Compression Garments and the CHOP/Dallas Exercise Program for POTS
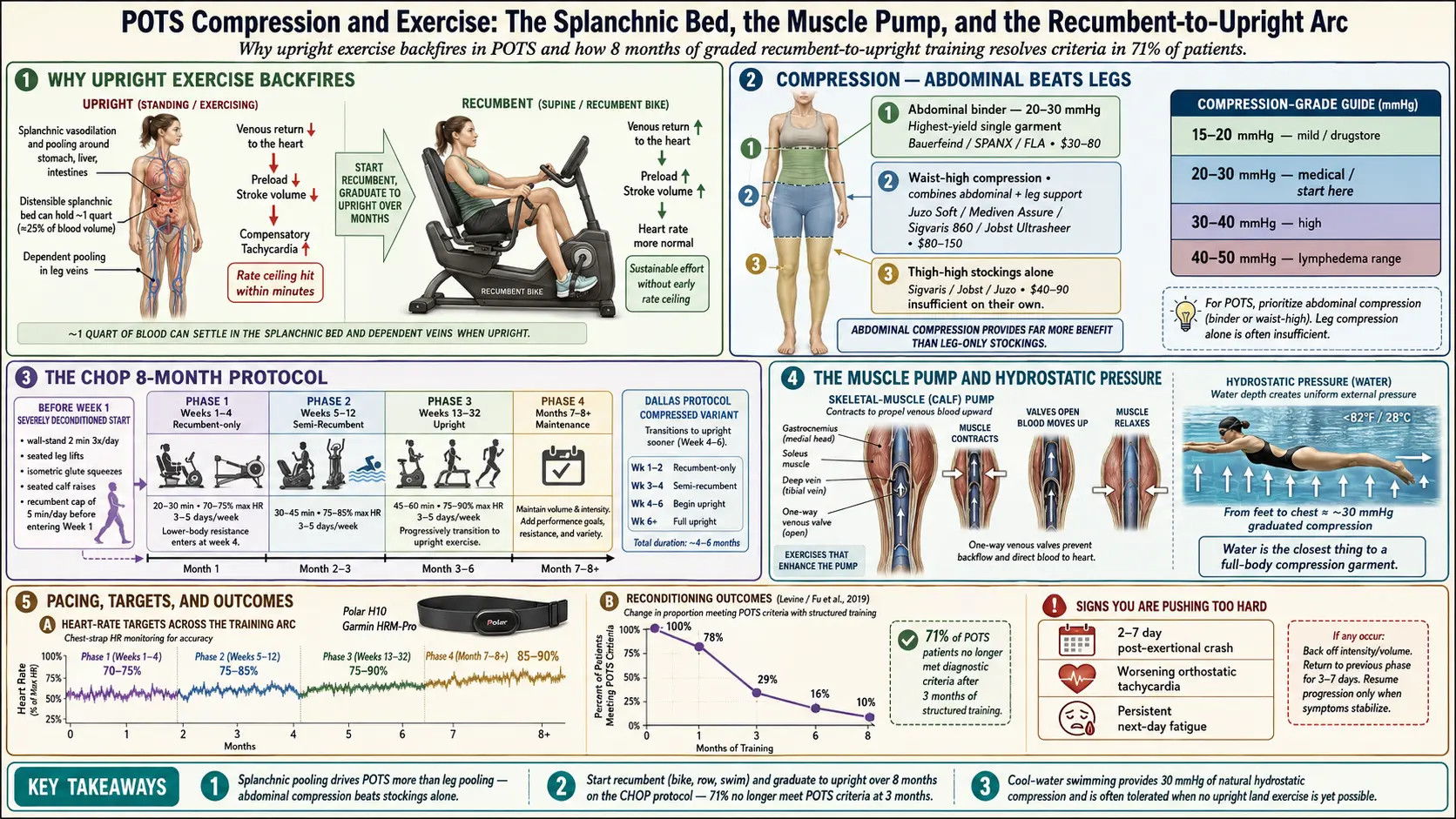
Table of Contents
- Why POTS Makes Normal Exercise Backfire
- Compression 101
- Compression Grades
- Garment Types & Pros/Cons
- Where to Buy
- The CHOP Protocol
- The Dallas Protocol
- Starting When You’re Severely Deconditioned
- Resistance Training Without Heart Rate Spikes
- Swimming — The Special Case
- Heart Rate Targets and Pacing
- Signs You’re Pushing Too Hard
- Integration with Other Treatments
- Realistic Timeline
- Key Research Papers
- Research Papers
- Connections
- Featured Videos
1. Why POTS Makes Normal Exercise Backfire
If a cardiologist told you to “just get more exercise” and handed you a walking prescription, they skipped a step. In POTS, standing up is already the challenge. Adding upright aerobic work — brisk walking, running, the elliptical, hiking uphill — stacks gravitational stress on top of autonomic dysfunction, and the predictable result is worse tachycardia, worse presyncope, and a post-exertional crash that can take 2 to 7 days to resolve.
This isn’t deconditioning you’re imagining. It’s a real cardiovascular constraint: blood pools in the legs and splanchnic bed on standing, venous return drops, and the heart compensates with rate. Add exercise and the rate ceiling gets hit within minutes.
The fix is not to stop moving. The fix is to start recumbent — lying down or semi-reclined, where gravity doesn’t fight venous return — and graduate to upright work over months. Done correctly, this reverses the deconditioning without triggering crashes. The CHOP and Dallas protocols described below are the two best-studied versions.
2. Compression 101
Compression garments work by mechanically opposing venous pooling. External pressure on the legs and abdomen keeps blood moving back up toward the heart instead of settling in the lower body every time you stand. The effect on heart rate on standing can be measurable within minutes of putting a garment on.
Here is the counterintuitive part most patients miss: abdominal compression matters more than leg compression for POTS. The dominant venous pooling in POTS is not in the calves — it’s in the splanchnic vasculature, the large, distensible venous bed surrounding the stomach, liver, and intestines. That region holds roughly a quart of blood that can drop out of circulation on standing.
Patients who buy thigh-high stockings alone often report mild or no improvement. The same patients adding an abdominal binder frequently report the single biggest symptom reduction of any intervention they’ve tried. If you’re going to buy one garment first, make it an abdominal binder.
3. Compression Grades
Compression is measured in millimeters of mercury (mmHg) — the pressure applied at the ankle, tapering upward. Four grades exist:
- 15–20 mmHg — mild, everyday “support” range. Found at drugstores. Minimal benefit for POTS.
- 20–30 mmHg — moderate medical grade. The most POTS-effective range and the default starting point. Most insurance plans cover this tier with a prescription.
- 30–40 mmHg — high medical grade. Reserved for severe cases or visible leg pooling/edema. Harder to put on.
- 40–50 mmHg — used for chronic venous insufficiency and lymphedema. Overkill for POTS and often unwearable without donning aids.
Start at 20–30 mmHg. Move up only if the moderate grade is well-tolerated but the symptom control isn’t enough.
4. Garment Types & Pros/Cons
Abdominal Binder
A wide elastic wrap or SPANX-style panel covering the lower abdomen. Brands include Bauerfeind, Boa Fit, SPANX high-waisted shapewear, and medical binders from FLA Orthopedics. Approximates 20–30 mmHg of splanchnic compression. $30–$80. This is the single best garment for POTS because it targets the splanchnic pooling that matters most. Easy to wear under regular clothes.
Thigh-High Stockings
Target leg pooling specifically. Require a silicone ride-up band to stay up or they roll down in an hour. Quality brands: Sigvaris, Jobst, Juzo, Mediven. $40–$90/pair. Useful addition for patients with visible lower-extremity pooling but insufficient on their own for most POTS patients.
Waist-High Pantyhose
The combination garment: abdominal panel plus full leg compression. Best overall coverage and strongest single-garment effect. Look at Juzo Soft, Mediven Assure, Sigvaris 860, Jobst Ultrasheer waist-high. $80–$150/pair. Hottest to wear. The default recommendation of POTS cardiology clinics when a patient can tolerate one garment all day.
Shorts-Style Compression
Athletic compression shorts from Under Armour, 2XU, CW-X, Skins. Lower mmHg (roughly 10–15) but breathable and heat-tolerant. Best choice for exercise sessions and hot weather where medical-grade compression becomes intolerable.
Lower-Leg Socks Only
The least-effective option for POTS because they miss the splanchnic bed entirely. Fine for a long flight or standing shift at work; not a primary POTS intervention.
5. Where to Buy
Insurance coverage varies by plan and by state. A prescription is typically not required below 30 mmHg, but a script makes reimbursement easier if you have medical-grade coverage.
- Medical supply stores — LegSmart, Ames Walker, BrightLife Direct, Compression Stockings Unlimited. Best selection and published size charts.
- Local brick-and-mortar medical supply — get fitted in person once. A trained fitter takes four measurements (ankle, calf, thigh, length) and picks a size more precisely than any online chart. After the first fitting you can reorder the same size online.
- Amazon — fine for a first generic pair to test tolerance; returns are easy if sizing is wrong.
- Insurance DME benefit — with a prescription and diagnosis code, many plans cover 2–4 pairs per year. Ask the prescriber to write “for POTS, orthostatic intolerance” with the ICD-10 code.
6. The CHOP Protocol
The Children’s Hospital of Philadelphia (CHOP) protocol is an 8-month graded exercise program originally designed for adolescents with POTS and since adapted widely for adults. It is the best-studied rehabilitation program in the POTS literature. The Fu and Levine studies out of Dallas showed that roughly 71% of POTS patients no longer met diagnostic POTS criteria after 3 months of structured training.
Recumbent-Only Phase (Weeks 1–4)
Recumbent bike or rowing machine only. 20–30 minutes per session, 3–5 days per week. Target 70–85% of max HR, staying on the lower end at first. Rowing counts as recumbent because the torso stays near-horizontal to the pump. No upright work of any kind.
Semi-Recumbent Phase (Weeks 5–12)
Transition to semi-recumbent bike, elliptical, and swimming. Sessions lengthen to 30–45 minutes. Frequency stays at 3–5 days. Heart rate target creeps up to 75–85% max HR.
Upright Phase (Weeks 13–32)
Upright bike, treadmill walking, and eventually jogging. This phase is where durable reconditioning happens — the cardiovascular system re-learns upright tolerance. By the end, many patients are running 20–30 minutes continuously.
Resistance Training
Lower-body resistance — squats, leg press, leg curls — enters at week 4, twice weekly. Upper-body resistance can start from week 1 because upper-body lifts done seated don’t impose orthostatic load.
7. The Dallas Protocol
The Dallas protocol, developed by Benjamin Levine and colleagues at UT Southwestern, is the CHOP template compressed. Same recumbent-to-upright arc but with the transition to upright exercise at week 4–6 instead of week 12. It works for patients who tolerate the earlier phases easily and want faster return to function.
It is not for everyone. Patients with severe baseline symptoms, hyperadrenergic features, or post-viral POTS tend to do better on the slower CHOP timeline and often crash if pushed onto Dallas pacing. If in doubt, run CHOP.
8. Starting When You’re Severely Deconditioned
If five minutes on a recumbent bike is currently beyond reach, you are not failing the program — you’re starting before the program. Build a pre-CHOP base like this:
- Passive standing tolerance: stand with your back against a wall, heels a few inches out, for 2 minutes, 3 times per day. Build by 30 seconds per week.
- Seated leg lifts: sit upright and straighten each leg slowly, 10 reps per side, twice daily.
- Isometric glute squeezes: at a desk, squeeze and hold for 5 seconds, release, repeat 10 times, twice daily. Activates the muscle pump without cardiovascular load.
- Calf raises seated: push up onto the balls of the feet from a chair, 15–20 reps.
- Recumbent ceiling: cap at 5 minutes on a recumbent bike, pedaling at a conversational pace, once daily. Add one minute per week only when the previous duration is fully symptom-neutral.
When you can hit 20 minutes of recumbent cycling at 70% max HR without a post-exertional crash, you’re ready to enter Week 1 of CHOP.
9. Resistance Training Without Heart Rate Spikes
Resistance work reverses muscle loss and rebuilds the calf and glute muscle pumps that propel venous blood upward on standing. Done correctly it doesn’t spike heart rate.
- Leg press — seated, fully supported, hits quads and glutes without orthostatic stress.
- Seated hamstring curl — posterior chain, minimal blood pressure swing.
- Calf raises — the most important single exercise for the calf pump. Do them seated first, then standing as tolerance builds.
- Seated rows and chest press — upper-body work, safe from day one.
Avoid overhead presses and any maneuver involving a sustained Valsalva (breath holding on exertion) in the first months — they can trigger symptom flares. Target 8–15 reps, 2–3 sets, 2–3 times per week, moderate weight, controlled tempo.
10. Swimming — The Special Case
Water is the closest thing to a full-body compression garment that exists. Hydrostatic pressure on a submerged body approximates 30 mmHg of graded compression from the feet up to the chest. That’s why swimming is uniquely tolerated by POTS patients, often at stages when no land-based upright exercise is possible.
Water walking, water aerobics, and lap swimming all work. Cool water (under 82°F / 28°C) is preferred because POTS is heat-sensitive and warm pools trigger vasodilation. Avoid hot tubs entirely. If your local pool runs warm, swim early in the day before it heats up, or look for a lap-only pool that maintains cooler temperature.
11. Heart Rate Targets and Pacing
Buy a chest-strap heart rate monitor — the Polar H10 or Garmin HRM-Pro are the accurate options. Wrist-based optical monitors lag and smooth data in ways that matter for POTS pacing.
Calculate max heart rate as 220 minus age, then pace by phase:
- Weeks 1–4: 70–75% max HR. Aerobic base. No bursts, no intervals, no spikes.
- Weeks 5–12: 75–85% max HR. Sustained moderate intensity.
- Weeks 13+: 85–90% max HR during peak intervals, with recovery valleys in between.
If your monitor shows a spike above the phase ceiling, pull back until it drops. The goal isn’t to “push through” — pushing through is exactly what produces the post-exertional crashes the program is built to avoid.
12. Signs You’re Pushing Too Hard
Watch for these signals in the 24–48 hours after a session:
- Post-exertional malaise (PEM) lasting more than 24 hours — the single clearest signal of overreach.
- Increased orthostatic symptoms the next morning — worse dizziness, presyncope, brain fog on first standing.
- Resting heart rate elevated by 10 bpm or more compared to your baseline on the following morning.
- Sleep disruption — trouble falling asleep, middle-of-night wakings, unrefreshing sleep.
If any of these show up: back off intensity by 50% for 3–5 days, then rebuild from a lower starting point. One overreach episode doesn’t undo your progress — ignoring the signal and pushing again does.
13. Integration with Other Treatments
Exercise is one layer in a stack, not a standalone. Integrate it with everything else you’re doing:
- Wear compression during every session. Shorts-style for heat tolerance, waist-high if you can wear it.
- Salt and fluid pre-load. 500 mL of water with electrolytes 30 minutes before exercise. See Salt & Hydration Protocol.
- Time medications to exercise. If you take midodrine, dose so peak plasma concentration (roughly 60–90 minutes post-dose) aligns with the start of your session. See Medications Guide.
- Cool the room. POTS is heat-intolerant. Train in air conditioning or early morning.
- Avoid exercising right after eating. Splanchnic blood flow spikes after a meal and stacks with exercise stress.
14. Realistic Timeline
Honest expectations matter. Most POTS patients see measurable improvement at 8–12 weeks — lower standing heart rate, longer symptom-free standing, fewer presyncopal episodes. Significant functional recovery arrives at 6–9 months, which is when many patients describe feeling genuinely different rather than just slightly better.
Relapses happen. A viral infection, a week of travel, a surgery, a bad menstrual cycle can all knock progress back by weeks. The key insight: patients with an established fitness base recover from setbacks far faster than patients who are rebuilding from zero. This is the long-term argument for never fully stopping — even a 10-minute recumbent session twice a week during a flare preserves enough base to resume quickly when the flare passes.
15. Key Research Papers
- Fu Q, et al. Exercise training versus propranolol in the treatment of postural orthostatic tachycardia syndrome. Hypertension. 2011;58(2):167-175.
- Raj SR, et al. Postural tachycardia syndrome (POTS). Circulation. 2013.
- Sheldon RS, et al. 2015 Heart Rhythm Society expert consensus statement on the diagnosis and treatment of POTS, inappropriate sinus tachycardia, and vasovagal syncope. Heart Rhythm. 2015.
- Fu Q, Levine BD. Exercise in the postural orthostatic tachycardia syndrome. European Heart Journal. 2018.
16. Research Papers
Curated PubMed topic searches — each link opens a live query so you always see the most recent literature.
- PubMed: POTS exercise training
- PubMed: CHOP protocol for POTS
- PubMed: Recumbent exercise in orthostatic intolerance
- PubMed: Compression garments for POTS
- PubMed: Abdominal compression for orthostatic intolerance
- PubMed: POTS deconditioning reversal
- PubMed: Levine POTS exercise studies
- PubMed: Swimming and orthostatic intolerance
Connections
- POTS Overview
- Medications Guide
- Salt & Hydration Protocol
- POTS Subtypes
- Tilt-Table & NASA Lean Test
- Vagus Nerve & Autonomic Retraining
- POTS-MCAS-EDS Triad
- Low-Dose Naltrexone for POTS
- MCAS
- Fibromyalgia
- Chronic Fatigue Syndrome
- Ehlers-Danlos Syndrome
- POTS Diet
- Magnesium
- Exercise Pacing and Graded Movement
- Pacing and Energy Envelope
- Physical Therapy and Joint Protection