Exercise and PT Protocol for Ankylosing Spondylitis
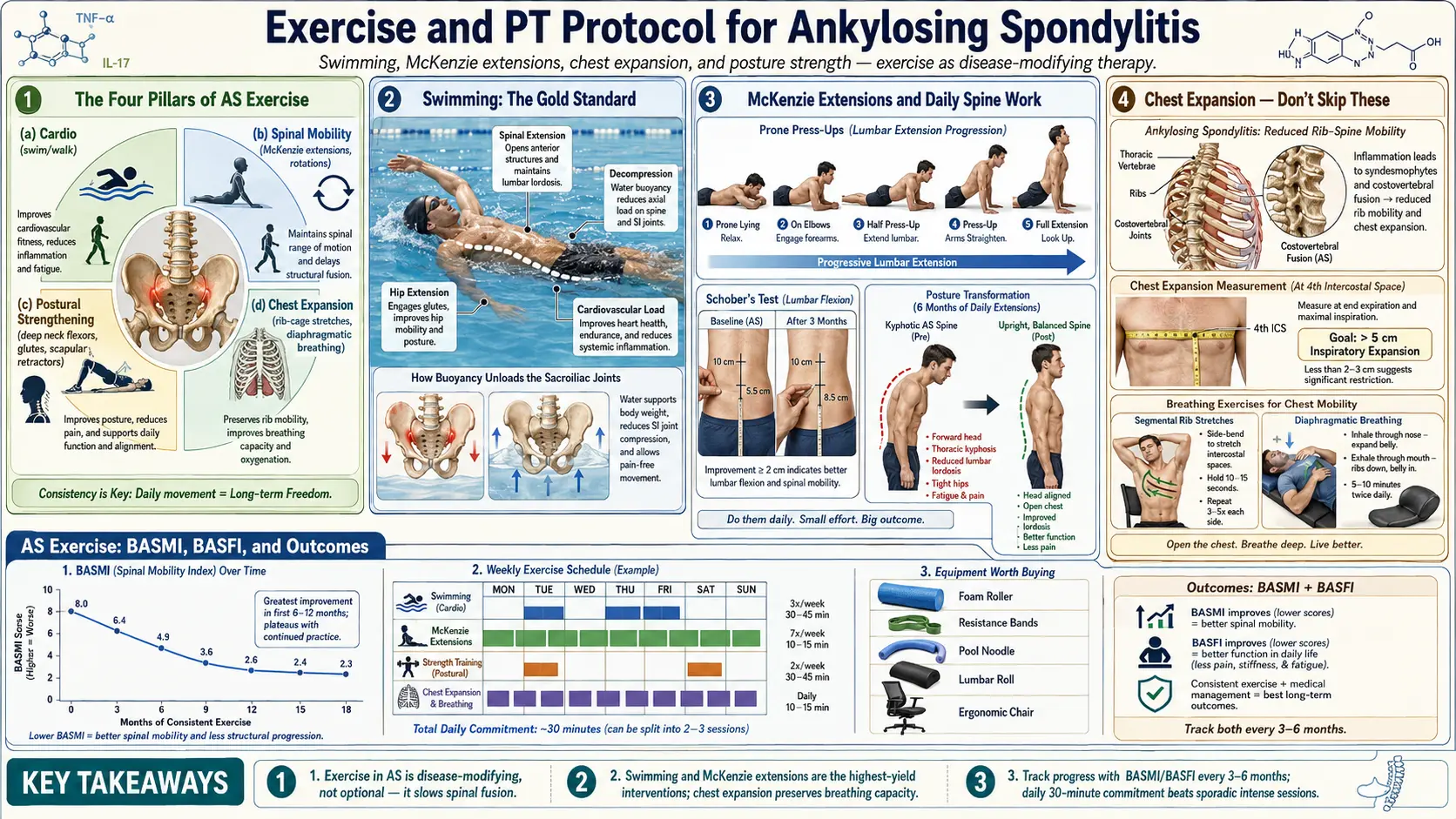
Table of Contents
- Why Exercise Is Disease-Modifying in AS
- The Four Pillars of AS Exercise
- Swimming — The Gold Standard
- McKenzie Extensions — Daily Spine Work
- Posture-Correction Strength Work
- Yoga for AS
- Weekly Schedule — McKenzie + Strength + Swim
- Chest Expansion Exercises — Don’t Skip These
- Track Your Progress — BASMI / BASFI
- When You’re in a Flare
- High-Impact Activities — Use With Caution
- Equipment Worth Buying
- Working With a Physical Therapist
- Workplace Strategies
- Realistic Timeline
- AS Exercise Communities & Apps
- Key Research Papers
- Research Papers
- Connections
- Featured Videos
1. Why Exercise Is Disease-Modifying in AS
Most forms of arthritis improve with rest. Ankylosing spondylitis does the opposite. AS is a "use-it-or-lose-it" disease, and that phrase is not a motivational slogan — it is a structural fact about how inflamed axial tissues behave when they stop moving.
When an inflamed enthesis or facet joint goes unused, the chronic inflammation drives new bone formation along the margins. Over months and years, those bony bridges (syndesmophytes) extend, meet, and fuse adjacent vertebrae. Inactivity accelerates the process. Movement — specifically, extension — disrupts it.
Long-term cohort studies consistently show that AS patients who exercise regularly retain spinal mobility and functional independence for decades longer than sedentary patients, even when baseline disease severity is matched. Exercise is not an adjunct to biologic therapy; it is a parallel disease-modifying intervention. Every inch of spinal extension you preserve is an inch of independence you keep.
The mental frame to adopt: you are not "working out." You are performing a structural intervention against a progressive fusion process. Skip a week of swimming and you are not just losing fitness — you are giving inflamed tissue a window to calcify.
2. The Four Pillars of AS Exercise
A complete AS program rests on four mutually reinforcing categories. Drop any one and the others lose value.
- Extension and mobility — keep the spine moving in all directions, with a bias toward extension, which is the range AS steals first.
- Cardiovascular — low-impact, sustained activity to preserve aerobic capacity as chest-wall compliance declines.
- Strength — postural muscles especially: core, back extensors, rhomboids, mid-traps, glutes.
- Deep breathing — costovertebral and sternocostal joints are vulnerable to fusion; expansion exercises are the only thing that keeps them mobile.
If you only have 20 minutes a day, split it: 10 minutes of extension/mobility work plus 10 minutes of either swimming, strength, or breathing. Rotate the second block across the week.
3. Swimming — The Gold Standard
If you do one thing for AS, swim. Every rheumatologist and AS-experienced PT will point you at the pool first, and the reasons are mechanical, not sentimental.
Why it works
Buoyancy offloads the spine, which means you can move through ranges that are painful on land. Water provides graded resistance in all directions, training musculature without concentric-eccentric shock. Extension-dominant strokes actively reverse the flexion pattern AS imposes over years of hunching.
Best strokes
- Backstroke — the single best AS stroke. The spine is held in extension, shoulders open, neck neutral to slightly extended.
- Elementary backstroke — slower, gentler on shoulders, ideal during flares.
- Sidestroke — spares the neck, works obliques.
Strokes to avoid (or modify)
- Breaststroke — demands heavy cervical flexion and extension cycling that can aggravate an already stiff neck.
- Freestyle — acceptable if you can rotate to breathe without pain; use a snorkel if neck rotation is limited.
Frequency, temperature, tools
3–5 sessions per week, 30–45 minutes each. Warm water (82–88°F / 28–31°C) is ideal — cold pools increase stiffness and can trigger spasm. Hydrotherapy pools kept at 92°F are gold-standard during flares.
Useful tools: a pull buoy to isolate upper body, a kickboard for legs-only work, and short fins that encourage hip extension without demanding ankle range.
4. McKenzie Extensions — Daily Spine Work
The McKenzie Method, developed by New Zealand physiotherapist Robin McKenzie, uses repeated end-range extension to decompress spinal structures. For AS patients, it doubles as a direct counter to flexion-dominant fusion.
The four core movements
- Press-ups (prone extensions) — lie face down, hands flat under shoulders, press the chest up while the pelvis stays grounded. Hold 2–3 seconds. 10 reps.
- Standing backbends — hands on lower back, feet shoulder-width, lean back gently into extension. 10 reps. Excellent desk-break movement.
- Cat-cow — four-point position, alternate between arched-back extension and rounded-back flexion. Moves every segment through full range. 10 cycles.
- Foam roller extension — lie supine with a foam roller across the upper-mid back, arms overhead, drape the thoracic spine over the roller. Move the roller inch by inch from mid-back to scapular spine.
Frequency: daily, twice a day ideal — once on waking (to break the morning stiffness cycle) and once before bed. Total time: 10–15 minutes. This is the cheapest, highest-leverage thing you will ever do for your spine.
5. Posture-Correction Strength Work
AS biases the body toward thoracic kyphosis, forward head, and anterior pelvic tilt. Strength training fights every one of those vectors — if you choose the right lifts.
Upper body (postural)
- Rhomboid and mid-trap rows — with bands, cables, or a low-row machine. Retract shoulder blades hard at the end range.
- Face pulls — rope attachment, pull toward forehead, externally rotate. The single best posture corrective for desk workers.
- Wall angels — slow "snow angels" pressed flat against a wall. Merciless diagnostic of thoracic mobility.
Core without spinal flexion
- Dead bug — supine, opposing arm and leg extensions. Deep core without crunching.
- Bird dog — quadruped, opposing arm and leg out, spine neutral. Trains anti-rotation.
- Plank — short holds (20–40 sec) with ribs pulled down; avoid sagging lumbar.
Lower body + posterior chain
- Glute bridges — opens hips, fires glutes, counters anterior pelvic tilt.
- Hip flexor stretches (couch stretch) — one shin up a wall, front foot flat, upright torso. Hold 90 seconds per side. Tight hip flexors pull the pelvis forward and worsen lumbar hyperlordosis; desk workers should do this daily.
- Quad stretches — same logic; tight quads tilt the pelvis anteriorly.
Frequency: 3 sessions per week, 30–45 minutes. Moderate loads, slow tempo, full range. Skip heavy spinal loading until you have a stable posture baseline.
6. Yoga for AS
Yoga is a near-perfect AS modality when matched to the right style and taught with proper modifications. Matched to the wrong style it is a fast way to inflame an SI joint.
Best poses
Extension-dominant, chest-opening shapes: cobra, upward-facing dog, sphinx, bridge, fish pose, locust, camel, and — once mobility permits — king cobra and wheel. These actively oppose the AS flexion pattern.
Modify or avoid
- Aggressive forward folds — progressive only; never force the range.
- Binding twists — bound revolved poses stress the sacroiliac joints, which are already the epicenter of AS inflammation.
- Hot yoga — dehydration plus aggressive flows is a poor fit for AS.
- Power vinyasa — chaturanga repetitions load the shoulders and compress the cervical spine.
Props, styles, teachers
Use props liberally — blocks, bolsters, straps, chairs — to avoid compensatory patterns. Best styles: Iyengar (prop-heavy, precise alignment), gentle Hatha, and restorative. Frequency: 2–3 sessions per week. Before you book a class, ask the teacher about experience with AS or inflammatory arthritis, and tell them before the first class what you are working with.
7. Weekly Schedule — McKenzie + Strength + Swim
Here is a concrete weekly template that balances all four pillars. It is the AS equivalent of the Dallas/CHOP protocol physical therapists build individually for patients.
- Monday: 30-min swim (backstroke focus) + 10-min morning McKenzie.
- Tuesday: strength training (upper back + core: rows, face pulls, dead bug) + evening McKenzie.
- Wednesday: 30-min swim or yoga (Iyengar) + morning and evening McKenzie.
- Thursday: strength training (lower body + posterior chain: bridges, hip flexor stretches, bird dog) + evening McKenzie.
- Friday: yoga (restorative or gentle Hatha) + morning McKenzie.
- Saturday: long swim (45–60 min) or a hike on soft terrain.
- Sunday: rest day — McKenzie only, morning and evening.
Notice that McKenzie appears every day. That is the non-negotiable core of the program. The swim/strength/yoga rotation can flex around your life; the daily extension work cannot.
8. Chest Expansion Exercises — Don’t Skip These
Costovertebral and sternocostal joint fusion is one of the most under-discussed consequences of AS. When the ribs stop moving, vital capacity drops, exercise tolerance collapses, and pneumonia risk rises. Breathing work is not optional.
The drills
- Diaphragmatic breathing — supine, hand on belly, inhale 4 seconds expanding the belly, exhale 6 seconds. 10 cycles, twice daily.
- Rib-cage expansion with a band — loop a resistance band around the lower chest, inhale against the band resistance, exhale and release. 10 reps.
- Thoracic rotation — seated book openers — side-lying, knees bent, top arm "opens" like a book, tracking with the eyes. 10 per side.
- Supine windshield wipers — knees bent up, feet together, drop knees side to side while keeping shoulders flat.
Measure monthly
Take a tape measure at nipple level (fourth intercostal space). Record deep inhale minus full exhale. Normal adult expansion is greater than 5 cm. AS progression is suspected below 2.5 cm. A falling monthly number is an early warning that costovertebral joints are tightening — well before spirometry changes show up.
9. Track Your Progress — BASMI / BASFI
You cannot manage what you do not measure. Three validated instruments, all free to calculate, give you an objective read on disease trajectory.
- BASMI (Bath Ankylosing Spondylitis Metrology Index) — a 5-measure spinal mobility score: cervical rotation, tragus-to-wall distance, lumbar side flexion, lumbar forward flexion (modified Schober), and intermalleolar distance. Scored 0–10; higher is worse. Have a PT measure every 6 months.
- BASFI (Bath Ankylosing Spondylitis Functional Index) — 10-question patient-reported functional assessment. Answer on a 0–10 scale; average the scores. Track monthly.
- BASDAI (Bath Ankylosing Spondylitis Disease Activity Index) — 6 questions on fatigue, pain, stiffness. The go-to activity score for rheumatology visits.
Free online calculators exist for all three — print the forms, date them, and bring the trendline to your rheumatology appointments. A flat or improving BASMI over 12 months while on your current regimen is the best evidence your program is working.
10. When You’re in a Flare
The worst thing you can do during a flare is stop moving entirely. Deconditioning sets in within days, and the inflamed tissues you "rest" are the same ones that fuse when still.
- Keep moving — gently. Walking, warm-water swimming, and restorative yoga stay on the menu.
- Reduce load: roughly 30% of normal duration, 50% of normal intensity.
- Heat before exercise — heating pad on the lower back for 10 minutes, or a warm shower — dramatically reduces stiffness.
- Ice after acute flare sessions — 10–15 minutes on the most inflamed area.
- Extend the morning routine: 15–20 minutes of gentle stretching before getting out of bed. See Morning Stiffness Management for the full wake-up protocol.
11. High-Impact Activities — Use With Caution
Some activities are neither recommended nor forbidden — they sit in a gray zone that depends on your disease stage, fusion extent, and symptom pattern.
- Running — possible, but pounding stresses the sacroiliac joints. Choose soft surfaces (trails, track), replace shoes every 300–500 miles, and add a short walk-warmup.
- Contact sports — avoid entirely if cervical spine is involved. A fused cervical spine fractures rather than flexes under impact, and C-spine fractures in AS are disproportionately fatal.
- Weightlifting — moderate loads are excellent. Avoid heavy spinal compression (loaded back squats, heavy conventional deadlifts) in advanced disease; trap-bar or goblet variants are safer.
- Cycling — the flexed road-bike posture is the exact shape AS is trying to lock you into. Upright bikes, recumbents, or hybrid geometry with a raised handlebar stack are far better than drops.
12. Equipment Worth Buying
You do not need a home gym. You need a short list of cheap tools that remove friction from daily practice.
- Pull buoy + kickboard — about $20 combined.
- Foam roller — a basic 36-inch high-density roller ($25–$35) or a RumbleRoller for more aggressive release.
- Resistance bands — TheraBand or Bodylastics sets cover rows, face pulls, and rib-expansion drills.
- Yoga blocks + strap — around $20; makes half the poses accessible that would otherwise be forced.
- Stability ball — alternate with your chair 20–30 minutes at a time at your desk.
- Quality mattress — medium-firm, not plush. See Morning Stiffness Management for specifics.
- Ergonomic workstation — standing desk, monitor at eye level, chair with proper lumbar support.
13. Working With a Physical Therapist
A good PT is worth more than any piece of equipment. They measure BASMI correctly, catch compensation patterns you cannot see, and calibrate load.
- Ask your rheumatologist for a referral — an AS-experienced PT is worth driving for. Generic orthopedic PTs sometimes prescribe flexion-biased programs that make AS worse.
- First 6–12 sessions establish baseline measurements, teach proper form, and individualize the home program.
- Insurance typically covers 30–60 visits per calendar year — check prior authorization rules before booking.
- Credentials to look for: APTA Certified Orthopaedic Specialist (OCS), Certified Manual Therapist, or Certified Functional Manual Therapist (CFMT).
- Hydrotherapy-equipped clinics — warm therapy pool on-site — are the gold standard for early-intensive AS rehab.
14. Workplace Strategies
Most AS progression happens during 40-hour weeks spent in a flexed posture. The workplace is where the disease wins or loses ground.
- Sit-stand desk — alternate positions every 30–60 minutes. Neither sitting nor standing all day is healthy; changing is.
- Walking meetings whenever the meeting does not require a screen.
- Hourly stretch breaks — set a timer; 30–60 seconds of standing backbends each hour adds up to 8+ minutes of extension per workday.
- Monitor and keyboard height — screen top at eye level, elbows at 90°, wrists neutral.
- Car posture — use a lumbar roll, avoid heavy seat recline, and stop every 90 minutes on long drives for extension work.
15. Realistic Timeline
Patients ask "when will I see results?" The honest answer is in two parts.
Subjective improvement — reduced stiffness, better sleep, more morning mobility — typically appears in 8–12 weeks of consistent practice. You will notice it before the tape measure does.
Objective BASMI improvement takes 6–12 months of consistent work and may plateau thereafter. Some spinal fusion is irreversible; the goal is preserving what you have and slowing what is progressing, not reversing bony bridges.
The best long-term outcomes appear in cohort data on patients who combine regular exercise with biologic therapy. See the Biologics Guide for how TNF inhibitors and IL-17 blockers interact with this program. Exercise alone is powerful. Exercise plus biologics is a different disease course.
16. AS Exercise Communities & Apps
Accountability and shared routines matter. A few reliable resources:
- NASS (National Ankylosing Spondylitis Society, UK) — free exercise videos, the most comprehensive library online.
- Spondylitis Association of America (SAA) — exercise guide, local support groups, aquatic program directories.
- Back Pain Liberation — YouTube channel with AS-specific routines.
- Curable app — pain-neuroscience education and guided practices for chronic pain regulation.
17. Key Research Papers
- van der Heijde D, et al. 2016 update of the ASAS-EULAR management recommendations for axial spondyloarthritis. Annals of the Rheumatic Diseases. 2017.
- Regnaux JP, et al. Home-based exercise programmes for ankylosing spondylitis (Cochrane review). Arthritis Care & Research. 2019.
- Dagfinrud H, et al. Physiotherapy interventions for ankylosing spondylitis. Cochrane Database of Systematic Reviews. 2008.
- Jennings F, et al. Exercise for people with axial spondyloarthritis. Rheumatology (Oxford). 2021.
18. Research Papers
Curated PubMed topic searches — each link opens a live query so you always see the most recent literature.
- PubMed: Ankylosing spondylitis exercise therapy
- PubMed: Ankylosing spondylitis hydrotherapy
- PubMed: BASMI / BASFI outcome measures
- PubMed: Ankylosing spondylitis and yoga
- PubMed: Spinal mobility in axial spondyloarthritis
- PubMed: Physiotherapy for spondylitis
- PubMed: Chest expansion in AS
- PubMed: McKenzie extension therapy
Connections
- Ankylosing Spondylitis
- HLA-B27 Explained
- Biologics Guide
- AS and IBD Overlap
- NSAID Strategy
- Morning Stiffness Management
- Starch-Free Diet and Ebringer
- Pregnancy and AS
- Uveitis and Eye Involvement
- Arthritis
- Tendinitis
- Chronic Pain
- Chronic Fatigue Syndrome
- Inflammatory Markers
- Exercise Pacing and Graded Movement