Vagus Nerve and Autonomic Retraining for POTS
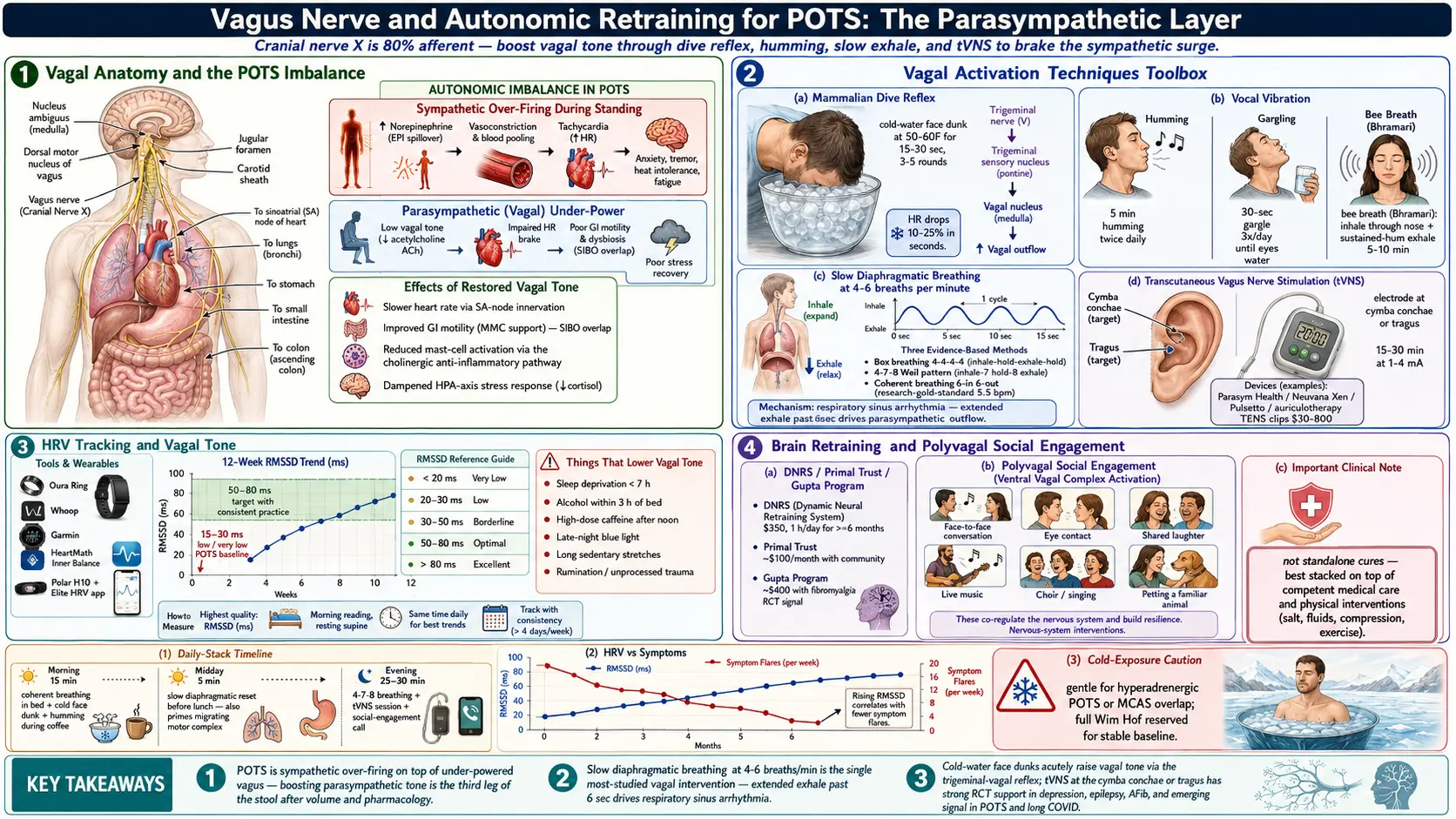
Table of Contents
- Why the Vagus Nerve Matters for POTS
- How to Measure Vagal Tone
- The Dive Reflex (Cold-Water Face Dunk)
- Humming, Chanting, Gargling
- Slow Diaphragmatic Breathing
- Transcutaneous Vagus Nerve Stimulation (tVNS)
- Cold Exposure Beyond Face Dunks
- Brain Retraining Programs
- Polyvagal Theory and Social Engagement
- Things That Lower Vagal Tone
- Integration Strategy — A Daily Vagal Practice
- Measuring Results
- What This Is Not
- Key Research Papers
- Research Papers
- Featured Videos
1. Why the Vagus Nerve Matters for POTS
The vagus nerve is cranial nerve X — the longest nerve in the body and the main highway of the parasympathetic “rest and digest” nervous system. It wanders from the brainstem down through the neck, heart, lungs, and gut, carrying roughly 80% afferent (body-to-brain) and 20% efferent (brain-to-body) fibers.
In POTS, the autonomic balance is broken in a specific way: the sympathetic (fight-or-flight) branch is over-firing, while the parasympathetic branch — chiefly the vagus — is under-powered. Standing up, which should produce a modest sympathetic surge that is quickly braked by vagal tone, instead produces a runaway tachycardia that nothing slows down.
Boosting vagal tone does several things that matter for POTS at once: it slows heart rate through direct sinoatrial-node innervation, improves gastrointestinal motility (relevant to the large POTS-SIBO overlap), reduces mast-cell activation via the cholinergic anti-inflammatory pathway, and dampens the HPA-axis stress response. This isn't mystical. It's anatomy.
The practical implication: the vagal layer is a real, measurable, trainable system. Most POTS treatment focuses on volume (salt, fluids, compression) and pharmacology (beta-blockers, ivabradine, midodrine, fludrocortisone). The vagal layer is the third leg of the stool, and for many patients it's the one that finally stabilizes their baseline.
2. How to Measure Vagal Tone
Heart rate variability (HRV) is the most practical proxy for vagal tone available to consumers. HRV is the beat-to-beat variation in heart rate — higher variability means the vagus is actively modulating the sinus node, which is what you want. A metronomically steady heartbeat is a sick heartbeat.
Consumer tools that track HRV reliably:
- Oura Ring — overnight RMSSD; excellent trend data
- Whoop — continuous, subscription-based
- Garmin watches — HRV status feature on newer models
- HeartMath Inner Balance — earlobe or finger sensor; pairs biofeedback with training
- Polar H10 chest strap + Elite HRV app — research-grade accuracy, lowest cost
Most POTS patients start with a morning RMSSD in the 15-30 ms range (considered low to very low). With consistent practice across the techniques below, moving into the 50-80 ms range over several months is a realistic target, and it typically tracks with symptom improvement.
3. The Dive Reflex (Cold-Water Face Dunk)
The mammalian dive reflex is the fastest way to acutely raise vagal tone. Mechanism: cold water on the forehead, cheeks, and around the eyes stimulates the trigeminal nerve, which synapses onto the vagal nucleus in the brainstem and triggers a rapid bradycardia — the heart rate can drop 10-25% in seconds.
Protocol: Fill a bowl with cold tap water plus a handful of ice cubes (target 50-60°F). Take a breath. Immerse the face from forehead to chin for 15-30 seconds. Come up, breathe, repeat 3-5 times.
Use it acutely during a POTS flare, a tachycardia episode, or a rising panic response — it works within one cycle. Used daily as a morning ritual, it also raises tonic vagal baseline over a 4-8 week horizon. If face immersion isn't practical, a cold gel pack held over the forehead and cheeks for 30-60 seconds produces a smaller but measurable version of the same reflex.
4. Humming, Chanting, Gargling
The vagus branches through the throat, innervating the muscles of the soft palate, pharynx, and larynx. Vibrating those tissues mechanically stimulates vagal afferents — this is why singers, chanters, and meditators across every tradition end up discovering vocal vibration as a nervous-system tool.
Humming
5 minutes of sustained “mmmmm” at whatever pitch sits comfortably in your chest, twice daily. The felt sense is a buzz in the sinuses and upper throat.
Gargling
30 seconds with plain water, 3 times a day, hard enough that your eyes water. Watering eyes are a reliable signal of vagal activation — that's the nerve firing.
Chanting “Om” or Singing
Long slow exhalations amplify the vagal effect because the parasympathetic system is already activated by extended exhale. Chanting combines the vibration and the slow-exhale mechanisms simultaneously.
Bee Breath (Bhramari Pranayama)
Classical yogic humming breath: inhale through the nose, exhale with a sustained hum, fingers optionally closing the ears to amplify the internal vibration. 5-10 minutes in the morning — one of the most consistently effective vagal practices in published breathing studies.
5. Slow Diaphragmatic Breathing
If you only have time for one vagal technique, this is it. Slow diaphragmatic breathing is the single most-studied vagal intervention, and the effect size is large enough that it shows up on HRV monitors within minutes.
The mechanism is called respiratory sinus arrhythmia: heart rate naturally rises on inhale (sympathetic) and falls on exhale (parasympathetic). Extending the exhale past roughly 6 seconds drives parasympathetic outflow through the nucleus ambiguus.
Technique: 4-6 breaths per minute, for 5-10 minutes, 2-3 times daily. One hand on the belly to make sure the diaphragm — not the chest — is doing the work.
Specific patterns that all work:
- Box breathing — 4 in, 4 hold, 4 out, 4 hold
- 4-7-8 breathing — inhale 4, hold 7, exhale 8 (Andrew Weil's pattern)
- Coherent breathing — 6 seconds in, 6 seconds out (the research-gold-standard 5.5 bpm)
Useful apps: Breathwrk, iBreathe (free), Headspace, HeartMath. A metronome app set to 10 beats per minute works just as well.
6. Transcutaneous Vagus Nerve Stimulation (tVNS)
The auricular branch of the vagus surfaces at the cymba conchae and tragus of the outer ear — one of the only places the vagus is accessible through skin. tVNS devices deliver small electrical pulses at that location, producing cortical and brainstem vagal activation without surgery.
Devices
- Parasym Health — FDA-cleared for stroke rehabilitation and TBI; clinical-grade
- Neuvana Xen — earbuds with pulsed current synced to music
- Pulsetto — neck-worn; targets the cervical vagus
- NuCalm — hybrid electrical + biosignal protocol
- Auriculotherapy TENS clips — inexpensive generic ear-clip electrodes hooked to a standard TENS unit
Protocol
15-30 minutes per day. Start at 1-2 mA and titrate up until you feel a clear tingle or mild pulsation with no pain or burning. Most users find a setting in the 2-4 mA range.
Evidence
Strong randomized-trial support exists in depression, epilepsy, and atrial fibrillation. Emerging evidence in POTS and long COVID is promising — Stavrakis and colleagues at Oklahoma have published several positive signals in autonomic dysfunction. The risk profile is excellent.
Cost
$300-800 for medical-grade devices; $30-60 for auriculotherapy clips plus a basic TENS unit. The cheap setup is perfectly adequate to test whether you respond before investing in a polished device.
7. Cold Exposure Beyond Face Dunks
Beyond the acute dive reflex, broader cold exposure builds tonic vagal capacity:
- Cold showers — 30-60 seconds of cold at the end of your normal warm shower
- Ice packs on chest or back of neck — 2-5 minutes while seated
- Wim Hof-style breathing plus cold plunge — advanced; powerful HRV lift
Start gentle. Cold stress can trigger mast-cell flares in patients with concurrent MCAS, and can transiently spike catecholamines in hyperadrenergic POTS subtype. If either applies and your baseline is currently unstable, skip cold exposure beyond the face dunk until the storm settles.
8. Brain Retraining Programs
Systematic limbic-retraining programs have a decidedly mixed reputation, partly because they get marketed with cure-all language they don't deserve. The underlying neuroscience — that a chronically sensitized limbic system can be retrained through structured, repeated exposure and state-shift practice — is real. Neuroplasticity is not imaginary, and the overlap between chronic-illness populations and altered limbic reactivity is well-documented.
These programs are not standalone cures. They work best stacked on top of competent medical care and the physical interventions (salt, fluids, compression, exercise reconditioning).
DNRS (Dynamic Neural Retraining System)
Annie Hopper's program. DVD set or streaming course, around $350. Protocol: 1 hour per day for a minimum of 6 months. Has the largest anecdotal track record in the POTS, MCAS, and multiple-chemical-sensitivity communities.
Primal Trust Academy
Cathleen King's program. Monthly subscription around $100. More affordable, with an active community, live calls, and polyvagal and somatic work layered on top of the retraining core.
Gupta Program
Ashok Gupta's approach, originally developed for ME/CFS and fibromyalgia. Streaming course around $400. Well-structured, with a published RCT signal in fibromyalgia.
Curable, Lightning Process
Adjacent limbic-retraining approaches. Curable is app-based and pain-focused; the Lightning Process is a short-format in-person seminar with its own controversies but also a real evidence base in chronic fatigue.
All of these require daily commitment. Expect 2-6 months before you notice a clear shift, and stop believing any testimonial that promises faster.
9. Polyvagal Theory and Social Engagement
Stephen Porges's polyvagal theory reframes the vagus into three evolutionary layers, of which the most recent — the ventral vagal complex — is the one engaged by safe social connection.
The practical takeaway is small and profound: face-to-face conversation, eye contact, shared laughter, live music, and singing with other people directly stimulate ventral vagal tone. Chronic illness is isolating, and isolation degrades vagal tone in a measurable feedback loop. Deliberate social contact — even 20 minutes of real conversation with one person — is a nervous-system intervention, not a luxury.
Things that count: a weekly meal with a friend, a choir or singing group, a video call with eye contact (not Slack), petting a familiar animal, playing with a child. Things that don't: doomscrolling, parasocial YouTube time, text threads.
10. Things That Lower Vagal Tone
Everything above works faster when the vagal drains are plugged:
- Chronic sleep deprivation (below 7 hours)
- Alcohol — especially within 3 hours of bed; crushes overnight HRV
- High-dose caffeine, particularly after noon
- Screen time in bed and late-night blue light
- Stimulant medications used poorly or at too high a dose
- Long sedentary stretches (the vagus tracks with movement)
- Rumination, catastrophizing, unprocessed trauma
Addressing these is slower, less glamorous, and cumulative — and often the reason a perfectly good daily practice doesn't move the HRV needle.
11. Integration Strategy — A Daily Vagal Practice
A realistic, stackable daily protocol:
Morning (15 minutes):
- 5 minutes of coherent breathing (6 in / 6 out) before getting out of bed
- Cold-water face dunk — 3 rounds of 20 seconds
- 5 minutes of humming or bee breath while making coffee or tea
Midday (5 minutes):
- Slow diaphragmatic breathing reset before lunch — this also primes the migrating motor complex and supports digestion
Evening (25-30 minutes):
- tVNS for 20 minutes while watching TV or reading
- Gargling with water before brushing teeth, 30 seconds
- Screens off 1 hour before bed
Weekly:
- 1-2 cold showers (30-60 seconds at the end)
- Intentional in-person social time — one meaningful conversation minimum
- One session of a structured brain-retraining practice if you're running a program
12. Measuring Results
Track the following as a weekly average, not a single data point:
- Morning HRV (RMSSD) — primary metric
- Standing heart rate at 1, 3, and 10 minutes — the core POTS signal
- Symptom diary — presyncope episodes, brain fog days, crash days
- NASA Lean Test monthly as an objective standing-tolerance benchmark
Expect 4-8 weeks before HRV begins to shift and 3-6 months before symptom patterns meaningfully change. Daily consistency beats weekly intensity every time.
13. What This Is Not
This is not a replacement for medications, compression garments, or salt-and-fluid protocols. It is not a cure for severe POTS. It is not a substitute for addressing MCAS or EDS comorbidity. And it is emphatically not a suggestion that POTS is psychological or that you could meditate your way out of it — the dysautonomia is physiological, the mechanism for vagal intervention is physiological, and the evidence is physiological.
What it is: a near-zero-cost, near-zero-side-effect adjunct with genuine mechanistic backing and a growing clinical evidence base. For patients who can't tolerate medications because of MCAS crossreactivity or who face financial barriers to specialist care, it's often the most effective lever available. For patients already on good pharmacology, it's the layer that often pushes stability from “functional” to “actually living.”
14. Key Research Papers
- Porges SW. Polyvagal theory: A biobehavioral journey to sociality. Int J Cardiol. 2017.
- Breit S, Kupferberg A, Rogler G, Hasler G. Vagus nerve as modulator of the brain-gut axis in psychiatric and inflammatory disorders. Front Psychiatry. 2018.
- Stavrakis S, et al. Transcutaneous vagus nerve stimulation in autonomic disorders. Auton Neurosci. 2019.
- Koopman FA, et al. Vagus nerve stimulation inhibits cytokine production and attenuates disease severity — cholinergic anti-inflammatory pathway. Int J Neuropsychopharmacol. 2018.
15. Research Papers
Curated PubMed topic searches — live queries that surface the newest peer-reviewed work on each topic.
- PubMed: Vagus nerve and POTS
- PubMed: Heart rate variability in POTS
- PubMed: Transcutaneous vagus nerve stimulation
- PubMed: Polyvagal theory
- PubMed: Diaphragmatic breathing and autonomic function
- PubMed: Cold exposure and vagal tone
- PubMed: Dynamic neural retraining and chronic illness
Connections
- POTS Overview
- POTS Subtypes
- Medications Guide
- Compression and Exercise
- Salt and Hydration
- Tilt Table Test
- LDN for POTS
- POTS/MCAS/EDS Triad
- MCAS
- SIBO
- ME/CFS
- Fibromyalgia
- Anxiety
- Gut-Brain Axis
- Arrhythmia
- Triggers and Flare Management
- POTS Diet