Salt and Hydration Protocol for POTS
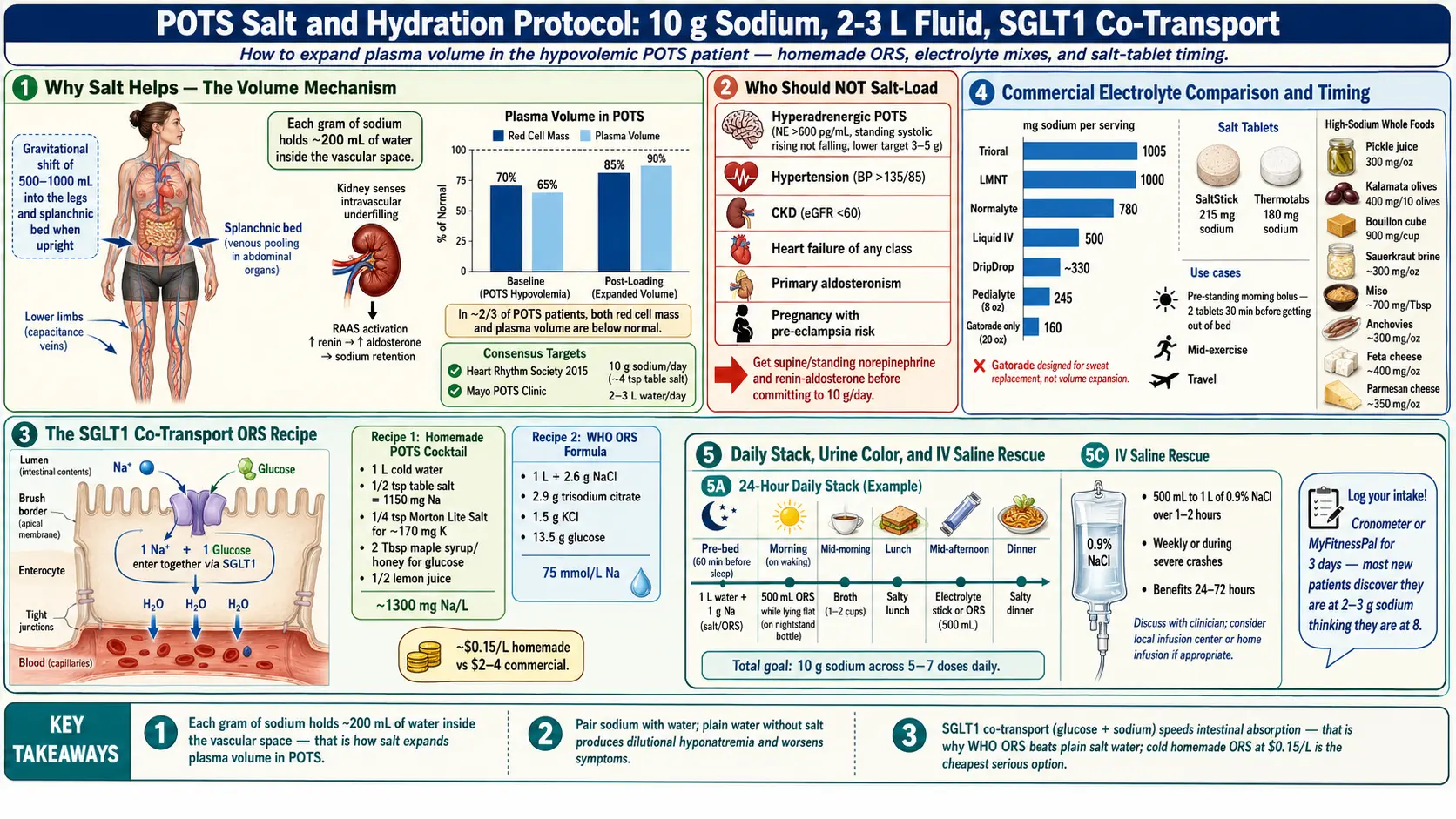
Table of Contents
- Why Salt Helps POTS
- Who Should NOT Salt-Load
- The Fluid Target
- How to Actually Hit 10g Sodium
- Homemade ORS Recipes
- Commercial Electrolyte Products Compared
- Salt Tablets vs Food-Based Salt
- Timing Strategies
- IV Saline for Crisis and Flares
- Monitoring What’s Working
- Side Effects and Trade-offs
- Key Research Papers
- Research Papers
- Connections
- Featured Videos
1. Why Salt Helps POTS
Most people with POTS are running on low blood volume. Studies consistently show mild to moderate hypovolemia — red cell mass and plasma volume both measured below normal in roughly two-thirds of patients. When you stand up, gravity pulls 500–1000 mL of blood into the lower body. If your total circulating volume is already short, there isn’t enough venous return to fill the heart, cardiac output drops, and the sympathetic nervous system fires a tachycardic rescue. That’s the core mechanism of orthostatic intolerance.
Sodium is how you fix volume. Every gram of sodium holds roughly 200 mL of water inside the vascular space. Take in more sodium with adequate fluid and your plasma volume expands — which is exactly the goal.
The target endorsed by the Heart Rhythm Society 2015 consensus and the Mayo Clinic POTS clinic is 10 grams of sodium per day. That is roughly 25 grams of table salt, or about 4 teaspoons. The “2300 mg/day healthy adult” ceiling is written for the general population at risk of hypertension — it does not apply to a hypovolemic POTS patient whose supine blood pressure is 95/60.
2. Who Should NOT Salt-Load
Aggressive salt loading is not universal. Before you start, check whether any of these apply:
- Hyperadrenergic POTS. This subtype is driven by excess norepinephrine, not hypovolemia. Standing plasma norepinephrine >600 pg/mL, standing systolic BP often rising rather than falling. High sodium can worsen symptoms in this group. A lower target of 3–5 g sodium/day is more appropriate. See POTS Subtypes to identify which group you’re in.
- Hypertension. Resting BP consistently >135/85. Salt loading will worsen it.
- Chronic kidney disease (eGFR <60).
- Heart failure of any class.
- Primary aldosteronism or other mineralocorticoid excess.
- Pregnancy with pre-eclampsia risk.
If you’re not sure which subtype you have, get a supine and standing norepinephrine level before committing to 10 g/day. It’s a single blood draw and it settles the question.
3. The Fluid Target
The companion target is 2–3 liters of water per day. Sodium and fluid must be paired. Each alone fails:
- Sodium without fluid pulls water from your cells into the bloodstream transiently, then gets excreted — net result: intracellular dehydration, headache, thirst.
- Fluid without sodium is worse. Plain water without accompanying salt is excreted by the kidneys within 30–60 minutes and can actually lower your plasma sodium (dilutional hyponatremia), producing the exact symptoms you’re trying to treat.
The simplest feedback loop is urine color. Pale straw = good hydration. Completely clear = too much free water, not enough salt. Dark amber = you’re behind on fluid. Aim to pee 4–6 times a day, straw-colored.
4. How to Actually Hit 10g Sodium
Ten grams sounds huge. It is huge. But you build it out of five stacking sources rather than trying to cram it into meals.
Salt your food aggressively
1 teaspoon of table salt = ~2.3 g sodium = ~6 g salt. Adding 2–3 teaspoons across the day (soups, eggs, rice, meat, popcorn) gets you 4–7 g of sodium without any supplements. Keep a small salt grinder with you. Salt every glass of water. Yes, really.
Broth-first strategy
Two cups of well-salted broth per day (chicken, beef, bone, vegetable) delivers 1600–2400 mg sodium. Warm broth between meals is also the easiest bolus on an irritable stomach. Bouillon cubes work: a Knorr cube is roughly 900 mg sodium in one cup.
Electrolyte mixes
One to three packets/day (see the commercial comparison below) covers another 1–3 g sodium plus potassium and often glucose for faster absorption.
High-sodium whole foods
Pickle juice (1 oz = ~300 mg sodium), olives (10 kalamata = ~400 mg), sauerkraut brine, miso, soy sauce, anchovies, feta, parmesan. Useful when you’re fatigued on sweet electrolyte drinks.
Salt tablets
SaltStick caps (215 mg sodium each) and Thermotabs (180 mg each) are the standard picks. Useful for targeted dosing around exercise or before standing.
Log for 3 days
Use Cronometer or MyFitnessPal for 3 days to get your baseline. Nearly every new patient discovers they’re at 2–3 g sodium/day thinking they’re at 8. Close that gap deliberately.
5. Homemade ORS Recipes
Oral rehydration solutions beat plain salt water because they use sodium-glucose co-transport (SGLT1): a small amount of glucose dramatically speeds sodium absorption across the gut wall. The WHO designed this formula to treat cholera. It works equally well for POTS.
The “POTS Cocktail” (easy version)
- 1 liter cold water
- 1/2 teaspoon table salt (~1150 mg sodium)
- 1/4 teaspoon Morton Lite Salt (adds ~170 mg potassium plus more sodium)
- 2 tablespoons maple syrup or honey (glucose for co-transport)
- Juice of 1/2 lemon
Shake in a Nalgene bottle. Total sodium: ~1300 mg per liter. Drink cold; palatability jumps.
WHO ORS (exact formula)
- 1 liter water
- 2.6 g sodium chloride (table salt)
- 2.9 g trisodium citrate dihydrate
- 1.5 g potassium chloride
- 13.5 g anhydrous glucose
This is the reference formula. Total sodium ~75 mmol/L (1725 mg/L). Trisodium citrate is sold as a canning ingredient; KCl as “NoSalt” or “Nu-Salt” at most grocery stores.
Cost per liter: ~$0.15 homemade vs. $2–$4 for commercial equivalents. Store in the fridge. Cold temperature masks the salinity and many patients find they’ll actually drink it cold when warm was unbearable.
6. Commercial Electrolyte Products Compared
Per packet/serving as marketed. Sodium is the number that matters for POTS.
LMNT
1000 mg sodium + 200 mg potassium + 60 mg magnesium. Sugar-free (uses stevia). ~$1.50/packet. Strong sodium per serving, no glucose means slower absorption but avoids sugar swings — a plus for patients with MCAS or reactive hypoglycemia, a minus for pure absorption speed.
Liquid IV
500 mg sodium + 370 mg potassium + 11 g sugar (glucose for co-transport). ~$1.30/stick. Widely available at Costco, Target, Amazon. The co-transport formulation is legitimate; sodium dose is modest so you often need two packets.
Normalyte
780 mg sodium + 300 mg potassium + 20 g glucose. WHO ORS formulation. ~$0.70/packet. Popular in the dysautonomia community because it’s medical-grade rehydration at a reasonable price.
Trioral
1005 mg sodium + 580 mg potassium + 13.5 g glucose. The exact WHO ORS formula in a sachet. ~$0.35/packet in bulk from Amazon. Cheapest serious option. Tastes medicinal — that’s the price of the correct formula.
Pedialyte
245 mg sodium per 8 oz serving (~490 mg per 16 oz bottle). Drugstore ubiquitous. High sugar in the flavored versions. Fine for acute flares when you need something now.
Hydralyte / DripDrop / Buoy
Mid-range: 300–500 mg sodium per serving, glucose-based, $1–$2 each. DripDrop is the most medical-feeling of the three; Buoy is liquid drops you add to existing drinks (convenient, low sodium per use).
Skip: Gatorade and Powerade
Gatorade has only 160 mg sodium per 20 oz bottle and 36 g of sugar. Powerade is similar. Designed for athletes replacing sweat loss — not for volume-expanding a hypovolemic POTS patient. You’d need 6 bottles to hit a single gram of sodium.
7. Salt Tablets vs Food-Based Salt
Food-based salt should be your base. Tablets are a tool for specific situations:
- When food load is already high and adding another salty meal makes you nauseous. A tablet with water skips the food.
- During exercise — sweat plus orthostatic stress can crater you. Two SaltStick caps at 30 minutes into a workout, with water.
- Pre-standing morning bolus — 2 tablets (~430 mg) 30 minutes before getting out of bed, with a full glass of water. This is the single most underused hack in the POTS playbook.
- Travel — airports and rental cars don’t provide broth. Tablets in a pill box solve it.
Downsides: tablets give you sodium without paired fluid by default, so you must wash them down with a full glass of water or you’ll create transient hyperosmolality and a headache. Don’t dry-swallow.
8. Timing Strategies
Pre-bed salt loading
Drink 1 liter of water + 1 g sodium 30–60 minutes before sleep. Blood volume naturally contracts overnight through insensible losses and antidiuretic hormone cycling — pre-loading preserves morning volume and softens the brutal first-standing spike.
Morning bolus before standing
Keep a pre-made bottle of ORS on the nightstand. Drink 500 mL while still lying flat, wait 10–15 minutes, then sit up slowly. This alone will drop many patients’ morning heart rate spike by 20–30 bpm.
Between-meal mini-doses
Never try to slam 10 g of sodium into one or two meals — it causes bloating, reflux, and fatigue. Break it into 5–7 smaller hits across the day: morning bolus, mid-morning broth, salty lunch, electrolyte stick mid-afternoon, salty dinner, pre-bed bottle. You’ll feel it working by week two.
9. IV Saline for Crisis and Flares
For patients whose oral intake can’t keep up — severe flares, viral illness, MCAS reactions, post-exertional crashes — intravenous normal saline (0.9% NaCl) works where oral fails. A typical protocol is 500 mL to 1 L over 1–2 hours, weekly or during acute crashes. Benefits are usually felt within the infusion and last 24–72 hours.
Access options, ranked from least to most invasive:
- Peripheral IV in an infusion center — most common, stick-per-session, lowest infection risk.
- CVICU or mobile RN home infusion — better for patients who can’t travel on bad days.
- Port-a-cath — considered when weekly access is long-term certain and peripheral veins have failed.
- PICC line — last resort. High infection, clot, and hospitalization risk in chronic POTS use. Consider only when every other option has been exhausted and benefit is clearly documented.
Evidence base is small case series (Ruzieh 2017, Moak 2016) rather than randomized trials, but reported response rates in refractory POTS run 70–85% for substantial symptom reduction. Not first-line, but genuinely life-changing for the severe end of the disease.
10. Monitoring What’s Working
Treat salt loading like a drug trial on yourself. Track objective numbers, not just how you feel:
- Morning and evening blood pressure + heart rate (home cuff). Supine for 5 minutes, then 1, 3, and 10 minutes standing. The standing HR delta is your core metric.
- Weekly NASA Lean Test for the first month — see Tilt Table & NASA Lean Test.
- Standing-symptom diary — 1–10 scale for lightheadedness, palpitations, fatigue, brain fog, each morning.
- Body weight daily. Effective salt loading adds 1–3 lbs of retained fluid in the first 1–2 weeks. That weight gain is the treatment working, not a complication.
- 24-hour urine sodium at 4 weeks — the definitive measurement of whether you’re actually hitting 10 g/day of intake.
If after 4 weeks of documented 10 g/day intake with 2–3 L fluid you have zero symptom improvement, you likely have hyperadrenergic or neuropathic POTS where volume expansion isn’t the limiting factor — time to move on to pharmacotherapy.
11. Side Effects and Trade-offs
- Swollen ankles and hands. Common in weeks 1–3. Usually resolves as vasculature adapts. Compression socks help; see Compression & Exercise Program.
- Headaches. Almost always from fluid without enough sodium, not the reverse. Add salt, not water.
- Acid reflux. High salt can irritate. Split doses across the day, take with food, avoid lying down within an hour of a salt bolus.
- Potassium imbalance. Heavy sodium loading without potassium replacement can trigger cramps or palpitations. Add half a banana, a cup of coconut water, or 1/4 tsp Morton Lite Salt daily. Aim for 3–4 g potassium/day.
- Bloating. Usually a timing/pacing issue — smaller, more frequent doses fix it.
- Taste fatigue. Rotate sources: broth one day, ORS another, pickles and olives on a third. The patient who eats the same salted chicken for six weeks quits.
12. Key Research Papers
- Raj SR, et al. Postural tachycardia syndrome (POTS): review and evidence-based approach. Circulation. 2013.
- Raj SR, et al. Postural Tachycardia Syndrome. New England Journal of Medicine. 2020.
- Sheldon RS, et al. 2015 Heart Rhythm Society expert consensus statement on the diagnosis and treatment of POTS. Heart Rhythm. 2015.
- Miller AJ, Raj SR. Pharmacotherapy for postural tachycardia syndrome (including volume expansion). Autonomic Neuroscience. 2018.
13. Research Papers
Curated PubMed topic searches — each link opens a live query so you always see the most recent literature.
- PubMed: POTS salt, sodium, volume expansion
- PubMed: Oral rehydration in POTS
- PubMed: IV saline for POTS
- PubMed: Fludrocortisone for POTS
- PubMed: Hypovolemia in postural tachycardia
- PubMed: Salt loading for orthostatic intolerance
- PubMed: Hyperadrenergic POTS norepinephrine
- PubMed: Sodium-glucose co-transport rehydration
Connections
- POTS Overview
- POTS Subtypes
- Tilt Table Test
- Compression and Exercise Program
- Medications Guide
- POTS/MCAS/EDS Triad
- Vagus Nerve and Autonomic Retraining
- LDN for POTS
- Potassium
- Magnesium
- MCAS
- SIBO
- Lightheadedness on Standing
- Fatigue
- Orthostatic Intolerance in ME CFS
- POTS Diet