POTS Diet: Small Frequent Meals & Postprandial Crashes
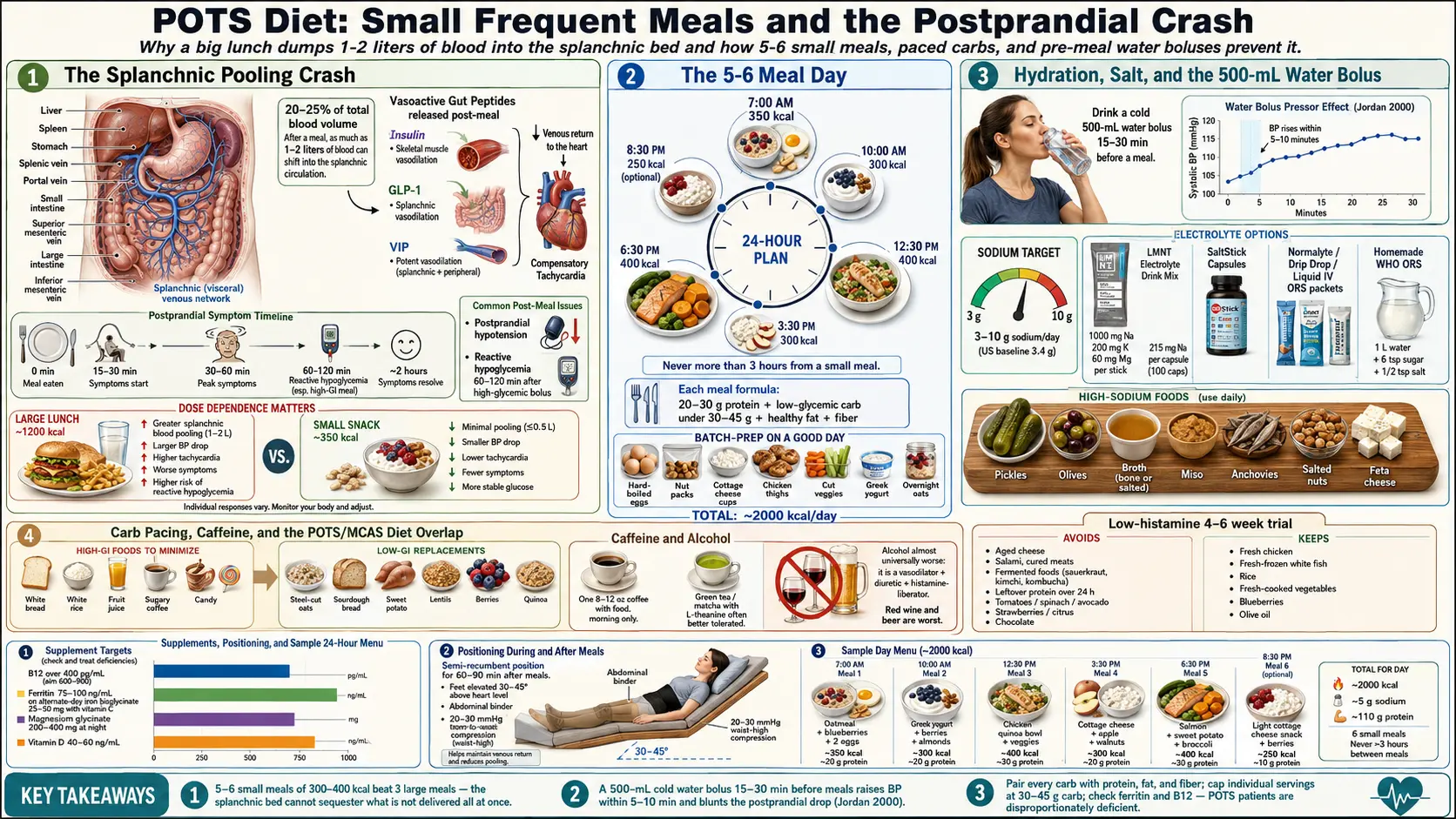
If you have POTS and you have noticed that a big lunch makes you want to lie on the floor for two hours, you are not imagining it and you are not lazy. Eating — especially a large, carb-heavy meal — is one of the most reliable symptom triggers in postural orthostatic tachycardia syndrome. The reason is plumbing: after a meal, your gut demands an extra 1–2 liters of blood to handle digestion, and that blood has to come from somewhere. In a healthy person, the autonomic nervous system tightens the peripheral vessels to compensate. In POTS, that compensation is broken, blood pools in the splanchnic (abdominal) circulation, and your heart rate rockets upward trying to keep your brain perfused. The result is the classic postprandial crash: lightheaded, foggy, tachycardic, exhausted, sometimes nauseous, sometimes pre-syncopal.
The good news is that diet is one of the few POTS levers you control entirely. This article walks through the eating pattern most POTS clinics (Mayo, Vanderbilt, Johns Hopkins, Cleveland Clinic) now recommend — small frequent meals, paced carbs, protein at every meal, aggressive hydration and salt, and a few specific tricks (positioning, compression, caffeine timing) that blunt the crash when it happens.
Table of Contents
- Why Eating Crashes You: The Splanchnic Pooling Problem
- Small Frequent Meals: The 5–6 Meal Day
- Low-Glycemic Carb Pacing and Why Heavy Carbs Wreck POTS
- Protein at Every Meal
- Hydration Timing: Before, Not During, Meals
- Electrolytes and the 3–10 g Salt Target
- Caffeine and Alcohol: The Nuanced Rules
- Histamine-Lowering Overlap for POTS/MCAS
- Supplements, Gastroparesis Overlap, and Positioning
- Food Journal, Trigger Foods, and a Sample 24-Hour Menu
- Key Research Papers
- PubMed Topic Searches
- Connections
- Featured Videos
Why Eating Crashes You: The Splanchnic Pooling Problem
The splanchnic circulation is the network of veins draining your stomach, small intestine, large intestine, liver, and spleen. Under normal digestion, roughly 20–25% of your total blood volume temporarily sequesters there to support absorption. In a healthy autonomic system, arterioles in the legs and arms constrict to maintain blood pressure. In POTS, that sympathetic constriction is either delayed, blunted, or paradoxical — and in the hyperadrenergic subtype, the system over-corrects with a surge of norepinephrine that spikes heart rate without actually fixing the pooling.
The effect is dose-dependent: the bigger the meal, the bigger the crash. A 1200-kilocalorie lunch demands more splanchnic blood than a 350-kcal snack. Carbohydrates worsen the effect because they trigger release of vasoactive gut peptides — particularly insulin, glucagon-like peptide-1 (GLP-1), and vasoactive intestinal peptide (VIP) — all of which are vasodilators. Insulin specifically causes skeletal-muscle vasodilation, which in a POTS patient compounds the pooling already happening in the abdomen. This is the mechanism of postprandial hypotension, and it is so reliable that a meal challenge can be used diagnostically.
The crash typically starts 15–30 minutes after eating, peaks around 30–60 minutes, and can last two hours. If your symptoms worsen every afternoon, track what you had for lunch before blaming the time of day.
Small Frequent Meals: The 5–6 Meal Day
The single most effective dietary change for POTS is eating 5 to 6 small meals per day of roughly 300–400 kilocalories each instead of three large meals. Smaller meals mean less blood shunted to the gut at any one time and a milder postprandial dip. Most patients notice a measurable difference within a week.
Practical structure:
- 7:00 AM — Meal 1 (breakfast, ~350 kcal)
- 10:00 AM — Meal 2 (mid-morning snack-meal, ~300 kcal)
- 12:30 PM — Meal 3 (early lunch, ~400 kcal)
- 3:30 PM — Meal 4 (afternoon, ~300 kcal)
- 6:30 PM — Meal 5 (early dinner, ~400 kcal)
- 8:30 PM — Meal 6 (light evening, ~250 kcal) — optional if you tolerate
Total daily intake for most adult women lands around 1800–2100 kcal, for most adult men 2200–2600 kcal. The target is steady energy, not weight loss. Many POTS patients are already underweight from food avoidance because eating feels miserable; under-eating worsens POTS by reducing blood volume and muscle mass.
If a six-meal day feels like constant cooking, batch-prep on a good day: hard-boiled eggs, pre-portioned nut packs, cottage cheese cups, cooked chicken thighs, cut vegetables, Greek yogurt, overnight oats. The point is not gourmet — the point is never being more than three hours from your next small meal.
Low-Glycemic Carb Pacing and Why Heavy Carbs Wreck POTS
Large carbohydrate boluses are the single worst meal pattern for POTS. Two things happen at once:
- Splanchnic pooling (as above) from the sheer volume of high-glycemic food demanding digestive blood flow.
- Reactive hypoglycemia: a rapid carb dump triggers a large insulin release. In POTS patients, whose autonomic counter-regulation is already impaired, blood sugar can then overshoot downward 60–120 minutes later, producing shakiness, sweating, tachycardia, and the fog of a full crash on top of the postprandial one.
The solution is low-glycemic carb pacing: pair every carbohydrate with protein, fat, and fiber, and keep individual carb servings under roughly 30–45 grams per meal.
High-glycemic foods to minimize or time carefully:
- White bread, white rice, white pasta eaten alone
- Sugary cereals, granola bars, pastries
- Fruit juice and soda (a glass of orange juice is a carb grenade)
- Large portions of potatoes without fat or protein alongside
- Candy, desserts, sweetened coffee drinks
Low-glycemic replacements that POTS patients tolerate well:
- Steel-cut or rolled oats (not instant) with nuts and Greek yogurt
- Sourdough or 100% whole-grain bread with butter or nut butter
- Sweet potato with olive oil and protein
- Beans, lentils, and chickpeas
- Berries, apples, pears (whole fruit, not juice)
- Quinoa and barley
Protein at Every Meal
Aim for 20–30 grams of protein at every meal, 10–15 grams at each snack. Protein has three advantages for POTS:
- It digests more slowly than carbs, flattening the blood-sugar and blood-pressure curves.
- It supports plasma volume through the amino acid pool needed to maintain albumin.
- It blunts gut peptide surges that drive splanchnic pooling.
Reliable protein sources: eggs, Greek yogurt, cottage cheese, chicken, turkey, fish (salmon and sardines are excellent — see salmon and sardines), tofu and tempeh if tolerated, whey or pea protein powder in smoothies, beef, pork, lentils, and hemp seeds. If MCAS is part of the picture (see the POTS/MCAS/EDS triad article), lean toward fresh, low-histamine proteins like freshly cooked chicken, turkey, and white fish and away from aged, smoked, or fermented options.
Hydration Timing: Before, Not During, Meals
POTS patients need a lot of fluid — most guidelines recommend 2.5–3 liters per day of total fluid intake — but when you drink matters almost as much as how much. Two rules:
Rule 1: Drink a large bolus 15–30 minutes before meals. A classic POTS trick is the 500-mL water bolus: chugging half a liter of cold water raises blood pressure within 5–10 minutes and blunts the subsequent postprandial drop. This is a well-documented phenomenon (Jordan et al. 2000) and is a free, drug-free way to protect yourself from a meal.
Rule 2: Minimize fluids during the meal itself. Drinking a lot of water during eating dilutes gastric contents, delays gastric emptying (especially in patients with comorbid gastroparesis), and can worsen the post-meal drop. Small sips to wash food down are fine; an entire 20-ounce tumbler is not.
Sip steadily between meals rather than chugging enormous volumes all at once far from food. Track intake for a week using a marked water bottle or an app — most POTS patients discover they are under 2 liters a day and are shocked.
Electrolytes and the 3–10 g Salt Target
Plain water alone will not expand plasma volume. You need sodium. Most autonomic specialists recommend 3 to 10 grams of sodium per day for POTS patients without contraindications such as kidney disease or certain heart conditions — confirm your personal target with your cardiologist or autonomic specialist before pushing salt high. For context, the average American eats around 3.4 g of sodium per day, so a POTS target often means adding 3–7 g above baseline.
Practical electrolyte strategies patients actually use:
- LMNT — each stick contains 1000 mg sodium, 200 mg potassium, 60 mg magnesium, no sugar. Strong flavors; many POTS patients tolerate this well when sweet drinks make them worse.
- SaltStick — capsules delivering 215 mg sodium plus potassium, calcium, magnesium. Good for people who cannot drink more fluid but need more salt.
- Normalyte / Drip Drop / Liquid IV — ORS-style (oral rehydration solution) packets based on the WHO formula that pairs sodium with small amounts of glucose to drive intestinal absorption. Liquid IV is sweeter; Normalyte matches WHO ratios more closely.
- Homemade ORS — 1 liter water + 6 level teaspoons sugar + ½ teaspoon salt. Cheap, effective, unsexy. A pinch of lite salt adds potassium.
- Salt-loading food — pickles, olives, broth, miso, anchovies, salted nuts, cottage cheese, feta, and adding a generous pinch of salt to eggs, avocado, and vegetables. Bone broth with added salt before getting out of bed is a morning standby.
See the dedicated salt and hydration protocol article for the full titration plan, including how to introduce salt gradually to avoid bloating, and when to consider IV saline infusions for severe cases.
Caffeine and Alcohol: The Nuanced Rules
Caffeine is the single most individual variable in a POTS diet. Roughly one-third of patients tolerate it and even use it strategically (a morning cup can blunt orthostatic symptoms via mild vasoconstriction); one-third get a nasty tachycardia spike and feel worse; one-third are mixed. The only way to know is a structured trial: hold caffeine for two weeks, then reintroduce one small cup in the morning with food and note your heart rate and symptoms for three days. If it helps, keep it; if it flares you, drop it.
Rules of thumb when you do use caffeine:
- Never on an empty stomach — pair with breakfast.
- Morning only; afternoon caffeine worsens the sleep fragmentation that feeds the POTS cycle.
- Cap at one 8–12 oz cup (about 80–120 mg caffeine); energy drinks and pre-workouts are almost universally a mistake.
- Green tea and matcha are often better tolerated than coffee because they pair caffeine with L-theanine, which modulates the sympathetic response.
Alcohol is simpler: almost every POTS patient does worse with it. Alcohol is a vasodilator, a diuretic, and a histamine-liberator — a triple hit for POTS and especially for anyone with MCAS overlap. Red wine, beer, and champagne are worst; clear distilled spirits (vodka, tequila) are slightly less histamine-loaded but still pull fluid and dilate vessels. Most patients find life noticeably better alcohol-free and at minimum should keep to a single drink with food and a full glass of electrolyte water alongside.
Histamine-Lowering Overlap for POTS/MCAS
A large fraction of POTS patients — estimates range from 30% to more than 60% in hyperadrenergic cohorts — have comorbid mast cell activation syndrome (MCAS). For these patients, certain foods can trigger a mast cell flare and a POTS crash simultaneously, because histamine itself is a vasodilator and a tachycardia driver. A low-histamine diet trial for 4–6 weeks is a reasonable low-cost experiment if eating reliably makes you feel awful even when portion sizes are small.
High-histamine foods to minimize during a trial:
- Aged cheeses (cheddar, parmesan, blue)
- Cured, smoked, or fermented meats (salami, prosciutto, bacon, hot dogs)
- Fermented foods (sauerkraut, kimchi, kombucha, soy sauce, miso, vinegar)
- Leftover protein stored more than 24 hours (histamine accumulates)
- Tomatoes, spinach, eggplant, avocado
- Strawberries, citrus, pineapple (histamine liberators even if not high themselves)
- Chocolate, nuts (especially walnuts and cashews)
- Alcohol (all forms)
Better-tolerated staples for a low-histamine trial: freshly cooked chicken or turkey (not leftover), fresh-frozen white fish, rice, quinoa, oats, most fresh-cooked vegetables (carrots, zucchini, sweet potato, broccoli, lettuce), fresh apples, pears, blueberries, olive oil, coconut oil, and fresh herbs. See the POTS-MCAS-EDS triad article for the full MCAS picture.
Supplements, Gastroparesis Overlap, and Positioning
Key supplements to check. POTS patients are disproportionately deficient in a few nutrients that directly affect autonomic tone and blood volume:
- Vitamin B12 — target serum B12 > 400 pg/mL; many POTS patients feel meaningfully better at 600–900. Methylcobalamin 1000 mcg daily sublingually is a common starting dose.
- Iron and ferritin — ferritin below 50 ng/mL worsens POTS symptoms even when hemoglobin is normal. Most autonomic specialists aim for ferritin 75–100 ng/mL minimum, higher in menstruating patients. Iron bisglycinate 25–50 mg taken with vitamin C, on alternate days (not daily — alternate-day dosing absorbs better and is gentler on the gut).
- Magnesium — magnesium glycinate 200–400 mg at night supports sleep and may reduce adrenergic surges. Citrate works but can loosen stools.
- Vitamin D — aim for 40–60 ng/mL 25-OH vitamin D.
Check levels before megadosing. Iron in particular is dangerous to take blind.
Gastroparesis overlap. Slow gastric emptying is extremely common in POTS — some series report it in more than half of patients — and it makes every dietary rule above more urgent. If meals feel "stuck," if you are full for hours after a small portion, or if nausea dominates, talk to your gastroenterologist about a gastric-emptying study. Management includes smaller meals (already your plan), lower-fat and lower-fiber content at individual meals (fat and fiber slow emptying further), well-chewed food, and in some cases prokinetics like low-dose erythromycin, prucalopride, or metoclopramide.
Positioning after eating. Do not lie flat immediately after a meal (reflux) and do not stand rigidly in the kitchen (pooling). The optimal posture is semi-recumbent with legs elevated — a recliner, couch with feet up, or bed with the head at 30–45 degrees — for 30–60 minutes after larger meals. Wearing compression stockings (20–30 mmHg or higher, waist-high ideal) or an abdominal binder during and after meals reduces splanchnic pooling mechanically and is one of the highest-leverage non-drug interventions available. See the compression and exercise program article for garment selection.
Food Journal, Trigger Foods, and a Sample 24-Hour Menu
Keep a food and symptom journal for at least two weeks. Column one: time and food eaten. Column two: fluid and sodium intake. Column three: standing heart rate at 0, 30, 60, and 120 minutes after the meal (a cheap pulse oximeter or a smartwatch works). Column four: symptoms. After two weeks, patterns emerge that no clinician can predict for you.
Common individual trigger foods reported across POTS cohorts:
- Large pasta portions, pizza, heavy sandwiches, rice bowls with sauce
- Sugary coffee drinks (double hit: caffeine + sugar bolus)
- Soda and fruit juice on an empty stomach
- Buffets and holiday meals (sheer volume)
- Processed meats (histamine + sodium often paired with low volume of actual food)
- High-fat fried meals that sit in the stomach for hours
Sample 24-hour POTS-friendly menu (~2000 kcal, ~5 g sodium, ~30 g fiber, ~110 g protein):
- 7:00 AM — wake. 500 mL cold electrolyte water (1 LMNT or equivalent) sipped over 15 minutes while still seated, before standing.
- 7:30 AM — Meal 1. 2 eggs scrambled in olive oil with a pinch of salt, ½ avocado (skip if low-histamine trial), 1 slice sourdough, ½ cup blueberries. One small coffee with food if tolerated.
- 10:00 AM — Meal 2. Greek yogurt (6 oz, full-fat) with 1 tablespoon chia seeds and a small apple. 8 oz water with a pinch of salt.
- 12:15 PM — pre-lunch water bolus. 500 mL cold water or electrolyte drink.
- 12:45 PM — Meal 3 (early lunch). 4 oz grilled chicken thigh, 1 cup cooked quinoa with olive oil, steamed broccoli, pickle spear or olives for salt. Minimal fluid with the meal; small sips only.
- 1:15 PM — post-lunch position. Recliner with feet up 30–45 minutes; compression stockings on.
- 3:30 PM — Meal 4. Cottage cheese (½ cup) with a handful of salted almonds and a pear. 8 oz electrolyte water.
- 6:00 PM — pre-dinner water bolus. 500 mL water with a pinch of salt.
- 6:30 PM — Meal 5. 4–5 oz baked salmon, 1 small roasted sweet potato with olive oil and salt, side salad with olive oil and vinegar (skip vinegar on low-histamine trial).
- 8:30 PM — Meal 6 (optional). Small bowl of steel-cut oats with a tablespoon of almond butter and a sprinkle of cinnamon. Magnesium glycinate 200–400 mg.
- Throughout day: total fluid target 2.5–3 L, total sodium 4–6 g depending on your prescribed range.
This is a starting template, not a prescription. Adjust portion size to your body, swap proteins to what you tolerate, and iterate from the journal data. The principle is what matters: small, paced, protein-anchored, low-glycemic, well-hydrated, well-salted, and supported by compression and positioning around the meal itself.
Key Research Papers
- Low PA, Sandroni P, Joyner M, Shen W-K. Postural tachycardia syndrome (POTS). Mayo Clin Proc. 2009;84(12):1131–1139.
- Raj SR. Postural tachycardia syndrome (POTS). Circulation. 2013;127(23):2336–2342.
- Jordan J, Shannon JR, Black BK, et al. The pressor response to water drinking in humans: a sympathetic reflex? Circulation. 2000;101(5):504–509.
- Jansen RWMM, Lipsitz LA. Postprandial hypotension: epidemiology, pathophysiology, and clinical management. Ann Intern Med. 1995;122(4):286–295.
- Fu Q, Levine BD. Exercise and non-pharmacological treatment of POTS. Auton Neurosci. 2018;215:20–27.
- Sheldon RS, Grubb BP, Olshansky B, et al. 2015 Heart Rhythm Society Expert Consensus Statement on the Diagnosis and Treatment of Postural Tachycardia Syndrome. Heart Rhythm. 2015;12(6):e41–e63.
PubMed Topic Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on POTS, postprandial physiology, and dietary management:
- POTS and diet
- Postprandial hypotension
- Splanchnic pooling and orthostatic intolerance
- Water bolus pressor response
- POTS, salt loading, and plasma volume
- POTS and mast cell activation (MCAS)
- POTS and gastroparesis overlap
- POTS, iron deficiency, and ferritin
- POTS, compression garments, and abdominal binders
- Reactive hypoglycemia and autonomic dysfunction
Connections
- POTS Overview
- Compression and Exercise Program
- Salt and Hydration Protocol
- POTS-MCAS-EDS Triad
- Medications Guide
- POTS Subtypes
- Vagus Nerve and Autonomic Retraining
- Low-Dose Naltrexone for POTS
- Tilt Table and NASA Lean Test
- Mast Cell Activation Syndrome (MCAS)
- Ehlers-Danlos Syndrome
- Magnesium
- Salmon
- Sardines
- Potassium
- Olive Oil