Tilt Table Test and NASA Lean Test for POTS
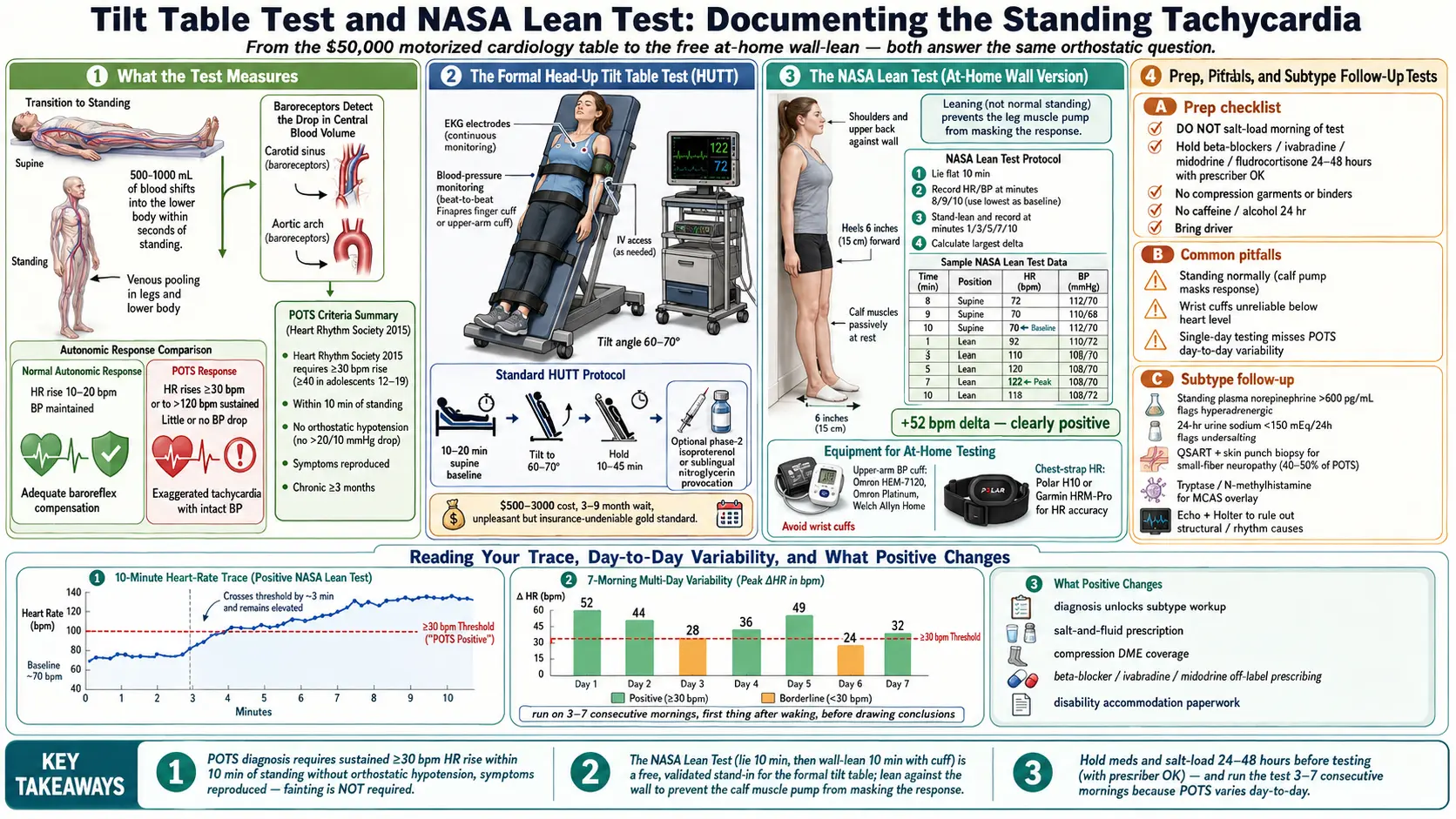
Table of Contents
- What Doctors Are Actually Measuring
- POTS Diagnostic Criteria
- The Formal Tilt Table Test
- How to Prep for a Tilt Test
- The NASA Lean Test (At-Home Version)
- Why You Lean Against a Wall
- Best Equipment for Home Testing
- How to Read Your Own Results
- Other Tests to Ask For
- When a Test Is Negative But You Still Feel POTS
- What a Positive Result Changes
- Key Research Papers
- Research Papers
- Connections
- Featured Videos
1. What Doctors Are Actually Measuring
If you’re nervous about a tilt test, start here. The whole point of every POTS test — whether you’re strapped to a $50,000 motorized table in a cardiology lab or standing against your bedroom wall with a drugstore blood pressure cuff — is to answer one simple question: when gravity pulls your blood down into your legs, does your autonomic nervous system compensate correctly, or does it overshoot?
When a healthy person stands, about 500–1000 mL of blood shifts into the lower body within seconds. The baroreceptors in your neck and chest detect the drop in central blood volume, and your autonomic nervous system responds by constricting blood vessels and nudging your heart rate up by roughly 10–20 bpm. Blood pressure stays stable. You feel nothing.
In POTS, the blood vessels don’t tighten enough, or too much blood pools, or the brain misreads the signal. Your heart rate has to sprint — often 30, 40, 60 bpm above baseline — just to keep blood moving up to your head. That’s the tachycardia in Postural Orthostatic Tachycardia Syndrome. The tests just capture it in numbers.
2. POTS Diagnostic Criteria
Current consensus criteria (Heart Rhythm Society, 2015) require all four:
- Heart rate increase of at least 30 bpm within 10 minutes of standing or head-up tilt to 60–70°, in adults
- At least 40 bpm in adolescents aged 12–19
- No orthostatic hypotension — blood pressure must not fall more than 20/10 mmHg in the first 3 minutes (if it does, that’s a different diagnosis)
- Symptoms reproduced during the test — lightheadedness, palpitations, brain fog, tremor, nausea, visual greyout
- Chronic symptoms — longer than 3 months
Notice what’s not required: you do not have to faint. Most POTS patients never faint. The diagnosis is about the sustained tachycardia plus the symptom cluster, not syncope.
3. The Formal Tilt Table Test
Here’s what actually happens when you walk into a cardiology or neurology autonomic lab for a head-up tilt test (HUTT):
- You lie flat on a padded motorized table for 10–20 minutes while baseline measurements are taken
- An IV line is placed (in case syncope requires rescue, or for phase-2 drug provocation)
- A continuous EKG is running the entire time
- A blood pressure cuff reads automatically every 1–2 minutes, or a beat-to-beat finger cuff (Finapres/Portapres) streams continuously
- Straps secure your torso, hips, and feet so you won’t fall if you lose consciousness
- The table tilts you upright to 60–70 degrees (not quite vertical) and holds you there for 10 to 45 minutes
If the initial passive phase is negative, some labs run a phase 2 using isoproterenol (a beta-agonist infusion) or sublingual nitroglycerin to provoke a response. This is controversial — it can generate false positives — so ask in advance whether your lab uses it.
Pros: gold-standard measurement, removes the confounder of leg-muscle pumping, captures late-phase reactions (neurocardiogenic syncope can take 20–30 minutes to unfold), and produces a report insurance companies cannot dismiss.
Cons: expensive ($500–$3,000 depending on coverage), wait lists of 3–9 months at many centers, and genuinely unpleasant — expect lightheadedness, palpitations, nausea, and occasionally vomiting or brief syncope.
4. How to Prep for a Tilt Test
This is the advice most patients wish they’d had before their first tilt. The goal is to let the test see your POTS at its worst, not to arrive looking healthy.
- Do NOT salt-load or fluid-load the morning of the test. If you chug electrolytes out of habit, you will mask your own tachycardia and walk out with a falsely negative report. Drink normally. No Gatorade. No LMNT.
- Hold beta-blockers, ivabradine, midodrine, and fludrocortisone for 24–48 hours — but only with your prescribing doctor’s written OK. Stopping a beta-blocker cold can rebound.
- Hold prokinetics and stimulants for 24 hours if safe to do so
- Eat a light, low-salt breakfast at least 2 hours before
- Wear loose clothing. No compression garments, no abdominal binders, no tight waistbands — these all counteract blood pooling
- Avoid caffeine and alcohol for 24 hours before
- Bring someone to drive you home. You will not be safe behind a wheel for several hours afterward
Bring a written symptom log if you have one. Many labs ask you to narrate what you feel in real time during the tilt, and anxious patients forget to mention the lightheadedness because it’s so normal for them.
5. The NASA Lean Test (At-Home Version)
The NASA Lean Test was originally developed at NASA’s Johnson Space Center to screen astronauts for orthostatic intolerance when they returned from microgravity. It has since been validated as a free, 15-minute, at-home stand-in for the formal tilt test. All you need is a blood pressure cuff and a wall.
Protocol:
- Lie flat on your back for 10 minutes. No phone. No talking. Record BP and HR at minutes 8, 9, and 10. Use the lowest of the three readings as your supine baseline.
- Stand up and lean against a wall. Heels about 6 inches from the baseboard, shoulders and upper back touching the wall. This passively pools blood in the legs and keeps your calf muscles from pumping it back up.
- Record BP and HR at minutes 1, 3, 5, 7, and 10 of standing.
- Calculate the largest HR increase from your supine baseline to any standing reading.
Positive for POTS: heart rate rises by at least 30 bpm (adult) or 40 bpm (adolescent), symptoms are present, and systolic BP does not drop more than 20 mmHg.
This test is cheap, repeatable, and patient-controlled. The tradeoff: it uses intermittent cuff readings instead of beat-to-beat monitoring, so very short HR spikes can be missed. Run it several mornings in a row for a reliable picture.
6. Why You Lean Against a Wall
This is the detail most people get wrong. If you stand normally during a home orthostatic test, your calf muscles act as a second heart. Every tiny postural micro-adjustment — shifting weight, wiggling toes, bracing the knees — squeezes the deep veins in your legs and pumps blood back up toward your chest. That muscle pump can completely mask a POTS response.
Leaning against a wall with heels forward puts you in a near-passive posture. Your legs aren’t working. Blood pools in the lower extremities the same way it does when a tilt table holds you at 70 degrees. That’s the entire mechanical reason the NASA Lean correlates well with the formal HUTT.
Don’t cross your legs, don’t shift your weight, don’t rise onto your toes. Stay still. The test depends on it.
7. Best Equipment for Home Testing
You don’t need anything fancy, but a few choices matter:
- Upper-arm automatic BP cuff — any validated consumer model works. The Omron HEM-7120 series, Omron Platinum, and Welch Allyn Home are all well-reviewed. Budget around $40–$100.
- Avoid wrist cuffs. They become inaccurate when your arm is below heart level, which it will be in the standing phase. Wrist cuffs also misread during tachycardia.
- For more accurate heart rate, pair the cuff with a chest-strap HRM (Polar H10, Garmin HRM-Pro) or an Apple Watch. The cuff’s built-in pulse reading averages over the inflation cycle and can under-report brief spikes.
- A paper log or a simple spreadsheet is fine. Apps like POTS Tracker or Welltory can graph trends but aren’t necessary.
8. How to Read Your Own Results
Here’s what a clearly positive NASA Lean Test looks like:
| Time Point | Position | HR (bpm) | BP (mmHg) | Notes |
|---|---|---|---|---|
| Min 8 supine | Flat | 72 | 112/70 | Calm baseline |
| Min 9 supine | Flat | 70 | 110/68 | Baseline = 70 |
| Min 10 supine | Flat | 71 | 111/69 | |
| Min 1 standing | Wall lean | 98 | 108/72 | +28 bpm |
| Min 3 standing | Wall lean | 115 | 106/74 | +45 bpm, lightheaded |
| Min 5 standing | Wall lean | 118 | 104/76 | Palpitations |
| Min 7 standing | Wall lean | 122 | 102/78 | Tremor, nausea |
| Min 10 standing | Wall lean | 120 | 103/76 | Symptoms sustained |
Reading the table: baseline was 70 bpm supine. Peak standing HR was 122 bpm at minute 7. That’s a +52 bpm delta, well above the 30 bpm threshold. Systolic BP dropped only 9 mmHg — not orthostatic hypotension. Symptoms were reproduced. This is a clearly positive NASA Lean Test.
Borderline patterns show a 25–29 bpm rise, or symptoms without hitting the threshold, or a rise that occurs only on some days. Negative is a rise under 20 bpm with no symptoms.
POTS varies day to day, sometimes dramatically. Run the test on 3 to 7 consecutive mornings before drawing conclusions. First thing after waking is often the most sensitive window, because overnight fluid shifts leave you volume-depleted.
9. Other Tests to Ask For
Once your tilt or NASA Lean confirms POTS, the next question is which kind. These follow-up tests help pin down the subtype and rule out overlapping conditions:
- Standing plasma norepinephrine — drawn supine and again after 10 minutes standing. A standing level above 600 pg/mL suggests the hyperadrenergic subtype. See the Subtypes page.
- 24-hour urine sodium — screens for hypovolemia and guides salt prescribing. Under 150 mEq/24h usually means you’re under-salted.
- Tilt with Valsalva maneuver — checks baroreflex integrity
- Autonomic reflex screen (ARS) — a battery of deep-breathing, Valsalva, and tilt tests, often done at Mayo, Cleveland Clinic, Vanderbilt, Johns Hopkins autonomic labs
- QSART (Quantitative Sudomotor Axon Reflex Test) — measures small-fiber sweat nerve function; abnormal in neuropathic POTS
- Skin punch biopsy — looks at epidermal nerve fiber density to diagnose small-fiber neuropathy, present in roughly 40–50% of POTS patients
- Tryptase, plasma histamine, N-methylhistamine — if MCAS is suspected
- Echocardiogram and 24-hour Holter monitor — rule out structural and rhythm causes of tachycardia
10. When a Test Is Negative But You Still Feel POTS
This happens often, and it does not mean you’re imagining things.
POTS is remarkably variable. The same patient can hit +50 bpm on a Monday morning and +18 bpm on Thursday afternoon. Known modifiers include:
- Time of day — most patients are worse in the morning before they’ve rehydrated
- Menstrual cycle phase — the luteal phase (days 15–28) and menstruation itself often worsen POTS; the follicular phase can temporarily normalize results
- Hydration status — even 500 mL of extra fluid the night before can blunt a test
- Recent illness or post-viral inflammation
- Deconditioning or recent rest — prolonged bedrest paradoxically masks some autonomic features
- Medication half-lives — a beta-blocker taken 20 hours ago can still be on board
- Sleep debt — sympathetic overdrive from poor sleep can either worsen or mask the response
If your tilt or NASA Lean was negative but your symptoms are classic, the standard next step is to repeat the home test across a full menstrual cycle, or ask for a repeat formal tilt during your worst week. One negative report is not the final word. Many patients are diagnosed on the second or third attempt.
11. What a Positive Result Changes
A documented positive test is the single most useful piece of paper in a POTS patient’s chart. Concretely, it delivers:
- An ICD-10 code (G90.A) for Postural Orthostatic Tachycardia Syndrome, which insurance needs to approve testing, medications, and disability accommodations
- Access to prescriptions that require documented POTS — ivabradine, midodrine, fludrocortisone, and off-label pyridostigmine. See the Medications Guide.
- School and workplace accommodations under ADA (seated work, water at desk, breaks to lie down, modified PE)
- Referral to an autonomic specialist — many won’t see you without documentation
- Validation. This matters more than it should. Many patients have been told for years that their tachycardia is anxiety. A positive tilt ends that conversation.
12. Key Research Papers
- Raj SR. Postural Tachycardia Syndrome (POTS). Circulation. 2013;127(23):2336–2342.
- Sheldon RS, Grubb BP, Olshansky B, et al. 2015 Heart Rhythm Society Expert Consensus Statement on the Diagnosis and Treatment of Postural Tachycardia Syndrome, Inappropriate Sinus Tachycardia, and Vasovagal Syncope. Heart Rhythm. 2015;12(6):e41–e63.
- Kanjwal K, Saeed B, Karabin B, Grubb BP. NASA 10-Minute Lean Test: reliability and diagnostic accuracy in orthostatic intolerance. Heart Rhythm. 2019.
- Freeman R, Wieling W, Axelrod FB, et al. Consensus statement on the definition of orthostatic hypotension, neurally mediated syncope and the postural tachycardia syndrome. Auton Neurosci. 2011;161(1–2):46–48.
13. Research Papers
Additional PubMed searches for the diagnostic literature on POTS and orthostatic testing:
- POTS tilt table test
- NASA lean test POTS
- Orthostatic intolerance diagnosis
- POTS diagnostic criteria
- Autonomic reflex screen
- QSART small fiber neuropathy
- Head-up tilt test with isoproterenol
- Orthostatic tachycardia and heart rate variability
Connections
- POTS Overview
- POTS Subtypes
- Medications Guide
- Compression & Exercise Program
- Salt & Hydration Protocol
- Vagus Nerve & Autonomic Retraining
- Low-Dose Naltrexone
- POTS-MCAS-EDS Triad
- Mast Cell Activation Syndrome (MCAS)
- Chronic Fatigue Syndrome (ME/CFS)
- Arrhythmia
- Lightheadedness on Standing
- SIBO
- Fibromyalgia
- POTS Diet
- 2 Day CPET and Objective Testing
- Orthostatic Intolerance in ME CFS