Pain Reprocessing Therapy and Pain Neuroscience Education
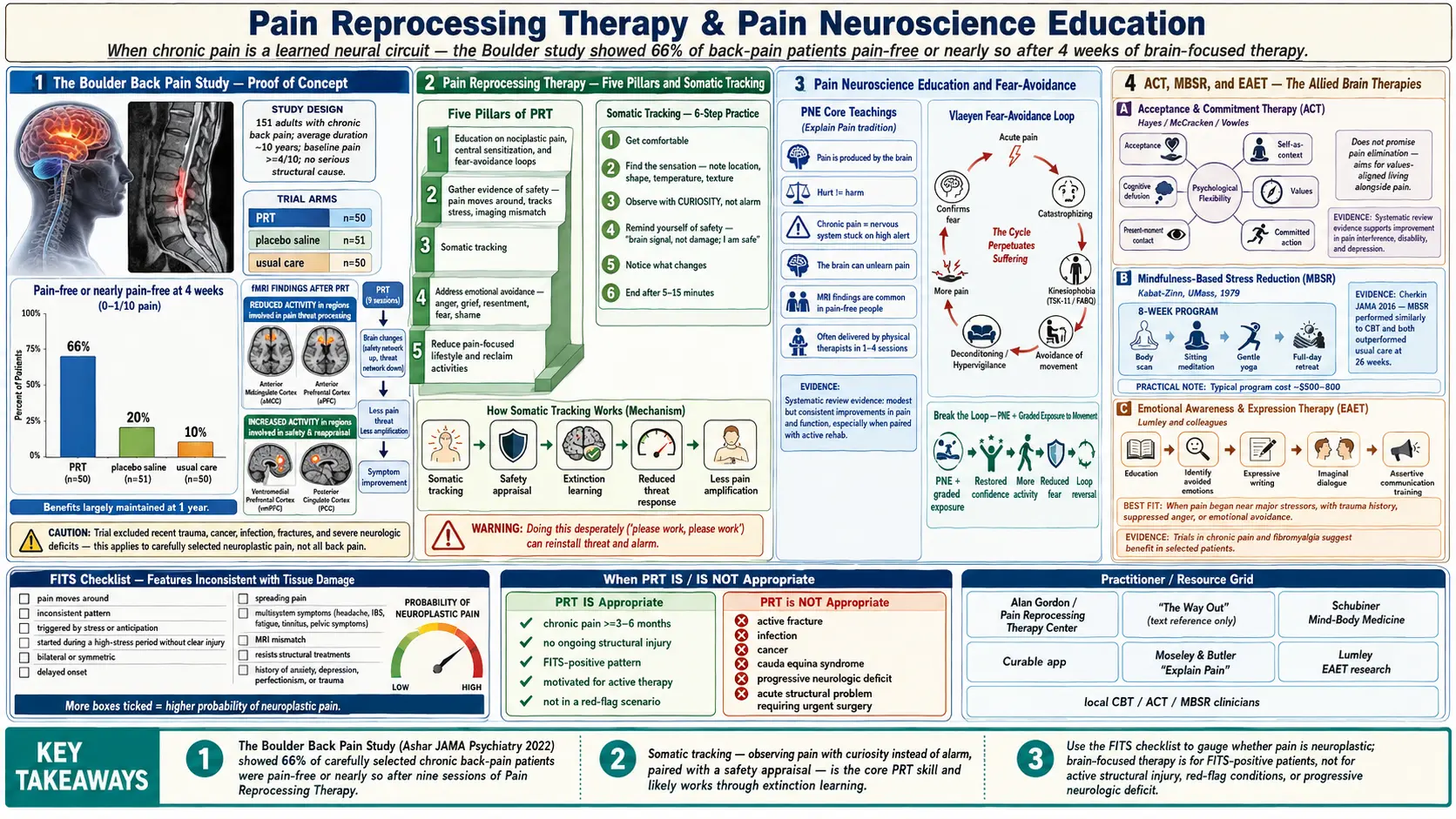
Table of Contents
- Why the Brain Is Now Part of Pain Treatment
- The Boulder Back Pain Study — Proof of Concept
- Pain Reprocessing Therapy (PRT) in Detail
- Somatic Tracking — The Core PRT Skill
- Authentic Self-Expression and Avoided Emotions
- Pain Neuroscience Education (PNE)
- Fear-Avoidance and Kinesiophobia
- Acceptance and Commitment Therapy (ACT)
- Mindfulness-Based Stress Reduction (MBSR)
- Emotional Awareness and Expression Therapy (EAET)
- FITS — Is Your Pain Likely Neuroplastic?
- When PRT Is NOT Appropriate
- Finding a Practitioner and What It Costs
- Combining PRT with Medication and Other Treatment
- Self-Guided Resources
- Key Research Papers
- Connections
- Featured Videos
Why the Brain Is Now Part of Pain Treatment
For a century, medicine treated chronic pain like a plumbing problem. Find the damaged tissue, fix it, and the pain should stop. For acute injuries — a sprained ankle, a kidney stone, a fresh surgical wound — that model works beautifully. For chronic pain that has lasted more than three to six months, it often fails. MRI scans reveal "bulging discs" or "degeneration" in perfectly pain-free people. Surgeries correct the visible abnormality and leave the pain untouched. Patients are told the problem is structural, given opioids or injections, and sent home.
In the last fifteen years a different model has taken hold, backed by functional MRI studies, placebo research, and a growing body of randomized controlled trials. The model says this: pain is always made by the brain. Tissue damage sends danger signals, but the brain decides — moment by moment — how much pain to produce, based on context, memory, expectation, emotion, and learned associations. In chronic pain, especially the kind with no clear ongoing injury, the brain has often learned the pain. The nerves fire not because tissue is damaged but because the pain circuit has become its own habit. Clinicians now call this nociplastic or neuroplastic pain. It is as real as a broken bone. It is just generated higher up in the nervous system.
Pain Reprocessing Therapy (PRT), Pain Neuroscience Education (PNE), Acceptance and Commitment Therapy (ACT), Mindfulness-Based Stress Reduction (MBSR), and Emotional Awareness and Expression Therapy (EAET) are the five best-studied treatments aimed at this learned-pain circuitry. This article walks through each one, explains when they help, and tells you how to find a practitioner.
The Boulder Back Pain Study — Proof of Concept
The single trial that changed the conversation is the Boulder Back Pain Study, published by Yoni Ashar, Alan Gordon, Tor Wager and colleagues in JAMA Psychiatry in 2022. It was a randomized controlled trial of 151 adults with chronic back pain (average duration: ten years, average intensity: 4/10 or higher, no serious structural cause). Participants were randomized to one of three groups:
- Pain Reprocessing Therapy (PRT). One 60-minute evaluation session plus eight 60-minute sessions over four weeks. Therapy focused on reappraising pain as a safe brain-generated signal rather than tissue damage.
- Placebo. A subcutaneous saline injection framed as a promising pain treatment.
- Usual care. Whatever the patient and their doctors chose to do.
At the four-week endpoint, the results were striking:
- 66% of the PRT group were pain-free or nearly pain-free (pain score 0 or 1 out of 10).
- 20% of the placebo group reached the same threshold.
- 10% of the usual-care group reached the same threshold.
The gains held at one-year follow-up. Functional MRI showed reduced activity in brain regions involved in pain processing (anterior midcingulate cortex, anterior prefrontal cortex) in the PRT group, and increased activity in regions associated with threat reappraisal. Crucially, the trial deliberately excluded people with dangerous structural causes (recent trauma, cancer, infection, fractures, severe neurological deficits). This is a study of neuroplastic back pain, not all back pain. For the right patient, a four-week brain-focused course beat everything else medicine was offering.
Pain Reprocessing Therapy (PRT) in Detail
PRT was developed by psychotherapist Alan Gordon at the Pain Psychology Center in Los Angeles, building on the work of John Sarno (who used the term "TMS" — tension myositis/myoneural syndrome) and on pain neuroscience research from David Butler, Lorimer Moseley, and Howard Schubiner. Gordon's book The Way Out (2021) is the lay-reader protocol. The clinical manual is available through the Pain Reprocessing Therapy Center.
PRT is built on a simple thesis: chronic pain, in the absence of ongoing tissue damage, is a learned danger signal. Unlearning it requires the brain to experience the sensation repeatedly while the threat appraisal is switched off. The protocol has five pillars:
- Education. The patient is taught, in detail, the neuroscience of learned pain: nociplastic pain, central sensitization, fear-avoidance loops, how the brain generates pain from safe signals. Belief that the pain is a brain signal — not a tissue alarm — is foundational.
- Gathering evidence of safety. The therapist helps the patient build a personal case that their pain is neuroplastic. Does pain move around? Come and go with stress? Appear in positions that shouldn't hurt? Did imaging show findings that don't match the pain? Each data point becomes a piece of evidence the brain can use.
- Somatic tracking. The core experiential practice. Described in detail below.
- Addressing emotional avoidance. Chronic pain often functions as a protective distraction from difficult emotions — anger at a parent, grief, fear of failure, unexpressed needs. PRT invites the patient to name and sit with those feelings.
- Reducing the pain-focused lifestyle. Slowly taking back movement, activities, and identity that pain had confiscated.
Somatic Tracking — The Core PRT Skill
Somatic tracking is a short, daily practice that trains the brain to experience pain without threat. The steps are simple; the internal stance is everything.
- Get comfortable. Sit or lie down. Close your eyes if that helps.
- Find the sensation. Bring attention to the pain. Notice where it is, its shape, its temperature, its texture. Is it a burning? A pressure? A tight band? A tingle?
- Observe with curiosity, not alarm. This is the pivot. Instead of "something is wrong, this shouldn't be here, please stop," the stance becomes "huh, interesting, I wonder what this is." You are a scientist examining a sensation, not a victim fighting an intruder.
- Remind yourself of safety. Silently or aloud: "This is a brain signal. It is not damage. I am safe. My back is fine." Say it with calm conviction, not desperation.
- Notice what changes. The sensation may shift, move, soften, or intensify. All outcomes are acceptable. If it intensifies, you are not failing — you are giving the brain a new context in which to experience the signal.
- End when ready. Most sessions last 5 to 15 minutes.
The mechanism is classical extinction learning. A sensation repeatedly paired with a safety appraisal — instead of a danger appraisal — eventually stops triggering the pain output. You cannot force the pain to leave. You can only keep changing the brain's assessment of it. Over weeks, the circuit quiets.
Somatic tracking fails when the patient does it desperately ("please work, please work"). That framing re-installs threat. The therapist spends significant time coaching tone and attitude.
Authentic Self-Expression and Avoided Emotions
Gordon and the earlier work of John Sarno both observed a pattern: chronic pain patients are often high-achieving, self-critical, approval-seeking, and uncomfortable with anger. The theory is that the brain, trying to protect the person from overwhelming or forbidden feelings, generates a physical symptom instead. The pain is "safer" than the emotion.
PRT does not require the patient to accept this as a universal truth. It does ask them to investigate whether avoided emotions are feeding the circuit. Common targets:
- Anger at a family member who the patient "can't" be angry at — a parent, spouse, or child.
- Grief that was never fully processed — a death, a divorce, a lost career.
- Resentment about caretaking roles, work obligations, or relationships.
- Fear of failure, of aging, of being seen as weak.
- Shame about needs, sexuality, or perceived inadequacy.
The intervention is not dramatic catharsis. It is gradual permission: journaling, speaking honestly with a therapist, saying "no" once this week, letting a tear through, allowing irritation without shutting it down. Patients often report that as they tolerate the real emotion, the pain signal loosens its grip. This is consistent with Lumley's EAET research (see below).
Pain Neuroscience Education (PNE)
Pain Neuroscience Education, sometimes called "Explain Pain," is the educational half of the brain-pain toolkit. It was developed by Australian physiotherapist Lorimer Moseley and neuroscientist David Butler, whose 2003 book Explain Pain (now in multiple editions) is the field's founding text. PNE is frequently delivered by physical therapists, not psychologists, and can be done in a single session or across several.
The content is straightforward:
- Pain is produced by the brain, not measured by the body. Nociceptors send danger signals; the brain decides whether to produce pain and how much.
- Hurt does not equal harm. Pain intensity is a poor predictor of tissue damage.
- Chronic pain is often the nervous system stuck in high-alert mode — central sensitization — rather than ongoing injury.
- The brain can unlearn pain the way it learned it. Graded movement, safe exposure, and education reverse the sensitization.
- Imaging findings (disc bulges, degeneration, minor tears) are common in pain-free people and are not, by themselves, proof of a pain source.
A 2021 systematic review in the Journal of Pain found that PNE combined with exercise produced modest but consistent improvements in pain and function compared with exercise alone, and markedly improved patient beliefs about pain. PNE is the educational scaffolding that makes PRT, ACT, and graded exposure work. Without it, patients keep interpreting every twinge as damage and re-activate the threat circuit.
Fear-Avoidance and Kinesiophobia
The fear-avoidance model (Vlaeyen, Linton, and others) describes the vicious loop that turns an acute injury into chronic disability:
- Acute pain happens.
- The patient catastrophizes ("this will never get better", "something is seriously wrong").
- They develop kinesiophobia — fear of movement. Bending, lifting, twisting, and exercising start to feel dangerous.
- They avoid movement. Muscles deconditioning. Posture stiffens. The nervous system becomes hypervigilant.
- Return to normal activity produces more pain than before, which confirms the fear.
- Avoidance deepens. Function shrinks. Depression and anxiety grow.
Breaking the loop requires graded exposure to movement, ideally paired with education that movement is safe. PRT, PNE, and physical therapy all attack this loop from different angles. A good chronic-pain PT does not just prescribe exercises — they spend the first visit dismantling catastrophic beliefs and giving the patient permission to move.
Screening tools like the Tampa Scale for Kinesiophobia (TSK-11) and the Fear-Avoidance Beliefs Questionnaire (FABQ) flag patients at high risk of chronic disability and are used in multidisciplinary pain clinics.
Acceptance and Commitment Therapy (ACT)
ACT (pronounced "act", not A-C-T) was developed by Steven Hayes and colleagues and applied extensively to chronic pain by Lance McCracken and Kevin Vowles. Unlike PRT, ACT does not promise pain reduction. Its thesis is subtler: suffering comes less from pain itself than from the fight against pain. By accepting unpleasant sensations as they are, while committing to action aligned with personal values, patients regain a rich life even while pain persists.
The six ACT processes, applied to chronic pain:
- Acceptance. Make room for the pain rather than struggling to eliminate it.
- Cognitive defusion. Notice thoughts ("I can't do this") as thoughts, not truths.
- Present-moment contact. Mindful attention to the here and now, instead of dwelling on the injury story or future disability.
- Self-as-context. The observer self that has pain is larger than the pain.
- Values. Name what actually matters — relationships, work, play, creativity.
- Committed action. Take steps toward those values, even with pain along for the ride.
A 2017 Cochrane review found ACT produced moderate improvements in pain interference, disability, and depression at treatment end in chronic pain populations. It is a realistic fit when pain has a structural component that cannot be reversed (advanced osteoarthritis, post-surgical neuropathy, amputation) and the goal is living well alongside it rather than eliminating it.
Mindfulness-Based Stress Reduction (MBSR)
MBSR was developed by Jon Kabat-Zinn at the University of Massachusetts Medical School in 1979, specifically to help chronic pain patients that conventional medicine had written off. The program is an 8-week structured course with weekly 2.5-hour classes plus a full-day silent retreat. Core practices include body scan meditation, sitting meditation, gentle yoga, and informal mindfulness in daily life.
The mechanism overlaps with PRT's somatic tracking but approaches it from the meditative rather than therapeutic tradition. Mindfulness trains the patient to observe sensation without reactivity. Over weeks, the brain's default threat appraisal relaxes. Functional MRI studies (Zeidan and colleagues) show that mindfulness meditation reduces pain through distinct brain mechanisms from placebo and from opioids — particularly by decreasing activity in the thalamus and increasing activity in the orbitofrontal and anterior cingulate cortices.
A 2016 JAMA randomized controlled trial compared MBSR, cognitive behavioral therapy, and usual care for chronic low back pain in 342 adults. Both MBSR and CBT produced meaningful improvements in pain and function at 26 weeks; usual care did not. MBSR courses are widely available through hospitals, community centers, and the UMass Center for Mindfulness (online and in-person). Typical cost: $500 to $800 for the 8-week program.
Emotional Awareness and Expression Therapy (EAET)
EAET, developed by psychologist Mark Lumley at Wayne State University, is the clearest research-based successor to John Sarno's clinical tradition. It targets chronic pain patients whose symptoms appear to be driven or amplified by unprocessed emotional experience — unresolved trauma, suppressed anger, conflict avoidance, or inhibition of authentic self-expression.
A typical EAET protocol runs 8 to 10 sessions and includes:
- Education linking stress, emotion, and the brain's pain output.
- Identifying avoided emotions and life stressors.
- Writing exercises (expressive writing, unsent letters) that surface and process difficult feelings.
- Imaginal dialogue — speaking honestly in imagination to a person with whom there is unresolved emotion.
- Assertive communication training — actually saying the hard thing in real life.
In a 2017 randomized trial of 230 veterans with chronic musculoskeletal pain (Lumley, Schubiner, et al.), EAET produced greater pain reduction than CBT at 6-month follow-up. A 2022 trial in fibromyalgia showed similar superiority. EAET is particularly promising for patients whose pain began or worsened around a major stressor, who carry a trauma history, or whose pain flares predictably track with interpersonal conflict. See the canonical Fibromyalgia page for the broader context.
FITS — Is Your Pain Likely Neuroplastic?
PRT practitioners use a working checklist called Features Inconsistent with Tissue Damage (FITS) to gauge whether chronic pain is likely neuroplastic. No single feature is diagnostic. The more that apply, the higher the probability the pain is brain-generated rather than driven by ongoing injury.
- Pain that moves or changes location. True tissue pathology tends to stay put.
- Pain that is inconsistent — worse on some days, better on others, with no mechanical explanation.
- Pain triggered by non-physical events: stress, specific people, anticipation, weather forecasts, weekends versus workdays.
- Pain that started during a high-stress period without a clear injury.
- Symmetric pain on both sides of the body (uncommon with a single structural lesion).
- Delayed-onset pain — not at the moment of the event but hours or a day later.
- Pain that spreads over time to new body regions.
- Multiple co-occurring symptoms: headaches, IBS-type gut symptoms, fatigue, dizziness, tinnitus, pelvic pain — suggesting a generally sensitized nervous system.
- Imaging findings that don't match the pain. MRI normal or showing only age-expected changes.
- Pain that resists every structural treatment — injections, surgery, physical therapy — or returns shortly after brief relief.
- A history of anxiety, depression, perfectionism, or trauma.
FITS is a probability tool, not a diagnosis. A patient with several positive features is a good candidate for PRT or a related approach. A patient with none should keep looking for the structural driver.
When PRT Is NOT Appropriate
PRT is not a universal pain treatment, and well-trained practitioners are explicit about this. The therapy is contraindicated or secondary when pain has an identifiable and ongoing medical driver. Red-flag categories:
- Active injury or acute inflammation. A recent fracture, sprain, surgical wound, or acute infection needs medical care, not brain training.
- Active inflammatory or autoimmune disease. Rheumatoid arthritis, ankylosing spondylitis, lupus, polymyalgia rheumatica, and inflammatory bowel disease flares produce real tissue pain that requires immunomodulation. PRT can complement but never replace disease-modifying therapy.
- Cancer pain. Tumor-related pain requires oncologic and palliative management.
- Severe neurological deficits: foot drop, progressive weakness, saddle anesthesia, bladder or bowel dysfunction — these require urgent surgical evaluation (cauda equina, cord compression).
- Unexplained systemic symptoms: fever, unintended weight loss, night sweats, elevated inflammatory markers — need a diagnostic workup first.
- Fresh imaging findings that match the pain pattern in someone who has not yet tried conservative physical treatment.
- Severe, untreated depression, psychosis, or active suicidality. These need mental-health stabilization first. See the canonical Depression page and Anxiety page.
A responsible PRT practitioner will ask you when you last had a medical workup, what imaging or blood work has been done, and will sometimes decline to treat until an obvious structural question has been ruled out. The therapy is powerful when applied to the right kind of pain. Applied to the wrong kind, it can delay needed care.
Finding a Practitioner and What It Costs
The field is young and the credentialing landscape reflects that. Three main directories and training bodies exist:
- Pain Reprocessing Therapy Center (painreprocessingtherapy.com). Maintains a practitioner directory of certified PRT therapists. Certification requires a mental-health license (LCSW, LMFT, LPC, psychologist, psychiatrist) plus completion of the PRT training program.
- Psychophysiologic Disorders Association (PPDA, ppdassociation.org). A broader umbrella organization that lists clinicians (physicians, therapists, physical therapists) trained in mind-body approaches to chronic pain, including the work of Howard Schubiner, David Clarke, and others.
- Curable Health. A well-regarded app-based self-guided program built on PRT, PNE, and expressive writing principles. Good entry point when in-person therapy is unaffordable or unavailable.
Typical session cost in the U.S. runs $150 to $300 per 50-minute session, largely out of pocket. Many PRT therapists accept insurance for the mental-health CPT codes (90791 evaluation, 90834 or 90837 psychotherapy). Sliding-scale options exist at training clinics. A full PRT course is typically 8 to 12 sessions over 1 to 3 months. Telehealth is widely available and appears to work as well as in-person delivery.
MBSR courses through hospital systems are often partially covered by insurance wellness benefits. ACT is delivered by many clinical psychologists and is typically covered at in-network mental-health rates. EAET practitioners are rarer; the closest substitute in most cities is a trauma-informed psychotherapist familiar with expressive writing and emotion-focused therapy.
Combining PRT with Medication and Other Treatment
Brain-based therapies are not anti-medication. They usually work better when the nervous system is not in screaming crisis. A reasonable combined approach:
- Sleep first. Untreated insomnia amplifies pain. Short-term trazodone, low-dose doxepin, or cognitive behavioral therapy for insomnia (CBT-I) can unlock the whole plan. See the sibling page Sleep, Exercise and Lifestyle for Chronic Pain.
- Low-dose SNRI or TCA when appropriate. Duloxetine, nortriptyline, or amitriptyline at low doses dampens central sensitization enough for the patient to engage with therapy. See Non-Opioid Medications.
- Taper opioids cautiously if relevant. Long-term opioids can paradoxically worsen central pain (opioid-induced hyperalgesia) and blunt the emotional work PRT requires. Tapers should be slow, agreed upon, and medically supervised. See Opioids for Chronic Non-Cancer Pain.
- Continue appropriate physical therapy. PNE-literate PT that emphasizes graded exposure and reassurance pairs beautifully with PRT. Avoid PT that re-instills structural fear ("your core is weak", "your pelvis is out").
- Avoid the cycle of new injections while doing PRT. Each procedure re-activates the tissue-damage story. Hold interventional procedures unless clearly indicated. See Interventional Pain.
- Treat comorbid depression and anxiety. A depressed brain cannot extinguish a pain signal. The canonical Depression and Anxiety pages cover treatment options.
Self-Guided Resources
When in-person therapy is not accessible, self-guided work can still produce meaningful change. The minimum effective kit:
- Book: The Way Out by Alan Gordon (2021) — the PRT protocol for lay readers.
- Book: Explain Pain by David Butler and Lorimer Moseley (2nd edition) — foundational PNE.
- Book: Unlearn Your Pain by Howard Schubiner — structured 4-week program combining education, expressive writing, and mind-body practices.
- Book: Full Catastrophe Living by Jon Kabat-Zinn — the MBSR manual.
- Book: The Mindful Way Workbook — accessible mindfulness for pain and depression.
- App: Curable Health — structured PRT/PNE/writing program with daily lessons and guided exercises.
- Free podcast: Tell Me About Your Pain with Alan Gordon and Alon Ziv — case-based PRT demonstrations.
- Free podcast: Like Mind Like Body (PPDA) — clinician and patient interviews across the mind-body field.
- YouTube lecture: Lorimer Moseley, "Why Things Hurt" (TEDxAdelaide) — 15 minutes, excellent PNE primer.
A reasonable self-guided sequence: watch the Moseley TED talk, read The Way Out over two weeks, begin a daily somatic tracking practice of 10 minutes, add expressive writing three times a week, and layer in MBSR-style body scans before sleep. Track your pain weekly, not daily — daily tracking often feeds the threat loop. Give the approach at least 8 to 12 weeks before deciding it isn't working.
Key Research Papers
- Ashar YK, Gordon A, Schubiner H, et al. Effect of Pain Reprocessing Therapy vs Placebo and Usual Care for Patients With Chronic Back Pain: A Randomized Clinical Trial. JAMA Psychiatry. 2022.
- Cherkin DC, Sherman KJ, Balderson BH, et al. Effect of Mindfulness-Based Stress Reduction vs Cognitive Behavioral Therapy or Usual Care on Back Pain and Functional Limitations in Adults With Chronic Low Back Pain. JAMA. 2016.
- Lumley MA, Schubiner H, Lockhart NA, et al. Emotional awareness and expression therapy, cognitive behavioral therapy, and education for fibromyalgia: a cluster-randomized controlled trial. Pain. 2017.
- Louw A, Zimney K, Puentedura EJ, Diener I. The efficacy of pain neuroscience education on musculoskeletal pain: A systematic review of the literature. J Pain. 2019.
- Hughes LS, Clark J, Colclough JA, et al. Acceptance and Commitment Therapy (ACT) for Chronic Pain: A Systematic Review and Meta-Analyses. Clin J Pain. 2017.
- Vlaeyen JW, Linton SJ. Fear-avoidance and its consequences in chronic musculoskeletal pain: a state of the art. Pain. 2000.
- Zeidan F, Martucci KT, Kraft RA, et al. Brain mechanisms supporting the modulation of pain by mindfulness meditation. J Neurosci. 2011.
Live PubMed Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on brain-based chronic pain treatments:
- Pain reprocessing therapy
- Pain neuroscience education for chronic pain
- Nociplastic pain and central sensitization
- Acceptance and commitment therapy for chronic pain
- Mindfulness-based stress reduction and chronic pain
- Emotional awareness and expression therapy for pain
- Fear-avoidance and kinesiophobia in chronic pain
- Neuroplastic pain, fibromyalgia and the brain
Connections
- Interventional Pain — Injections, Ablations, Neuromodulation
- Fibromyalgia
- Depression
- Anxiety
- Non-Opioid Medications — Gabapentinoids, SNRIs, LDN
- Sleep, Exercise, and Lifestyle for Chronic Pain
- Chronic Pain Overview
- Chronic Low Back Pain — Evidence-Based Care
- Central Sensitization and Nociplastic Pain
- Nociceptive vs Neuropathic vs Nociplastic Pain
- Complex Regional Pain Syndrome
- Opioids for Chronic Non-Cancer Pain
- Insomnia
- Chronic Fatigue Syndrome
- Central Sensitization Explained
- Low-Dose Naltrexone for Fibromyalgia
- Peripheral Neuropathy
- Inflammatory Markers