PTLDS and the “Chronic Lyme” Controversy
If you are reading this, you or someone you love is probably still suffering long after a course of antibiotics was supposed to fix things. Your fatigue, pain, brain fog, and the erosion of the life you used to lead are real. This page will not dismiss that suffering, and it will not sell you a cure. What it will do is walk honestly through what is known, what is disputed, and what actually helps.
Table of Contents
- What PTLDS Actually Is
- What “Chronic Lyme” Means to Different People
- The Two Camps — IDSA vs. ILADS
- Four Major Antibiotic Trials
- Proposed Mechanisms for PTLDS
- What Actually Helps
- What Doesn’t Help — and May Harm
- Ruling Out PTLDS Mimics
- How to Talk to Your Doctor
- Finding a PTLDS-Literate Clinician
- Insurance and Disability
- Mental Health and Validation
- Natural History and Prognosis
- What Not to Do
- Key Research Papers
- Connections
- Featured Videos
What PTLDS Actually Is
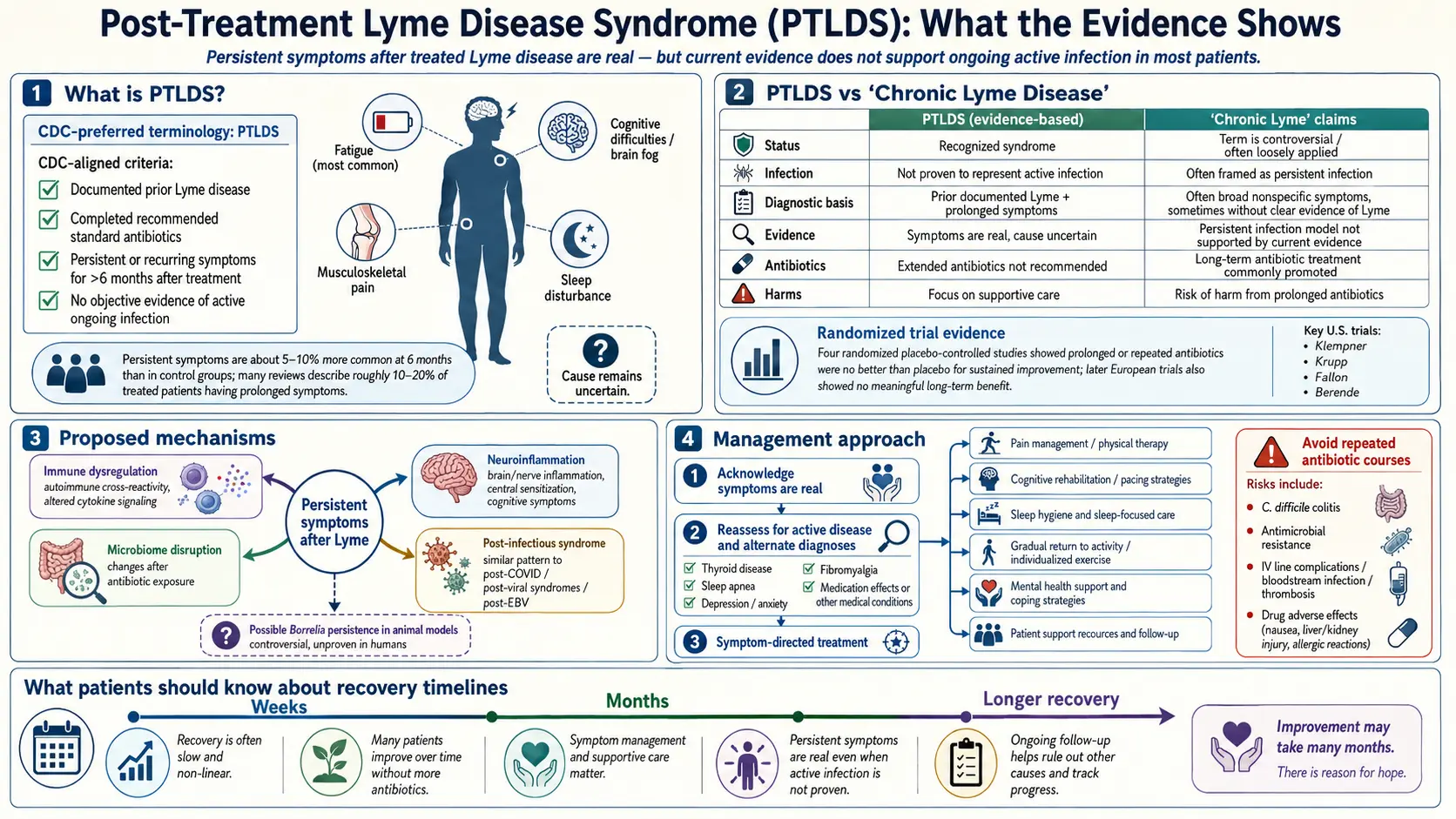
Post-Treatment Lyme Disease Syndrome (PTLDS) is a clinically defined syndrome: a constellation of persistent fatigue, widespread musculoskeletal pain, and cognitive difficulty that lasts more than six months after an adequate antibiotic course for documented Lyme disease. The IDSA case definition requires prior documented Lyme (positive two-tier serology, physician-observed erythema migrans rash, or an objective manifestation like Lyme arthritis or neuroborreliosis), completion of a standard antibiotic course, and functionally significant symptoms persisting at least six months.
Best estimates suggest 10–20% of treated patients develop PTLDS. With roughly 476,000 U.S. Lyme diagnoses annually (CDC estimate), even the low end means tens of thousands of new cases each year.
PTLDS is a real entity, recognized by the CDC, IDSA, AAN, and NIH. The controversy is not whether these patients are sick, but why and what to do about it.
What “Chronic Lyme” Means to Different People
“Chronic Lyme disease” is not a single diagnosis. It is an umbrella label that gets applied to at least four very different groups of patients, and much of the public argument happens because people are talking past each other about which group they mean.
- Group 1: PTLDS. Documented prior Lyme, treated, now has persistent symptoms. Real, recognized, and the focus of most legitimate research.
- Group 2: Untreated or under-treated Lyme. Patients with objective, ongoing Lyme manifestations (Lyme arthritis, neuroborreliosis) who were missed or inadequately treated. These patients usually respond to a proper antibiotic course.
- Group 3: Chronic multisystem illness without evidence of prior Lyme. Patients with fatigue, pain, and cognitive symptoms, negative Lyme serology, no clear exposure history, who have been told by a clinician that they have “chronic Lyme.” This is the most contested group and the one most vulnerable to unvalidated testing and indefinite antibiotic courses.
- Group 4: Tick-borne co-infection not fully addressed. Babesia, Bartonella, Anaplasma, or Ehrlichia that was never diagnosed or treated alongside Lyme.
The term “chronic Lyme” is contested because it collapses all four groups into one label, which then gets used to justify one treatment (long-term antibiotics) for patients with very different underlying problems. PTLDS is a precise term. “Chronic Lyme” is not.
The Two Camps — IDSA vs. ILADS
Two professional societies issue competing guidelines, and patients often end up choosing sides without knowing what each camp actually claims.
IDSA, joined by the AAN and ACR in 2020, holds that a 10–28 day course of doxycycline, amoxicillin, or cefuroxime cures most Lyme infections; that persistent symptoms after treatment are not caused by ongoing Borrelia infection in most patients; and that long-term antibiotic courses do not help and cause harm. This is backed by the four major randomized trials (below) and by culture, PCR, and xenodiagnosis data failing to recover viable spirochetes from most PTLDS patients. Where IDSA overreaches: it has at times sounded dismissive of PTLDS suffering, and early guidelines underplayed the fraction of patients who remain ill.
ILADS argues that standard serology misses a meaningful fraction of cases; that Borrelia can persist as slow-growing or dormant “persister cells” after antibiotics; and that some chronically ill patients benefit from longer or combination courses. ILADS has a point about persister biology — in vitro and some animal studies show antibiotic-tolerant subpopulations. Where ILADS overreaches: the leap from in vitro persisters to months of IV ceftriaxone plus oral combinations is not supported by human trials, and ILADS-aligned clinics often use non-validated tests (CD57, non-standard Western blot criteria) to justify treatment.
A careful clinician can hold both truths: PTLDS is real and poorly understood, and long-term antibiotics are not the answer for most patients.
Four Major Antibiotic Trials
The most important thing to know about long-term antibiotics for PTLDS is that the question has been rigorously tested. Four randomized placebo-controlled trials, funded by the NIH and published in peer-reviewed journals, give consistent answers.
- Klempner 2001 (NEJM). Two parallel trials of 30 days IV ceftriaxone then 60 days oral doxycycline vs. placebo. No significant improvement in quality of life. Adverse events common, including thrombus and line infection.
- Krupp STOP-LD 2003 (Neurology). 28 days IV ceftriaxone vs. placebo for post-Lyme fatigue. Modest fatigue improvement at 6 months; no improvement in cognition or pain. Three serious adverse events including one fatal pulmonary embolism.
- Fallon 2008 (Neurology). 10 weeks IV ceftriaxone vs. placebo for post-Lyme cognitive dysfunction. Transient cognitive improvement at 12 weeks, lost by 24 weeks. Significant adverse events including gallbladder complications and one sepsis death.
- Berende PLEASE 2016 (NEJM). The Dutch trial — largest and most recent. 281 patients randomized to 12 weeks of doxycycline, clarithromycin-plus-hydroxychloroquine, or placebo after a 2-week ceftriaxone lead-in. No difference between any arm at 14, 40, or 52 weeks.
The consistent picture: modest or no lasting benefit, real harms. Documented harms in these trials and in case series include Clostridioides difficile colitis, central line bloodstream infections, gallstones from ceftriaxone, venous thromboembolism, and — rarely — death. The harms are not theoretical.
Proposed Mechanisms for PTLDS
If most PTLDS patients are not harboring active infection, what is driving symptoms? Several non-exclusive hypotheses are under active research.
- Persistent bacterial debris. Non-viable Borrelia fragments (peptidoglycan, DNA) may linger and drive immune activation after the spirochete is dead. Different from “chronic infection” — the bacteria are not replicating.
- Autoimmunity and molecular mimicry. Borrelia outer-surface proteins share sequences with human antigens (LFA-1, myelin components). Primed T cells cross-react with self. Leading explanation for antibiotic-refractory Lyme arthritis.
- Gut dysbiosis from the antibiotics themselves. Weeks of doxycycline disrupt the microbiome in ways that produce fatigue and cognitive symptoms.
- Central sensitization. The nervous system gets stuck in a pain-amplifying state; overlaps with fibromyalgia and ME/CFS.
- Missed co-infections. Babesia in particular causes persistent fatigue, night sweats, and air-hunger; it does not respond to doxycycline.
- Post-infectious fatigue as a pattern. The same syndrome follows Q fever, mono, Giardia. Lyme may be one trigger among many for shared downstream biology.
What Actually Helps
Evidence-based symptom management is unglamorous, incremental, and genuinely effective for most patients over time. Treat each symptom on its own terms rather than waiting for one master antibiotic to fix everything.
- Graded exercise and pacing. Start below the threshold where you crash; add a few minutes per week. For patients with post-exertional malaise, rigid pacing with a heart-rate monitor works better than ambitious graded exercise.
- Sleep optimization. Screen for sleep apnea with a home study — treating apnea often produces dramatic cognitive gains. Rigorous sleep hygiene, cool dark room, consistent wake time.
- CBT for chronic illness. This is not “it’s in your head.” CBT for chronic illness treats real secondary suffering — catastrophizing, activity avoidance, hopelessness — that layers on top of real biology and amplifies disability. Ask for a therapist experienced with chronic illness.
- Treat comorbid depression and anxiety. SSRIs, SNRIs, and — for pain-predominant patients — low-dose tricyclics (amitriptyline, nortriptyline) help both mood and sleep.
- Rule out mimics and co-infections. Babesia, Bartonella, Anaplasma, thyroid, B12, vitamin D, iron, EBV reactivation, sleep apnea, POTS, MCAS.
- Low-dose naltrexone (LDN). 1.5–4.5 mg at night. Case series in ME/CFS and fibromyalgia suggest benefit; reasonable trial given low cost and safety.
- Anti-inflammatory diet. Mediterranean-style whole foods; modest but replicated benefit in chronic pain and fatigue conditions.
- Physical therapy. A skilled PT addresses deconditioning without pushing patients into crashes.
What Doesn’t Help — and May Harm
The following interventions either lack evidence, have failed when rigorously tested, or carry real risk. The PTLDS patient community is a target-rich environment for expensive unproven therapies; be skeptical, especially when the pitch includes urgency and the price tag is large.
- Months of IV antibiotics without clear indication. Documented harms: C. difficile, line sepsis, thrombosis, gallstones, death. The four major trials found no durable benefit.
- Disulfiram. Repurposed on in vitro persister activity; real-world use has produced serious hepatotoxicity, psychosis, and peripheral neuropathy. No RCT evidence of benefit.
- “Herbal Lyme” megaprotocols. Cryptolepis, Japanese knotweed, cat’s claw. Some in vitro activity; no RCT evidence for PTLDS. Herbal is not automatically safe — liver injury and drug interactions are common.
- Hyperbaric oxygen at non-indicated doses. Small trials unreplicated; expensive, not covered by insurance.
- Bee venom therapy. Anecdotal; anaphylaxis risk.
- Colloidal silver. No evidence. Causes argyria (permanent blue-gray skin discoloration).
- Unvalidated “Lyme panels.” CD57 counts, non-standard Western blot interpretations, and bioresonance routinely produce false positives that justify expensive treatment.
Ruling Out PTLDS Mimics
The symptoms of PTLDS — fatigue, pain, cognitive difficulty — are nonspecific. Before accepting PTLDS as the whole explanation, make sure the following have been evaluated:
- Hypothyroidism — TSH, free T4, anti-TPO antibodies.
- Obstructive sleep apnea — home sleep study; the threshold for testing should be low.
- POTS (Postural Orthostatic Tachycardia Syndrome) — 10-minute active stand test or tilt-table; frequently overlaps with PTLDS.
- MCAS (Mast Cell Activation Syndrome) — flushing, hives, food reactions, GI symptoms; serum tryptase and urine methylhistamine/prostaglandins.
- Fibromyalgia — widespread pain, tender points, sleep disturbance; a clinical diagnosis.
- ME/CFS — post-exertional malaise as the defining feature.
- Depression with somatic features — not a diagnosis of exclusion, but a genuine diagnosis that coexists and is treatable.
- Vitamin B12, vitamin D, iron, ferritin — cheap, common, easily fixed.
- Celiac disease — tTG-IgA; fatigue and brain fog are common presentations.
How to Talk to Your Doctor
The most productive posture is collaborative: you are asking for each symptom to be evaluated on its own merits, not fighting about whether Lyme is the cause.
- Lead with specifics. “I have fatigue that doesn’t improve with rest, cognitive symptoms worse in the afternoon, and migrating joint pain” — not “I think I have chronic Lyme.”
- Ask for objective evaluation. Sleep study, thyroid panel, vitamin levels, stand test for POTS, cognitive screening.
- Bring a symptom log. Two weeks of daily 1–10 ratings for fatigue, pain, cognition, sleep.
- Ask about co-management. Infectious disease plus primary care plus, as needed, sleep medicine, cardiology (for POTS), and mental health.
- Accept partial help. A doctor who will treat your sleep apnea and depression but doesn’t prescribe long-term antibiotics is still a useful ally.
Finding a PTLDS-Literate Clinician
There are a small number of academic Lyme specialty clinics that combine research-grade evaluation with compassionate symptom management. These are the safest starting points:
- Johns Hopkins Lyme Disease Research Center (Baltimore, MD).
- Columbia University Lyme and Tick-Borne Diseases Research Center (New York, NY).
- Tufts Lyme Disease Initiative (Boston, MA).
- MGH Lyme Disease Clinic (Boston, MA).
A caution about “Lyme-literate MDs” (LLMDs): the label is self-applied and not credentialed. Some are thoughtful clinicians; many run cash-only practices, diagnose “chronic Lyme” at high rates based on non-validated tests, and prescribe long antibiotic or herbal protocols costing thousands per month. Warning signs: diagnosis made in one visit, reliance on non-CDC-criteria Western blots, urgency to start immediately, and reluctance to coordinate with your other physicians.
Insurance and Disability
PTLDS is recognized enough that disability claims can succeed, but the paperwork matters. Practical points:
- Documentation. A contemporaneous record of the original Lyme diagnosis is the foundation — request old records now if yours is thin.
- Functional measures. Reviewers want functional data — steps per day, hours worked, neuropsychological test scores — not symptom lists.
- Recognized ICD-10 codes. G93.32 (post-viral and related fatigue syndromes) and comorbid codes for fibromyalgia, depression, POTS as applicable.
- Short-term first. Short-term disability is easier to obtain and creates the paper trail for long-term disability or SSDI later.
- Be careful with unvalidated tests. A case built on non-CDC-criteria Western blots is weaker than one built on documented EM rash plus neuropsychological testing.
Mental Health and Validation
PTLDS patients carry one of the highest documented burdens of depression, anxiety, and social isolation in chronic disease research. This is not because the illness is psychiatric — it is because chronic invisible suffering, medical disbelief, lost work, and strained relationships would break anyone. Treating the mental-health dimension is not a concession that the illness isn’t real. It is a concession that you are carrying an enormous load.
Support groups can be life-saving and, in some online spaces, a source of misinformation and pressure toward unproven expensive treatments. Vet groups: do moderators permit science-based information as well as lived experience? Is there financial entanglement with specific clinicians or supplement brands? Are members encouraged to coordinate with mainstream medicine, or abandon it?
Natural History and Prognosis
This is the part most patients never get told clearly: most PTLDS patients improve. Longitudinal studies from Johns Hopkins and Columbia consistently find that the majority of well-defined PTLDS patients have substantial reduction in symptoms within 1 to 2 years after initial treatment. A minority have persistent symptoms at 5 years, and a smaller minority remain severely impaired long-term.
Prognostic factors that worsen outcomes: delayed initial treatment (symptoms present for months before diagnosis), disseminated disease at presentation (neurologic or cardiac involvement), higher initial symptom severity, co-infection with Babesia, and significant pre-existing mental-health or chronic-pain history. Prognostic factors that improve outcomes: early diagnosis and treatment, younger age, shorter initial symptom duration, absence of co-infection, and sustained engagement with rehabilitation (exercise, sleep, CBT).
The slope of improvement is often slow and uneven — measured in months, not days, with frequent temporary setbacks. That is consistent with the known biology and does not mean your treatment is failing.
What Not to Do
- Don’t spend thousands on unvalidated lab tests. The money is better put toward a sleep study, a good rheumatologist, and neuropsychological testing.
- Don’t accept long-term IV antibiotics without rigorous indication — meaning a documented ongoing infection or a study protocol with institutional oversight.
- Don’t abandon mainstream medicine. Even if your experience with one doctor was dismissive, the diagnostic infrastructure — sleep studies, tilt-tables, MRI, neuropsychological testing, endocrine panels — is where most actionable findings come from.
- Don’t interpret slow improvement as treatment failure. Recovery is measured in months.
- Don’t treat your illness as your whole identity. Staying connected to work, relationships, creative life, and purpose — in whatever reduced form is possible now — is itself therapeutic.
- Don’t give up. Most people in your situation get meaningfully better. The slope is slow, but it points up.
Key Research Papers
- Klempner MS, et al. Two controlled trials of antibiotic treatment in patients with persistent symptoms and a history of Lyme disease. N Engl J Med. 2001;345:85–92.
- Berende A, et al. Randomized trial of longer-term therapy for symptoms attributed to Lyme disease (PLEASE). N Engl J Med. 2016;374:1209–1220.
- Aucott JN. Posttreatment Lyme disease syndrome. Infect Dis Clin North Am. 2015;29(2):309–323.
- Lantos PM, et al. Clinical practice guidelines by IDSA, AAN, and ACR: 2020 guidelines for the prevention, diagnosis, and treatment of Lyme disease. Clin Infect Dis. 2021;72(1):e1–e48.
Live PubMed Searches
For further reading, the following PubMed topic searches return current peer-reviewed work on PTLDS biology, trials, and management:
- Post-treatment Lyme disease syndrome
- Chronic Lyme disease controversy
- Long-term antibiotics Lyme randomized trial
- Borrelia persister cells and antibiotic tolerance
- Lyme autoimmunity and molecular mimicry
- PTLDS and cognitive dysfunction
- Post-infectious fatigue syndromes
- Low-dose naltrexone in chronic fatigue and pain
Connections
- Lyme Disease Overview
- Erythema Migrans Rash
- POTS
- Fibromyalgia
- Chronic Pain
- MCAS
- Lyme Neuroborreliosis
- Prevention and Tick Removal
- Tick Bite First Aid
- Antibiotic Treatment Protocols
- Lyme Testing Explained
- Tick-Borne Co-Infections
- Chronic Fatigue Syndrome
- Fatigue
- Depression
- Arthritis
- Brain Fog
- Lyme Carditis