water Resources Development: Systematic Review, Meta-Analysis, and Estimates of People at Risk. The Lancet Infectious Diseases. 2006;6(7):411–425.
- Hotez PJ, Kamath A. Neglected Tropical Diseases in Sub-Saharan Africa: Review of Their Prevalence, Distribution, and Disease Burden. PLoS Neglected Tropical Diseases. 2009;3(8):e412.
- Mbabazi PS, Andan O, Fitzgerald DW, Chitsulo L, et al. Examining the Relationship Between Urogenital Schistosomiasis and HIV Infection. PLoS Neglected Tropical Diseases. 2011;5(12):e1396.
- Standley C, Lwambo N, Lange C, Kariuki H, et al. Performance of Circulating Cathodic Antigen (CCA) Urine-Dipsticks for Rapid Detection of Intestinal Schistosomiasis in Schoolchildren from Shoreline Communities of Lake Victoria. Parasites & Vectors. 2010;3:7.
- Dabo A, Badawi HM, Bary B, Doumbo OK. Urinary Schistosomiasis Among Preschool-Aged Children in Sahelian Rural Communities in Mali. Parasites & Vectors. 2011;4:21.
- Hotez PJ, Savioli L, Fenwick A. Neglected Tropical Diseases of the Middle East and North Africa: Review of Their Prevalence, Distribution, and Opportunities for Control. PLoS Neglected Tropical Diseases. 2012;6(2):e1475.
Live PubMed Searches
Each link opens a live PubMed query so results stay current as new papers are indexed.
- Schistosoma life cycle
- Schistosomiasis praziquantel treatment
- Schistosoma haematobium urinary disease
- Schistosoma mansoni liver fibrosis
- Female genital schistosomiasis
- Schistosomiasis diagnosis circulating antigen
- Schistosomiasis snail intermediate host
- Schistosomiasis mass drug administration control
Connections
- All Parasites
- Acanthamoeba
- Giardia
- Malaria
- Toxoplasma
- Entamoeba
- Cryptosporidium
- Ascaris
- Pinworm
- Hookworm
- Tapeworm
- Schistosomiasis — the general disease overview for the illness these blood flukes cause.
- Infectious Disease
- Urology
- All Conditions