Non-Opioid Medications for Chronic Pain
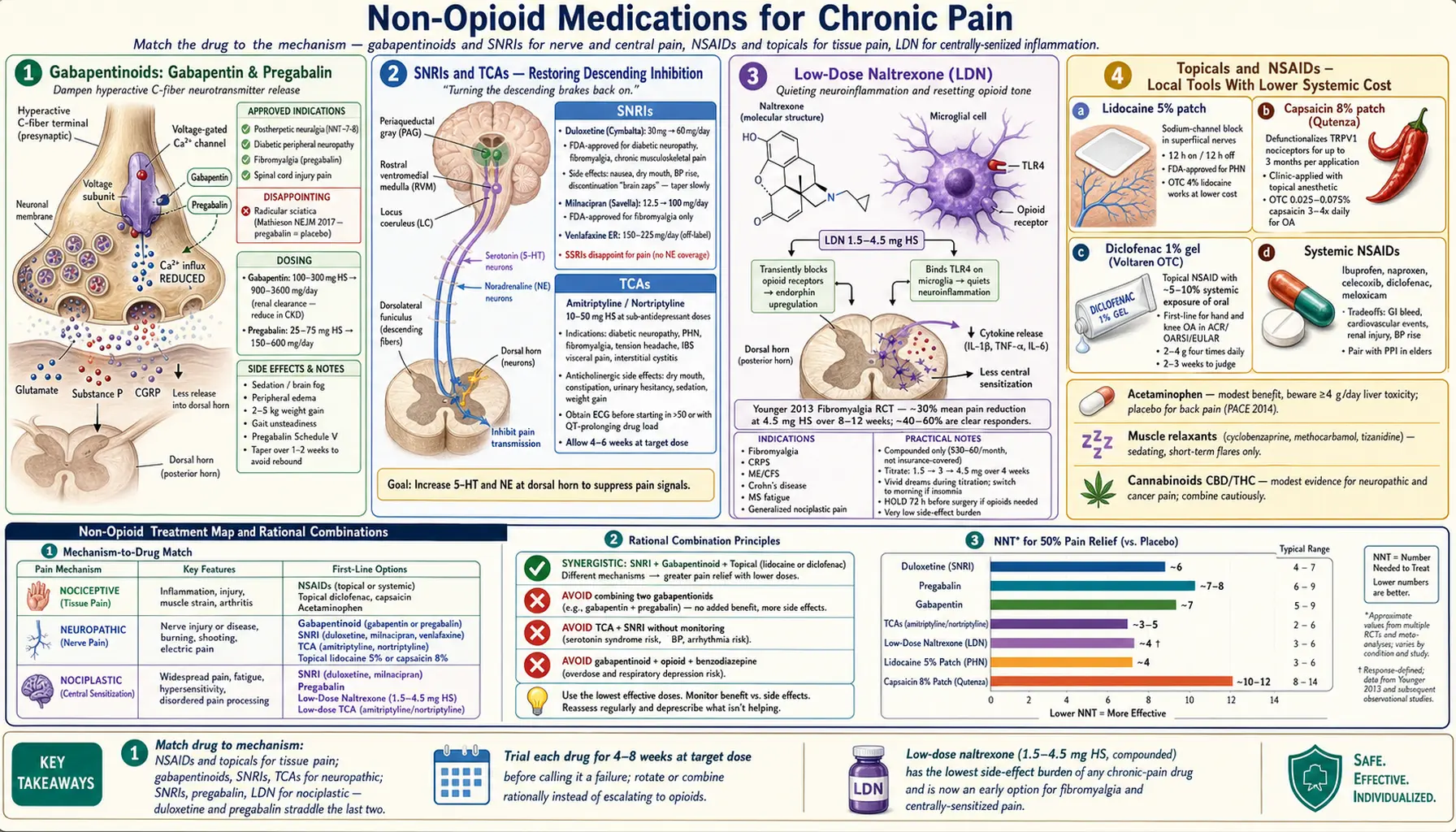
Table of Contents
- Why Start Here (Not With Opioids)
- Matching the Drug to the Pain Type
- Gabapentinoids: Gabapentin and Pregabalin
- SNRIs: Duloxetine, Milnacipran, Venlafaxine
- Tricyclic Antidepressants (TCAs)
- SSRIs — Why They Disappoint for Pain
- Low-Dose Naltrexone (LDN)
- Topical Agents: Capsaicin, Lidocaine, Diclofenac
- NSAIDs and the Cardiovascular/GI/Renal Tradeoffs
- Acetaminophen — Limits of the Workhorse
- Muscle Relaxants and Tizanidine
- Cannabinoids: CBD and THC
- Combining Drugs Rationally
- What to Ask Your Prescriber
- Key Research Papers
- Connections
- Featured Videos
Why Start Here (Not With Opioids)
If you live with chronic pain, the medication shelf looks crowded and contradictory. Your primary doctor suggests gabapentin. A neurologist adds duloxetine. A pain clinic mentions low-dose naltrexone. A friend swears by a lidocaine patch. The rheumatologist warns you about NSAIDs. Meanwhile, opioids hover in the background — promised relief shadowed by tolerance, dependence, and the mountain of harm revealed over the last two decades.
The honest summary: no single non-opioid drug reliably relieves chronic pain in most people, but several of them help a meaningful minority, and unlike opioids, their benefits tend to hold up over time without the spiral of escalating doses. The modern pain-medicine playbook is to start with the non-opioid class that best matches your pain type, accept that the first drug may not work, and rotate or combine rationally rather than defaulting to stronger and stronger opioids.
This article walks through every major non-opioid class used for chronic non-cancer pain — what they do, who they help, how they are dosed, what side effects to watch for, and what the evidence actually shows. We are not going to pretend that any of these are miracle drugs. We are going to help you have a more informed conversation with the person writing your prescriptions.
Matching the Drug to the Pain Type
Before any drug is chosen, your pain needs a category. The three clinical buckets (see the pain-type article) shape everything that follows:
- Nociceptive pain — tissue injury or inflammation (osteoarthritis, tendinopathy, acute musculoskeletal injury). Responds best to NSAIDs, acetaminophen, topical diclofenac, and physical rehabilitation.
- Neuropathic pain — damaged or dysfunctional nerves (diabetic neuropathy, postherpetic neuralgia, radiculopathy, chemotherapy-induced neuropathy, trigeminal neuralgia). Responds best to gabapentinoids, SNRIs, TCAs, lidocaine patch, capsaicin 8% patch.
- Nociplastic pain — altered central pain processing without detectable tissue or nerve damage (fibromyalgia, many chronic low-back-pain syndromes, IBS visceral pain, tension headache, CRPS in its later stages). Responds best to SNRIs, TCAs, low-dose naltrexone, and non-pharmacologic interventions including pain reprocessing therapy.
Most chronic pain patients have mixed pain — a bit of inflammation, a bit of nerve irritation, and years of central sensitization layered on top. That is why combination therapy is the rule, not the exception.
Gabapentinoids: Gabapentin and Pregabalin
What They Do
Gabapentin (Neurontin) and pregabalin (Lyrica) bind the α2δ subunit of voltage-gated calcium channels on overactive sensory neurons. By dampening calcium influx, they reduce the release of glutamate, substance P, and CGRP — the excitatory neurotransmitters that carry pain signals into the spinal cord. The net effect is quieter nerve firing.
Who Benefits
- Postherpetic neuralgia (the burning nerve pain after shingles) — FDA-approved for both drugs; number needed to treat (NNT) for 50% pain relief is roughly 7–8.
- Diabetic peripheral neuropathy — pregabalin is FDA-approved; gabapentin is a guideline-recommended first-line option.
- Fibromyalgia — pregabalin is FDA-approved; gabapentin is used off-label with similar but weaker evidence.
- Spinal cord injury pain — pregabalin is FDA-approved.
- Radicular (sciatic) pain — historically prescribed, but a NEJM trial (Mathieson 2017) found pregabalin no better than placebo for acute or chronic sciatica. Many guidelines now de-emphasize use for back pain alone.
Typical Dosing
- Gabapentin: start 100–300 mg at bedtime. Titrate by 300 mg every 3–7 days, split into three daily doses, to an effective range of 900–3600 mg/day. Reduce dose significantly if your kidneys are weak — gabapentin is cleared renally.
- Pregabalin: start 25–75 mg at bedtime. Titrate to 150–600 mg/day, split twice or three times daily. Effects usually visible within 1–2 weeks.
Side Effects You Should Actually Expect
The label lists a wall of possibilities. In real-world practice, four come up constantly:
- Sedation and "brain fog." Especially during titration and in older adults. Taking the largest dose at bedtime helps.
- Peripheral edema. Puffy ankles and feet, sometimes face. Not dangerous but uncomfortable; often dose-related.
- Weight gain. Averages 2–5 kg (4–11 lb) over a few months, more with pregabalin than gabapentin. Mechanism is partly appetite-driven, partly fluid retention.
- Dizziness and gait unsteadiness. A real fall risk in older patients, especially combined with other CNS depressants.
Abuse potential. Pregabalin is a Schedule V controlled substance in the U.S. Gabapentin is not federally controlled but is scheduled in several states. People with substance-use histories can misuse both drugs, particularly when combined with opioids or benzodiazepines; the combination increases overdose risk.
Stopping. Taper over 1–2 weeks. Abrupt discontinuation can cause rebound anxiety, insomnia, and, rarely, seizures.
SNRIs: Duloxetine, Milnacipran, Venlafaxine
What They Do
Serotonin-norepinephrine reuptake inhibitors raise synaptic levels of both neurotransmitters in the descending inhibitory pain pathways — spinal cord circuits that originate in the brainstem and normally dampen incoming pain signals. In chronic pain, these pathways are underactive. SNRIs turn them back up.
Duloxetine (Cymbalta)
The most important non-opioid pain drug in modern practice. FDA-approved for:
- Diabetic peripheral neuropathy
- Fibromyalgia
- Chronic musculoskeletal pain (including chronic low-back pain and osteoarthritis knee pain)
Typical dose: start 30 mg once daily for one week, then 60 mg once daily. Maximum 120 mg/day, though benefit rarely increases above 60 mg. Effects on pain typically appear within 2–4 weeks.
Side effects: nausea (usually transient, take with food), dry mouth, constipation, sweating, insomnia, sexual dysfunction. Blood pressure can rise modestly — check at follow-up. Discontinuation syndrome is real: skipping even one dose can produce "brain zaps," dizziness, and flu-like symptoms. Taper slowly (reduce by 30 mg every 1–2 weeks, or alternate-day dosing before stopping). Liver disease and heavy alcohol use are contraindications.
Milnacipran (Savella)
FDA-approved for fibromyalgia only. Dose: titrate from 12.5 mg once daily to 50 mg twice daily over a week. Slightly more norepinephrine-selective than duloxetine, which in theory explains its modest edge on fatigue in some patients. Side effects: nausea, headache, constipation, hot flushes, increased heart rate and blood pressure. Insurance coverage is patchier than duloxetine; generic is available.
Venlafaxine (Effexor)
Off-label for neuropathic pain and chronic musculoskeletal pain. At doses under 150 mg/day it acts mainly as a serotonin reuptake inhibitor; pain benefit requires 150–225 mg/day, where norepinephrine reuptake inhibition kicks in. Withdrawal is notoriously harsh — use extended-release formulation and taper slowly. Blood-pressure monitoring is important at higher doses.
Tricyclic Antidepressants (TCAs)
TCAs are the oldest neuropathic-pain drugs and, for many patients, still the most effective. Amitriptyline has the largest evidence base; nortriptyline (its active metabolite) is better tolerated. Both work for pain at doses far below antidepressant doses — typically 10–50 mg at bedtime, compared with 100–150 mg for depression.
Who Benefits
- Diabetic peripheral neuropathy
- Postherpetic neuralgia
- Fibromyalgia (amitriptyline is older but still guideline-recommended)
- Chronic tension-type headache and migraine prevention
- IBS visceral pain
- Interstitial cystitis / bladder pain syndrome
Dosing in Practice
- Amitriptyline or nortriptyline: start 10 mg at bedtime. Increase by 10 mg every 1–2 weeks based on tolerance. Most responders land between 25 and 50 mg. Nortriptyline causes less daytime grogginess, dry mouth, and constipation than amitriptyline.
- Allow 4–6 weeks at target dose before calling a trial a failure.
Side Effects and Safety
Anticholinergic effects dominate: dry mouth, constipation, urinary hesitancy, blurred vision, daytime sedation, weight gain. Avoid in older adults with dementia, glaucoma, or prostatic hypertrophy. QT prolongation matters at higher doses; get a baseline ECG in patients over 50 or those on other QT-prolonging drugs. Overdose is cardiotoxic, which is why these drugs are prescribed in small quantities if suicide risk is a concern.
SSRIs — Why They Disappoint for Pain
Selective serotonin reuptake inhibitors (sertraline, fluoxetine, citalopram, escitalopram, paroxetine) are excellent for depression and anxiety, both of which commonly ride alongside chronic pain. But as pain drugs in their own right, they are weak. The descending inhibitory pathway uses norepinephrine as well as serotonin, and SSRIs ignore the noradrenergic half of the equation.
The practical takeaway: if depression or anxiety is your dominant symptom and pain is secondary, an SSRI is reasonable. If pain is the primary problem, pick a drug that touches norepinephrine — a TCA, an SNRI, or both in combination. Paroxetine is the partial exception: some neuropathic-pain trials show modest benefit, likely because it has some noradrenergic activity at higher doses. Not enough to make it a first choice.
Low-Dose Naltrexone (LDN)
The Short Version
Naltrexone is an opioid-receptor antagonist used at 50 mg/day to block the effects of heroin or alcohol. At 1.5 to 4.5 mg once daily — roughly 1/10th to 1/30th of the addiction-medicine dose — it does something different. It transiently blocks opioid receptors for a few hours, triggering an upregulation of endogenous endorphins. More importantly, it binds TLR4 on microglia, the brain's resident immune cells, and quiets the neuroinflammation that drives central sensitization.
This glial mechanism is why LDN shows up in chronic-pain practice despite the counterintuitive "opioid blocker relieves pain" branding.
What the Evidence Shows
Jarred Younger and colleagues at Stanford/UAB have produced the clearest human trials: small randomized crossover studies in fibromyalgia showed ~30% mean pain reduction at 4.5 mg nightly, with the effect growing over 8–12 weeks. A subset of patients — perhaps 40–60% — are clear responders; others see nothing. See Younger's 2013 paper (DOI linked below) and subsequent reviews.
Beyond fibromyalgia, case series and small trials suggest benefit in:
- Complex regional pain syndrome (CRPS)
- Chronic fatigue syndrome / ME
- Crohn's disease (anti-inflammatory effect)
- Multiple sclerosis fatigue and spasticity
- Generalized chronic nociplastic pain
See the dedicated LDN fibromyalgia article for the full trial list and patient stories.
Practical Considerations
- Compounded only. Low-dose naltrexone is not available as a commercial tablet. A compounding pharmacy prepares 1.5 mg, 3 mg, or 4.5 mg capsules. Typical cost in the U.S. is $30–$60 per month, usually not covered by insurance.
- Start low. 1.5 mg at bedtime for 1–2 weeks, then 3 mg for 1–2 weeks, then 4.5 mg. Vivid dreams and insomnia during titration are common; switching to morning dosing fixes them for most people.
- Allow 2–3 months at 4.5 mg before calling it a failure.
- Do not combine with opioid analgesics. LDN will blunt their effect. If you need surgery or acute opioid pain control, hold LDN for 72 hours before and after.
- Very low side-effect burden compared with gabapentinoids, SNRIs, or TCAs — which is why many pain physicians now try it early rather than as a last resort.
Topical Agents: Capsaicin, Lidocaine, Diclofenac
Topical therapies deliver drug to painful tissue while keeping systemic exposure low. For localized pain, they are often under-used first-line options.
Lidocaine 5% Patch
Blocks sodium channels in superficial cutaneous nerves. FDA-approved for postherpetic neuralgia; used off-label for focal diabetic neuropathy, post-surgical nerve pain, and localized low-back pain. Apply up to three patches (covering the painful area) for 12 hours on, 12 hours off. Almost no systemic absorption; main side effect is skin irritation. Over-the-counter 4% lidocaine patches are widely available and usually adequate substitutes at lower cost.
Capsaicin 8% Patch (Qutenza)
A high-concentration patch applied in a clinic under a topical anesthetic. It defunctionalizes TRPV1-bearing nociceptive nerve fibers for up to three months per application. FDA-approved for postherpetic neuralgia and diabetic peripheral neuropathy of the feet. Expect intense burning during and briefly after the 30–60 minute application; patients often describe it as "worse before better." Low-concentration OTC capsaicin creams (0.025–0.075%) applied 3–4 times daily offer milder benefit for osteoarthritis and neuropathic pain.
Diclofenac 1% Gel (Voltaren)
A topical NSAID that is now over-the-counter in the U.S. Rubbed into joints affected by osteoarthritis — knees, hands, ankles. Delivers therapeutic drug concentration to the joint with roughly 5–10% of the systemic exposure of oral diclofenac, sharply reducing GI, cardiovascular, and renal risk. First-line for hand and knee osteoarthritis in every major guideline (ACR, OARSI, EULAR). Apply 2–4 g four times daily; allow 2–3 weeks of consistent use before judging.
NSAIDs and the Cardiovascular/GI/Renal Tradeoffs
Oral NSAIDs (ibuprofen, naproxen, meloxicam, celecoxib, diclofenac, etodolac) suppress COX-1 and COX-2 enzymes, reducing prostaglandin-driven inflammation and pain. They are highly effective for nociceptive pain and for inflammatory conditions like rheumatoid arthritis and ankylosing spondylitis. They are not the right first drug for neuropathic or nociplastic pain — they do very little for either.
The three big tradeoffs:
- Gastrointestinal. Ulcers and bleeding, especially with age > 65, prior ulcer, concurrent steroid, anticoagulant, or SSRI. Add a proton pump inhibitor if long-term use is unavoidable.
- Cardiovascular. All non-aspirin NSAIDs raise risk of myocardial infarction and stroke. Naproxen appears safest; diclofenac and rofecoxib (withdrawn) are the worst. Celecoxib is intermediate. Avoid all NSAIDs in patients with established coronary disease when possible.
- Renal. NSAIDs constrict afferent glomerular arterioles and can precipitate acute kidney injury, especially during dehydration, heart failure, or with ACE inhibitor / ARB use (the "triple whammy"). Avoid in eGFR < 30; use cautiously in eGFR 30–60.
For most chronic pain patients, the strategy is: topical diclofenac first, short courses of oral NSAIDs for flares, and serious reassessment before moving to daily long-term oral NSAID use.
Acetaminophen — Limits of the Workhorse
Acetaminophen (paracetamol) is the default "safe" analgesic, but the evidence for chronic pain is weaker than the reputation. Cochrane reviews and large trials (PACE trial 2014, LANCET) show minimal benefit for chronic low-back pain and only modest benefit for knee osteoarthritis. It is still reasonable for patients who cannot tolerate NSAIDs, and it is useful as an opioid-sparing background analgesic.
Dosing: 3 grams per day maximum for chronic use (down from the older 4 g limit), 2 grams/day maximum if you drink alcohol regularly or have any liver disease. Combination cold medicines often hide an extra 325–1000 mg — add them up before exceeding the cap. Acute acetaminophen overdose causes fulminant liver failure and is the leading cause of acute liver transplantation in the U.S.
Muscle Relaxants and Tizanidine
Cyclobenzaprine, methocarbamol, metaxalone, carisoprodol, tizanidine, and baclofen are grouped as "muscle relaxants" although their mechanisms are diverse. For acute musculoskeletal pain (a few days to two weeks), several show modest benefit, mostly through sedation rather than true muscle relaxation. For chronic pain, evidence is poor and side effects mount:
- Cyclobenzaprine (Flexeril): a TCA cousin. Sedating, anticholinergic. Use short-term only; 5 mg at bedtime is often enough.
- Carisoprodol (Soma): metabolized to meprobamate, a barbiturate-like drug. Avoid. Abuse potential is high and benefit modest.
- Baclofen: GABA-B agonist. Genuinely useful for spasticity in MS, spinal cord injury, and cerebral palsy. Limited role in non-spastic chronic pain.
- Tizanidine (Zanaflex): an alpha-2 agonist similar to clonidine. Works for spasticity, chronic tension headache, myofascial pain, and sometimes nighttime pain-driven insomnia (2–4 mg at bedtime). Watch for hypotension and liver enzyme elevation; avoid with fluvoxamine or ciprofloxacin (CYP1A2 inhibition → toxic levels).
Cannabinoids: CBD and THC
Cannabis-derived compounds are commonly used by chronic-pain patients, but the evidence is messier than marketing suggests.
- CBD (cannabidiol): non-intoxicating. Randomized trials for chronic pain are small and mixed; the best evidence is for specific rare epilepsies (prescription Epidiolex) and some inflammatory/anxiety applications. For chronic pain, CBD may help a subset, particularly when combined with sleep improvement. Quality of OTC products varies enormously — look for a certificate of analysis (COA) from an independent lab.
- THC (tetrahydrocannabinol): intoxicating. Modest evidence for chronic neuropathic pain and for chemotherapy-induced nausea (nabilone, dronabinol). Side effects include cognitive slowing, dependence, cannabinoid hyperemesis syndrome with heavy use, and cardiovascular events in susceptible patients.
- Nabiximols (Sativex, THC:CBD oral spray): approved in several countries for MS spasticity and cancer pain; not FDA-approved in the U.S.
Cannabinoids are not a primary pain therapy in current U.S. guidelines. They are a reasonable adjunct for motivated patients in states where access is legal, with full awareness of cognitive side effects and legal/employment implications.
Combining Drugs Rationally
Most chronic-pain patients end up on two or three agents. The goal is additive or synergistic mechanisms, not additive side effects. Common rational combinations:
- TCA + gabapentinoid for severe neuropathic pain (the COMBO-DN trial supports this).
- Duloxetine + gabapentin/pregabalin for diabetic neuropathy or fibromyalgia.
- LDN + SNRI for fibromyalgia (different mechanisms, non-overlapping side effects).
- Topical diclofenac + acetaminophen for osteoarthritis.
- Lidocaine patch + oral neuropathic drug for focal neuropathic pain.
Combinations to avoid or use with care: TCA + SNRI (serotonin syndrome risk, additive anticholinergic load), gabapentinoid + opioid + benzodiazepine (respiratory depression), multiple sedating agents (falls in older adults). Always show your complete medication list — including OTC, supplements, and cannabis — to every prescriber.
What to Ask Your Prescriber
- "Which pain type do you think I have — nociceptive, neuropathic, nociplastic, or mixed?" The answer shapes everything downstream.
- "What is the target dose, and how long until we know if this drug is working?" Most of these drugs need 2–6 weeks at a therapeutic dose, not just any dose.
- "What is the plan if this does not work — switch or add?" Have the next step mapped before you start the first.
- "What side effects am I most likely to feel, and which ones should prompt a call?"
- "How will we taper this drug if we decide to stop?" Do not let an SNRI, gabapentinoid, or TCA be prescribed without a taper plan on the record.
- "Is a topical option reasonable for my pain pattern?" Focal pain is often under-treated topically.
- "Can we consider low-dose naltrexone?" Many primary-care physicians are unfamiliar; pain specialists and functional-medicine clinicians prescribe it routinely.
Key Research Papers
- Finnerup NB, et al. Pharmacotherapy for neuropathic pain in adults: a systematic review and meta-analysis. Lancet Neurol. 2015.
- Mathieson S, et al. Trial of Pregabalin for Acute and Chronic Sciatica. N Engl J Med. 2017.
- Younger J, Noor N, McCue R, Mackey S. Low-dose naltrexone for the treatment of fibromyalgia: findings of a small, randomized, double-blind, placebo-controlled, counterbalanced, crossover trial. Clin Rheumatol. 2014.
- Brown N, Panksepp J. Low-dose naltrexone for disease prevention and quality of life. J Clin Pharm Ther. 2015.
- Williams CM, et al. Efficacy of paracetamol for acute low-back pain (PACE): a double-blind, randomised controlled trial. Lancet. 2014.
- Tesfaye S, et al. Duloxetine and pregabalin: high-dose monotherapy or their combination? The COMBO-DN study. Pain. 2013.
- Enke O, et al. Anticonvulsants in the treatment of low back pain and lumbar radicular pain: a systematic review and meta-analysis. CMAJ. 2018.
- Moore RA, et al. Amitriptyline for neuropathic pain in adults. Cochrane Database Syst Rev. 2015.
Live PubMed Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on non-opioid chronic pain pharmacotherapy:
- Gabapentinoids for neuropathic pain
- Duloxetine for chronic pain and fibromyalgia
- Milnacipran for fibromyalgia
- TCAs for neuropathic pain
- Low-dose naltrexone and chronic pain
- Capsaicin 8% patch for neuropathic pain
- Topical diclofenac for osteoarthritis
- NSAID cardiovascular and renal risk
Connections
- Nociceptive vs Neuropathic vs Nociplastic Pain
- Low-Dose Naltrexone for Fibromyalgia
- Chronic Pain Overview
- Fibromyalgia
- Peripheral Neuropathy
- Complex Regional Pain Syndrome
- Central Sensitization and Nociplastic Pain
- Interventional Pain — Injections, Ablations, Neuromodulation
- Pain Reprocessing Therapy and PNE
- Chronic Low Back Pain — Evidence-Based Care
- Sleep, Exercise, and Lifestyle for Chronic Pain
- Opioids for Chronic Non-Cancer Pain
- Insomnia
- Depression
- Anxiety
- Chronic Fatigue Syndrome
- Migraine
- Arthritis